Indeterminate QuantiFERON Results in Pediatric Kawasaki Disease: Inflammatory Predictors and Diagnostic Implications
Koji Yokoyama, Mitsukazu Mamada

TL;DR
This study explores why TB tests often give unclear results in children with Kawasaki disease, linking it to inflammation and suggesting alternative diagnostic approaches.
Contribution
The study identifies specific inflammatory markers associated with indeterminate TB test results in pediatric Kawasaki disease patients.
Findings
Indeterminate QFT results were found in 20.4% of pediatric cases, with 80% linked to Kawasaki disease.
Higher C-reactive protein and lower serum albumin levels were observed in KD patients with indeterminate QFT results.
The study suggests considering alternative TB diagnostic tools for children with acute Kawasaki disease.
Abstract
Introduction Interferon-gamma release assays (IGRAs), such as the QuantiFERON®-TB Gold Plus (QFT), are widely used for tuberculosis (TB) screening in children. However, indeterminate QFT results remain a diagnostic challenge, particularly in patients with Kawasaki disease (KD), in whom systemic inflammation may transiently impair T-cell function. This study aimed to identify clinical and laboratory factors associated with indeterminate QFT results in pediatric patients, with a focus on KD. Methods We retrospectively analyzed 147 pediatric QFT tests performed at a tertiary medical center in Japan between September 2019 and May 2025. Clinical characteristics and laboratory parameters were compared between patients with indeterminate and negative QFT results. Subgroup analyses were conducted for children with KD. Results Among the 147 pediatric cases, 30 (20.4%) yielded indeterminate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
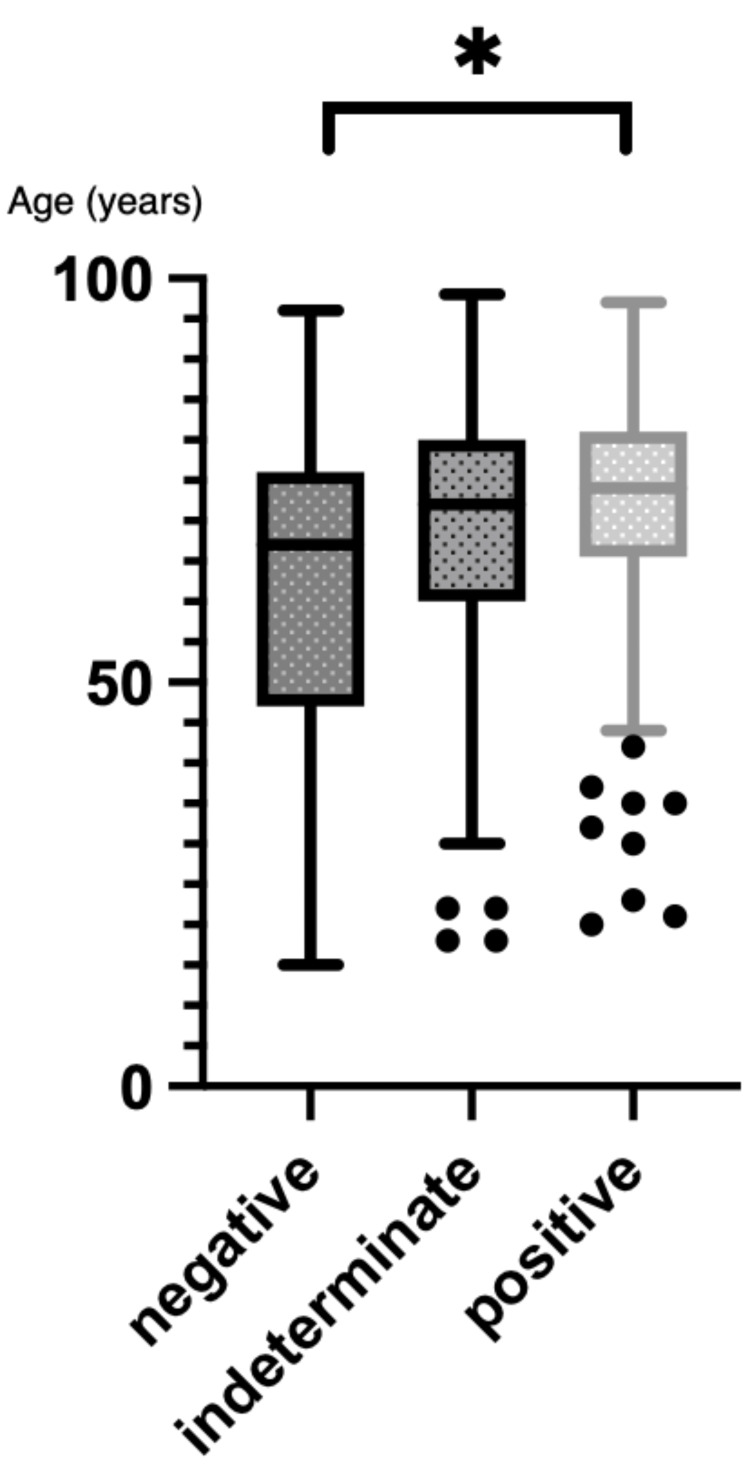 Figure 1
Figure 1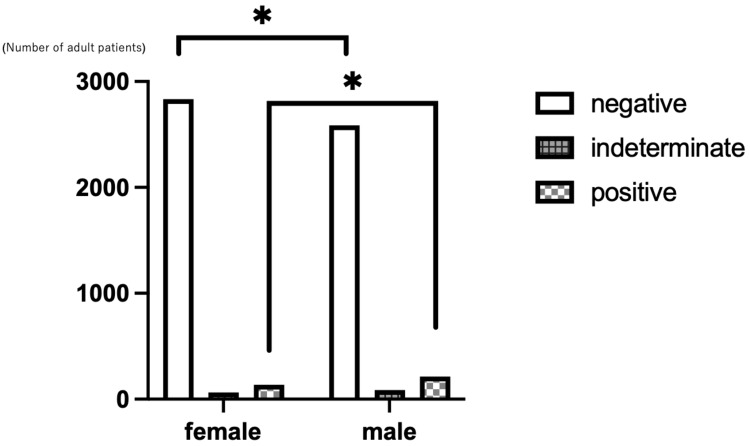 Figure 2
Figure 2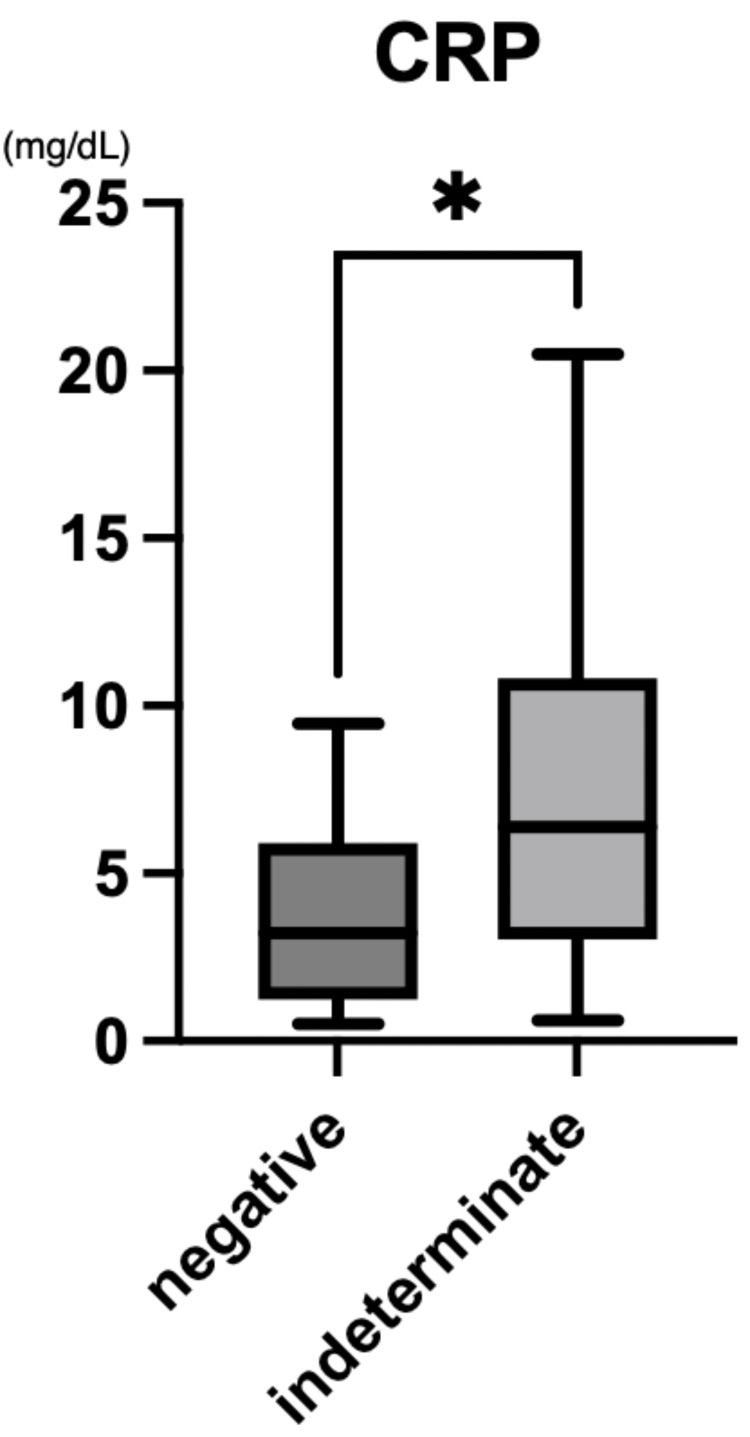 Figure 3
Figure 3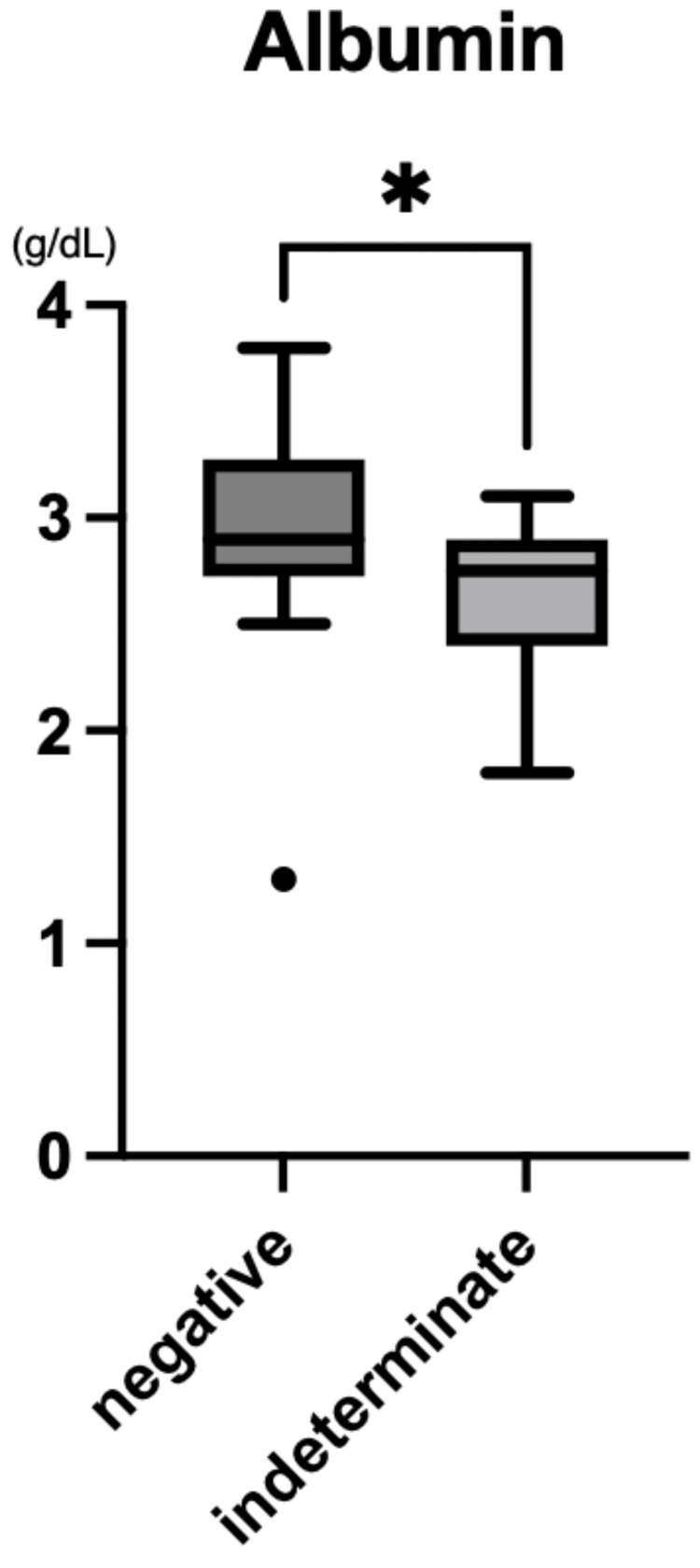 Figure 4
Figure 4| Clinical characteristics | n (%) |
| Corticosteroid use | 60 (45.1) |
| Immunosuppressive medication | 9 (6.8) |
| Kidney disease | 28 (21.1) |
| Rheumatic diseases | 11 (8.3) |
| Malignant disease | 9 (6.8) |
| Infectious disease※ | 7 (5.3) |
| Tuberculosis/nontuberculous mycobacteria | 5 (3.8) |
| Others | 4 (3) |
| Clinical diagnosis | n (%) |
| Juvenile idiopathic arthritis with corticosteroids | 2 (6.9) |
| Idiopathic nephrotic syndrome | 2 (6.9) |
| Kidney abscess | 1 (3.4) |
| ADEM | 1 (3.4) |
| Kawasaki disease | 23 (79.3) |
| Parameter | Unit | Reference range (typical) |
| WBC | ×10³/μL | 4.0-8.0 |
| Hemoglobin | g/dL | 11.5-14.5 |
| Platelet count | ×10⁴/μL | 15-45 |
| CRP | mg/dL | <0.3 |
| Serum albumin | g/dL | 3.8-5.0 |
| AST | U/L | <40 |
| ALT | U/L | <35 |
| BUN | mg/dL | 7-20 |
| Creatinine | mg/dL | 0.2-0.8 |
| Sodium | mmol/L | 135-145 |
| Potassium | mmol/L | 3.5-5.0 |
| PT | sec | 10-13 |
| Fibrinogen | mg/dL | 200-400 |
| D-dimer | μg/mL | <1.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Ultrasound in Clinical Applications · Bacterial Infections and Vaccines
Introduction
Interferon-gamma release assays (IGRAs), such as the QuantiFERON®-TB Gold Plus (QFT; Qiagen, Hilden, Germany), are widely used in tuberculosis (TB) screening, especially in children requiring immunosuppressive therapy. While TB remains a relevant health issue, this study focuses on the diagnostic behavior of QFT in pediatric patients with inflammatory conditions such as Kawasaki disease (KD). While the tuberculin skin test (TST) is used traditionally for TB screening, IGRAs are valuable alternatives because of their higher specificity and logistical advantages, particularly in Bacillus Calmette-Guérin (BCG)-vaccinated populations. However, it is important to note that QFT testing typically requires a blood sample of approximately 10 mL, which may pose a challenge in young pediatric patients, especially during the acute phase of illness. The QFT is one of the most widely used IGRAs, offering high sensitivity and specificity for Mycobacterium tuberculosis infection (including both latent and active forms), with validated performance even in pediatric cases [1]; however, indeterminate results pose a significant diagnostic challenge as they can complicate patient management and delay necessary interventions. This issue is more pronounced in young children, whose immature immune systems, susceptibility to acute inflammation, and nutritional vulnerabilities may compromise IGRA reliability. KD, a common type of pediatric vasculitis, is sometimes treated with corticosteroids or biologics when intravenous immunoglobulin (IVIG) is insufficient [2]. TB screening is recommended prior to initiating corticosteroids or biologics in cases of IVIG-resistant KD; however, the need for prompt treatment often precedes the availability of definitive screening results, complicating treatment decisions. The acute inflammatory milieu in KD is linked to impaired IGRA performance, as demonstrated by recent large-scale studies reporting high rates of indeterminate QFT results [3]. To date, there is no standardized approach to interpreting IGRA results in the setting of acute systemic inflammation, and clinicians often face diagnostic uncertainty when managing patients with indeterminate findings [4]. In countries such as Japan, where the incidence of KD is high and universal BCG vaccination is implemented [5,6], the reliability of QFT in pediatric inflammatory settings warrants particular attention. While several large-cohort studies demonstrate increased rates of indeterminate QFT results in KD cases, few have undertaken a systematic examination of the immunologic or clinical predictors of such outcomes in pediatric populations [7]. Therefore, understanding the factors associated with indeterminate QFT results in this population has important implications for clinical decision-making, particularly in IVIG-resistant KD cases where immunosuppressive therapy may be urgently required. We initially sought to assess QFT utility for TB screening in KD patients prior to immunosuppressive therapy. However, unexpectedly high rates of indeterminate results led us to investigate clinical and laboratory factors associated with QFT performance in this setting. This study aimed to identify clinical and inflammatory predictors of indeterminate QFT results in pediatric KD patients.
Materials and methods
This retrospective, single-center study enrolled patients who underwent QFT testing at the Japanese Red Cross Wakayama Medical Center, located in Wakayama City, Wakayama Prefecture, Japan, from September 2019 to May 2025. QFT testing was typically performed at the time of initial evaluation and prior to the administration of IVIG, especially in cases where second-line immunosuppressive therapy (e.g., corticosteroids or cyclosporine) was being considered. However, the exact timing of QFT testing relative to disease onset or treatment was not standardized and varied between patients depending on clinical urgency and logistical factors. The decision to perform QFT was made at the discretion of the treating physician based on clinical judgment and institutional practice. Blood samples were processed on the same day, and QFT assays were performed in accordance with the manufacturer's instructions (QuantiFERON®-TB Gold Plus, Qiagen), including incubation and interpretation protocols. Both adult and pediatric cohorts were examined, and subgroup analysis was performed for KD patients. As this was the only positive case, it was excluded from analysis due to the lack of a sufficient number of cases for meaningful comparison. Inflammatory, coagulation, and biochemical parameters were analyzed as variables. Continuous variables were compared using the Mann-Whitney U test, a nonparametric test that does not require an assumption of normality. Categorical variables were analyzed using the chi-squared test or Fisher's exact test, as appropriate. A p-value of <0.05 was considered statistically significant. In this cohort, QFT was used both as a pre-immunosuppressive screening tool and as part of differential diagnosis for suspected TB infection, reflecting its broad utility in pediatric clinical practice. Statistical analysis was conducted using GraphPad Prism version 10.4.2 (GraphPad Software, San Diego, California, United States). The Ethics Committee of the Japanese Red Cross Wakayama Medical Center approved this retrospective study (approval number: 1467), including a waiver of informed consent.
Results
Adult cohort
Among 6,045 adult QFT tests, 5,561 (92%) were negative, 351 (5.8%) were positive, and 133 (2.2%) were indeterminate. The positive group (median age 72; IQR: 68-80) was significantly older than the negative group (median age 60; IQR: 48-72; p=0.011). There was no significant age difference between the negative and indeterminate groups (median age 65; IQR: 56-79; p=0.144; Figure 1).
Age distribution of adult patients according to QFT resultsBox-and-whisker plots show median ages and IQR for patients with negative, positive, and indeterminate QFT results. Error bars represent 95% confidence intervals. Total patients: 6,045 (5,561 negative, 351 positive, and 133 indeterminate). QFT tests were conducted from 2019 and 2025.QFT: QuantiFERON®-TB Gold Plus; IQR: interquartile range
There was a significant difference in sex distribution among the groups (p<0.001), with females predominating in the negative group (52.3%) and males in the positive group (61.1%; Figure 2).
Sex distribution by QFT result in adult patientsBar graph showing the number of male and female patients in each QFT result category (negative, positive, and indeterminate). Total patients: 6,045 (3,007 males and 3,038 females). QFT tests were conducted from 2019 to 2025.QFT: QuantiFERON®-TB Gold Plus
Among the 133 indeterminate adult cases, 60 (45.1%) were receiving corticosteroids, and nine (6.8%) were treated with other immunosuppressive agents. Of the 64 indeterminate patients not receiving these therapies, the major underlying conditions were renal disease (28 cases), collagen vascular disease (11 cases), or malignancy (10 cases; Table 1).
Pediatric cohort
Among 147 pediatric QFT tests, 116 (78.9%) were negative, one (0.7%) was positive, and 30 (20.4%) were indeterminate. The single positive case involved a 56-month-old child who developed latent tuberculosis infection (LTBI) after recent travel from China and was excluded from statistical comparison due to its distinct epidemiological and clinical background. Further details regarding this case are provided in the Appendices [8]. There were no significant differences in age (p=0.22) or sex distribution (p=0.40) between the negative and indeterminate groups. Of the 30 pediatric patients, two had juvenile idiopathic arthritis (JIA; treated with corticosteroids), two had idiopathic nephrotic syndrome, one had a kidney abscess, and one had acute disseminated encephalomyelitis (ADEM). The remaining 24 cases (80%) were KD. Corticosteroids were not used in cases of nephrotic syndrome, kidney abscess, or ADEM (Table 2).
Subgroup analysis of non-KD cases was not performed because of the low number of such cases.
Subgroup analysis: Kawasaki disease
Among the 41 KD patients who underwent QFT testing, 24 were indeterminate and 16 were negative. The indeterminate group had significantly higher C-reactive protein (CRP) levels (median 5.65 mg/dL; IQR: 3.16-10.41) than the negative group (median 3.21 mg/dL; IQR: 1.48-5.39; p=0.016; Figure 3).
CRP levels in QFT-indeterminate and QFT-negative patients with Kawasaki diseaseBox-and-whisker plots show median values and IQR. CRP was measured in mg/dL. A statistically significant difference was observed between the two groups (p=0.016). Total KD patients analyzed: 40 (24 indeterminate, 16 negative). QFT tests were conducted between 2019 and 2025.QFT: QuantiFERON®-TB Gold Plus; CRP: C-reactive protein; IQR: interquartile range
Serum albumin levels were also significantly lower in the indeterminate group (median 2.75 g/dL; IQR: 2.40-2.90) than in the negative group (median 2.90 g/dL; IQR: 2.77-3.23; p=0.013; Figure 4).
Serum albumin levels in QFT-indeterminate and QFT-negative patients with Kawasaki diseaseBox-and-whisker plots show median values and IQR. Albumin was measured in g/dL. A statistically significant difference was observed between the two groups (p=0.013). Total KD patients analyzed: 40 (24 indeterminate, 16 negative). QFT tests were conducted between 2019 and 2025.QFT: QuantiFERON®-TB Gold Plus; IQR: interquartile range
There were no significant differences between the groups with respect to other laboratory parameters, including inflammatory, coagulation, hepatic, and renal markers. A detailed list of laboratory variables assessed is summarized in Table 3.
Discussion
In this study, we found a notably high frequency of indeterminate QFT results among pediatric patients with KD. Within this subgroup, elevated CRP levels (Figure 3) and decreased serum albumin concentrations (Figure 4) were significantly associated with indeterminate outcomes. These findings suggest that acute systemic inflammation during the active phase of KD may transiently suppress T-cell responsiveness, thereby impairing IGRA performance. Unlike patients with known immunosuppression or critical illness [4], the immune dysfunction in KD appears to be transient and inflammation-driven. This distinction has important diagnostic implications, particularly when TB screening is required before initiating immunosuppressive therapy [4,9].
Interpretation of inflammation-related mechanisms
In the acute phase of KD, hypoalbuminemia likely reflects increased vascular permeability rather than malnutrition, a hallmark of the disease's inflammatory pathology [10]. This phenomenon is driven by interleukin-6-mediated signaling and release of vascular endothelial growth factor and angiopoietin-like proteins, which contribute to albumin leakage and elevated CRP levels [10,11]. These inflammatory mediators may suppress T-cell function transiently and inhibit mitogen-induced production of interferon-gamma (IFN-γ), resulting in an indeterminate IGRA response [4,9]. Comparable mechanisms have been documented in patients within intensive care units and in individuals with systemic infections, providing further support for inflammation-induced T-cell hyporesponsiveness [4,9]. However, we acknowledge that our study did not include direct immunological measurements, such as T-cell function assays or cytokine profiling. As such, the proposed mechanistic explanations remain speculative and require validation through future studies incorporating targeted immunological analyses.
Implications for clinical practice and diagnostic strategies
These diagnostic limitations are particularly relevant when immunosuppressive therapy must be initiated before TB infection can be excluded definitively. In such cases, repeating IGRA testing after the resolution of the acute-phase response or selecting an alternative assay such as the T-SPOT.TB test which has been reported to be less susceptible to systemic inflammation due to its use of standardized cell counts and ELISPOT-based detection [12,13] may be considered as a future direction. However, we did not perform comparative testing in this study; therefore, this recommendation remains speculative. Based on these observations and previously published literature, we suggest several hypothesis-generating strategies that may improve TB screening accuracy in the context of acute KD, although these remain unvalidated in our study and warrant future investigation. First, the timing of IGRA testing should be optimized in accordance with the inflammatory state, particularly in IVIG-resistant cases that require urgent treatment [3,11]. Second, clinicians should consider alternative approaches when an indeterminate result is anticipated. The T-SPOT.TB assay has demonstrated resilience against inflammation-related interference [14,15], and adjunctive tools such as chest imaging and clinical risk stratification further support decision-making [16]. Microbiological testing methods, including nucleic acid amplification tests and gastric aspirate cultures, may also aid diagnosis in high-risk or symptomatic cases [17,18]. Lastly, the development of KD-specific diagnostic algorithms incorporating inflammatory biomarkers and treatment urgency is warranted to guide clinicians through indeterminate results. Similar strategies may prove useful in other pediatric conditions characterized by acute systemic inflammation and early immunosuppressive therapy, such as JIA [19,20]. Our findings underscore the importance of recognizing that systemic inflammation in KD can impair the performance of IGRA-based TB screening. In clinical practice, this means that a single indeterminate QFT result obtained during the acute phase of KD may not reliably reflect TB infection status. Clinicians should consider repeating the test during convalescence or integrating alternative assessments (e.g., history, imaging) before delaying immunosuppressive treatment based solely on indeterminate results. While CRP and albumin were significantly associated with indeterminate QFT outcomes in our cohort, their predictive utility has not been formally tested. Future studies are needed to evaluate whether these biomarkers can be incorporated into validated clinical decision tools.
This study has several limitations. First, its retrospective, single-center design and relatively small sample size may limit generalizability. Second, the timing of QFT testing in relation to disease phase or IVIG administration was not standardized, potentially affecting the results. Third, follow-up testing was not performed systematically in cases with indeterminate results, and clinical outcomes were not assessed. In addition, the study did not include direct comparisons with alternative assays such as T-SPOT.TB, nor did it assess imaging or microbiological diagnostic modalities. Although we discussed the potential advantages of T-SPOT.TB, its performance was not evaluated in this study; thus, any recommendations remain speculative. Furthermore, while our findings suggest inflammation-induced suppression of T-cell responsiveness, this mechanism remains hypothetical in the absence of direct immunological measurements. Lastly, the relatively small number of pediatric KD cases undergoing QFT testing may, in part, reflect ethical and practical concerns regarding blood sampling in young children. The QFT assay requires multiple milliliters of blood, which may limit its applicability in infants and toddlers where sampling volume is constrained. These limitations highlight the need for future prospective studies with larger cohorts, standardized testing protocols, immunological correlates, and outcome data to clarify the clinical utility of IGRAs in acute pediatric inflammatory diseases. Additionally, this study was exploratory in nature and should be considered hypothesis-generating. Future multicenter, prospective studies with follow-up of indeterminate cases will be needed to validate these preliminary findings and assess their clinical implications.
Conclusions
This study suggests that QFT may yield indeterminate results in children with KD during the acute inflammatory phase, which may reflect transient inflammation-induced T-cell suppression. Elevated CRP and decreased albumin levels were associated with indeterminate results, likely reflecting transient inflammation-induced T-cell suppression. To improve TB risk assessments in this population, clinicians should consider the timing of IGRA testing, alternative assays such as T-SPOT.TB, and adjunctive diagnostic tools. Furthermore, the development of KD-specific diagnostic algorithms incorporating inflammatory markers and treatment urgency may facilitate timely and accurate decision-making. These exploratory insights may help guide future screening protocol development for other pediatric inflammatory conditions requiring early immunosuppressive interventions. Implementing such considerations in clinical practice may help prevent diagnostic delays and optimize treatment decisions regarding children with acute inflammatory diseases. Although QFT may not serve as a definitive screening tool in acute KD, recognizing its diagnostic limitations and situations in which its results may be unreliable is critical for safe and timely clinical decision-making. Rather than validating QFT utility, our findings emphasize when its results should be interpreted with caution.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Performance of Quanti FERON-TB Gold Plus assays in paediatric tuberculosis: a multicentre PTBNET study Thorax Buonsenso D Noguera-Julian A Moroni R 2882967820233628382610.1136/thorax-2022-218929 · doi ↗ · pubmed ↗
- 2Overview of guidelines for the medical treatment of acute Kawasaki disease in Japan (2020 revised version) and positioning of plasma exchange therapy in the acute phase Pediatr Infect Dis J Mori M Matsubara T 03242202310.1097/INF.000000000000397437200509 · doi ↗ · pubmed ↗
- 3Performance of two interferon-gamma release assays for tuberculosis infection screening in Kawasaki children before immunosuppressive therapy Front Pediatr Chen H Zheng H Cui L 11625471120233727481610.3389/fped.2023.1162547 PMC 10232946 · doi ↗ · pubmed ↗
- 4Effects of acute critical illnesses on the performance of interferon-gamma release assay Sci Rep Huang CT Ruan SY Tsai YJ 19972620162680448710.1038/srep 19972 PMC 4726381 · doi ↗ · pubmed ↗
- 5Effect of BCG vaccination on childhood tuberculous meningitis and miliary tuberculosis worldwide: a meta-analysis and assessment of cost-effectiveness Lancet Trunz BB Fine P Dye C 1173118036720061661656010.1016/S 0140-6736(06)68507-3 · doi ↗ · pubmed ↗
- 6Epidemiologic features of Kawasaki disease in Japan: results of the 2009-2010 nationwide survey J Epidemiol Nakamura Y Yashiro M Uehara R 2162212220122244721110.2188/jea.JE 20110126 PMC 3798622 · doi ↗ · pubmed ↗
- 7Risk factors for indeterminate interferon-gamma release assay for the diagnosis of tuberculosis in children-a systematic review and meta-analysis Front Pediatr Meier NR Volken T Geiger M Heininger U Tebruegge M Ritz N 208720193119217510.3389/fped.2019.00208 PMC 6548884 · doi ↗ · pubmed ↗
- 8Treatment of latent tuberculosis infection in a Kawasaki disease patient receiving anti-tumor necrosis factor alpha (TNFα) therapy Cureus Yokoyama K Yakuo T Mamada M 016202410.7759/cureus.70407 PMC 1151938839473638 · doi ↗ · pubmed ↗