Arterial Spin Labelling Perfusion Changes in Persistent Migrainous Aura Without Infarction
Bhadra Sajeev Nair, Vandana Sudheer, Boby Varkey Maramattom

TL;DR
This paper discusses how a non-invasive MRI technique called ASL can detect blood flow changes in migraines with prolonged aura symptoms, helping distinguish them from strokes.
Contribution
The paper demonstrates ASL's effectiveness in identifying reversible perfusion changes in persistent migrainous aura without infarction.
Findings
ASL detected reversible perfusion changes in a patient with persistent migrainous aura.
ASL helps differentiate persistent migrainous aura from ischemic events.
ASL provides insights into the pathophysiology of migraine, such as cortical spreading depression.
Abstract
Migraine is a common disorder characterized by recurrent, usually unilateral, pulsatile headaches often accompanied by nausea, vomiting, photophobia, phonophobia, and fatigue. Visual aura is the most common of all aura symptoms in migraine patients. The aura and headache phases of migraine are caused by intracranial vasoconstriction and extracranial vasodilation, respectively. Migrainous aura without infarction refers to migraine aura symptoms that persist for an extended period of one week or longer without any evidence of infarction on imaging. Arterial spin labelling (ASL) is a non-invasive magnetic resonance imaging technique used to quantitatively assess cerebral blood flow. It can be used to track perfusion changes over the migraine cycle. This case report highlights the utility of ASL as a non-invasive tool to detect reversible perfusion changes in persistent migrainous aura,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
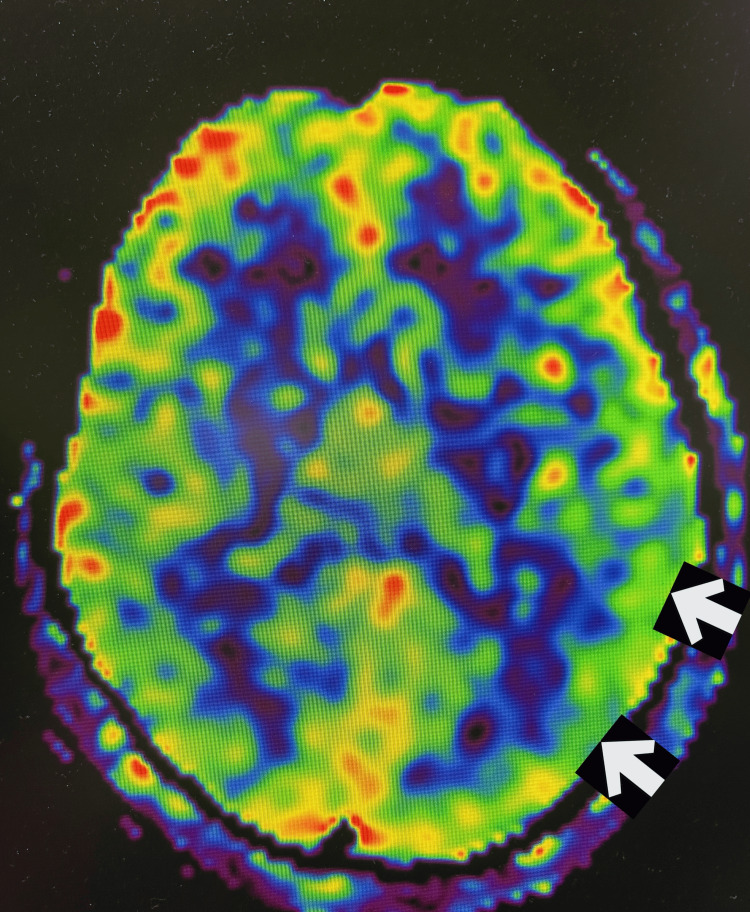 Figure 1
Figure 1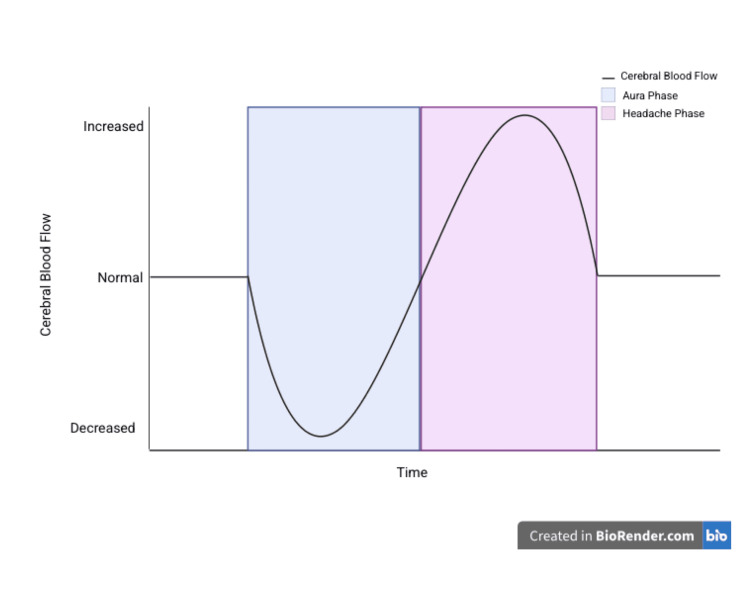 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies · Sympathectomy and Hyperhidrosis Treatments · Vestibular and auditory disorders
Introduction
Migraine is a prevalent neurological disorder characterized by recurrent, often unilateral headaches with a pulsatile quality, frequently accompanied by nausea, vomiting, generalized fatigue, and photophobia. As of 2025, the prevalence of persistent migraine without aura in India is estimated to be 10%-15%, with visual aura being the most common type (over 90% of aura cases) [1]. Scintillating or fortification scotoma, characterized by visual blurring, distortions, flickering, and shimmering, is most frequently observed. A primary dysfunction in central neuronal excitability is thought to underlie both aura and headache phases, with a propagating wave of reduced cerebral perfusion originating in the occipital cortex and advancing anteriorly. It resembles cortical spreading depolarization (CSD), wherein transient neuronal and glial depolarization suppresses neural activity and diminishes blood flow. This extent of hypoperfusion is sufficient to cause ischemic symptoms. Prolonged migrainous aura indicates prolonged cerebral hypoperfusion and may progress on to infarction. As the headache phase sets in, there is a relative hyperperfusion. Demographic trends show that migraines with aura most often affect females. Magnetic resonance imaging (MRI) helps rule out stroke mimics like transient ischemic attacks, seizure, reversible cerebral vasoconstriction syndrome, and intracranial hemorrhage. Arterial spin labelling (ASL) is a non-invasive MRI technique that quantitatively assesses cerebral blood flow that enables recognition of hypoperfusion or hyperperfusion states. ASL can be used to track perfusion changes over the migraine cycle. According to a 2024 study conducted among 1155 migraine patients, ASL done during the ictal phase showed hypoperfusion throughout aura symptoms, followed by hyperperfusion [2]. Herein, we present the case of a 32-year-old woman with chronic headache associated with persistent migrainous visual aura without infarction on MRI.
Case presentation
A 32-year-old female patient presented with a continuous flickering visual aura localized to the right upper quadrant of her visual field of the right eye, described as “seeing fireflies” for one week. The patient, however, did not experience headache. She had a history of chronic migraine, with headaches on more than 15 days every month for over three months, with aura. The patient did not report any regular medication, sensory changes, or menstrual abnormalities. Blood investigations, including complete blood count, kidney function tests, liver function test, lipid profile, blood glucose levels, thyroid profiles, and viral serology, were negative. Electroencephalogram (EEG) did not show epileptiform discharges. Arterial spin labelling during the ictal phase showed hypoperfusion of the left-sided parieto-occipital cortex as evidenced by asymmetry in signal (Figure 1). She was managed with beta-antagonists (oral propranolol 40 mg) and selective serotonin reuptake inhibitors (oral lasmiditan 50 mg), and her symptoms improved.
Arterial spin labelling imaging shows hypoperfusion of the left parieto-occipital cortex during the persistent aura phase (arrows)
Discussion
Persistent migrainous aura without infarction (PMA) is a rare complication of migraine with aura, in which typical aura symptoms such as visual disturbances, sensory changes, or speech difficulties persist for one week or longer without evidence of brain infarction on neuroimaging [1]. Migraine begins with intracranial vasoconstriction, leading to decreased blood flow in the occipital cortex, causing aura symptoms through a process known as cortical spreading depolarization (Figure 2). During CSD, endogenous calcitonin-gene related peptide (CGRP) is released from cortical tissue in a calcium-dependent manner, contributing to secondary vasodilation and neurogenic inflammation. However, this vasodilation is localized and insufficient to fully counteract the widespread vasoconstrictive response initiated by CSD. This results in transient neuronal inhibition and can mimic ischemia. If the aura is prolonged, it may lead to sustained hypoperfusion and potentially cerebral infarction. The headache phase follows, marked by extracranial vasodilation and relative cerebral hyperperfusion [3,4].
Time course of changes in cerebral blood flow in the migraine cycleImage credits: Created by authors on BioRender software (BioRender, Toronto)
This 32-year-old female patient presented to the outpatient department with isolated visual aura, that is, scintillating scotoma, persisting for one week in the absence of headache. A classical aura typically evolves and traverses the visual field, and recent studies suggest that approximately 20% of migraine patients may exhibit transient neurological symptoms without any accompanying headache. In a systematic case-based review article including 47 PMA cases, it was rightly pointed out that “accurate history taking is the most important diagnostic tool”. Clinical examinations and investigations in PMA would usually be normal [5,6].
Generally, auras without headache do not require treatment. The most effective drug in the treatment of PMA is lamotrigine [5,6]. An inhaled beta agonist, isoproterenol, may shorten the aura. Aura is now believed to result from neuronal depression, not ischemia, making vasodilators and triptans ineffective or harmful if used during this phase. Triptans, especially in oral forms, do not abort aura and may not prevent the headache even when injected. Calcium channel blockers, especially verapamil, are often very effective. Meclofenamate and naproxen are two rapid-acting non-steroidal anti-inflammatory drugs that are occasionally effective in reducing the duration of symptoms. Antiepileptic drugs such as valproic acid, gabapentin, and topiramate are also effective in reducing the frequency of PMA [7].
Conclusions
Migraine aura without headache should be considered in individuals experiencing recurrent, transient symptoms, particularly those of visual, neurological, or vestibular nature. While migrainous auras are typically vivid, scintillating, and dynamic, often manifesting as geometric patterns, ischemic visual disturbances are more commonly dark, static, and featureless in appearance. Our patient, who reported with a one-week history of scintillating scotoma, was diagnosed with persistent migrainous aura without infarction with the help of non-invasive ASL-MRI, which revealed hypoperfusion in the left parieto-occipital cortex. ASL perfusion imaging in migrainous aura without infarction reveals a reversible, biphasic blood flow pattern, initial hypoperfusion followed by hyperperfusion, that helps distinguish it from stroke, with PMA being a rare clinical entity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Visual aura in migraine: an analysis of 165 patients in a tertiary care hospital in North India J Neurosci Rural Pract Singla M Kale R Brar J Bhardwaj S 2732801220213392751810.1055/s-0040-1721624 PMC 8064847 · doi ↗ · pubmed ↗
- 2Perfusion imaging by arterial spin labeling in migraine: a literature review J Cereb Blood Flow Metab Schramm S Börner C Reichert M 1253127044202410.1177/0271678 X 241237733 PMC 1134272738483125 · doi ↗ · pubmed ↗
- 3Migraine Clinical Neurology, 8th Edition Greenberg DA Aminoff MJ Simon RP 151158 New York Mc Graw Hill Medical 2012 https://www.academia.edu/97588862/Clinical_Neurology_EIGHTH_EDITION
- 4Critical role of calcitonin gene-related peptide receptors in cortical spreading depression Proc Natl Acad Sci U S A Tozzi A de Iure A Di Filippo M 189851899010920122311219210.1073/pnas.1215435109 PMC 3503217 · doi ↗ · pubmed ↗
- 5Bilateral persistent ophthalmoplegia in a patient with migraine: persistent migraine aura without infarction?BMJ Case Rep Prakash S Prakash A Lodha D 014202110.1136/bcr-2021-242099 PMC 803067833827884 · doi ↗ · pubmed ↗
- 6Persistent migraine aura: new cases, a literature review, and ideas about pathophysiology Headache Thissen S Vos IG Schreuder TH Schreurs WM Postma LA Koehler PJ 129013095420142486314010.1111/head.12392 · doi ↗ · pubmed ↗
- 7Migraine aura without headache: benign, but a diagnosis of exclusion Cleve Clin J Med Kunkel RS 529534722005 https://www.ccjm.org/content/ccjom/72/6/529.full.pdf 1601829410.3949/ccjm.72.6.529 · doi ↗ · pubmed ↗