X‐Linked Hereditary Hydrocephalus Diagnosed in the Fetal Period With Adducted Thumb and a Novel L1CAM Variant: A Case Report
Ryosuke Horiuchi, Hiroshi Sato, Chinami Asai, Fumika Hamaguchi, Yu Takaishi, Kensuke Fujiwara, Yukari Atsumi, Yukiko Ando, Takahito Kawata, Kazuyo Kakui

TL;DR
A rare genetic condition causing fetal hydrocephalus was diagnosed through prenatal imaging and confirmed by a new mutation in the L1CAM gene.
Contribution
A novel L1CAM gene variant was identified in a case of X-linked hereditary hydrocephalus with prenatal imaging features.
Findings
Prenatal MRI detected fetal hydrocephalus and an adducted thumb, suggesting XLH.
A new frameshift variant in the L1CAM gene was confirmed through postnatal genetic testing.
Non-invasive prenatal testing in a subsequent pregnancy identified a female fetus without hydrocephalus.
Abstract
X‐linked hereditary hydrocephalus (XLH) is a congenital form of hydrocephalus caused by variants in the L1CAM gene on the X chromosome. Diagnosis is often made prenatally via ultrasound or magnetic resonance imaging (MRI), but specific features such as adducted thumbs are subtle and easily missed. We report a case in which prenatal MRI at 34 weeks gestation revealed fetal hydrocephalus and an adducted thumb, suggestive of XLH. Postnatal genetic testing confirmed a previously unreported frameshift variant in the L1CAM gene, c.2248dup (p.Tyr750LeufsTer36). The male infant required neurosurgical intervention and was also diagnosed with Hirschsprung's disease. Genetic testing confirmed that the mother was a heterozygous carrier. In a subsequent pregnancy, non‐invasive prenatal testing (NIPT) predicted a female fetus with no hydrocephalus. This case highlights the importance of thorough…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
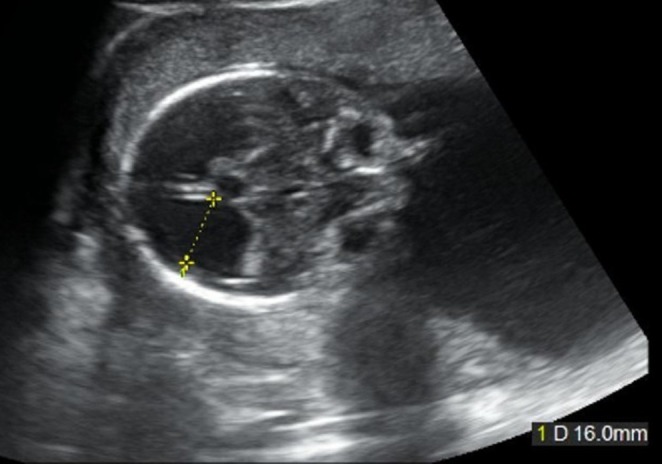 FIGURE 1
FIGURE 1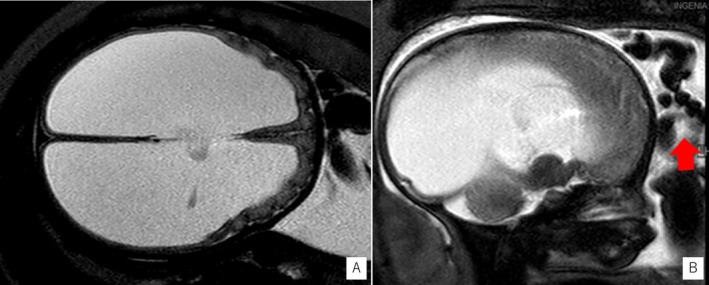 FIGURE 2
FIGURE 2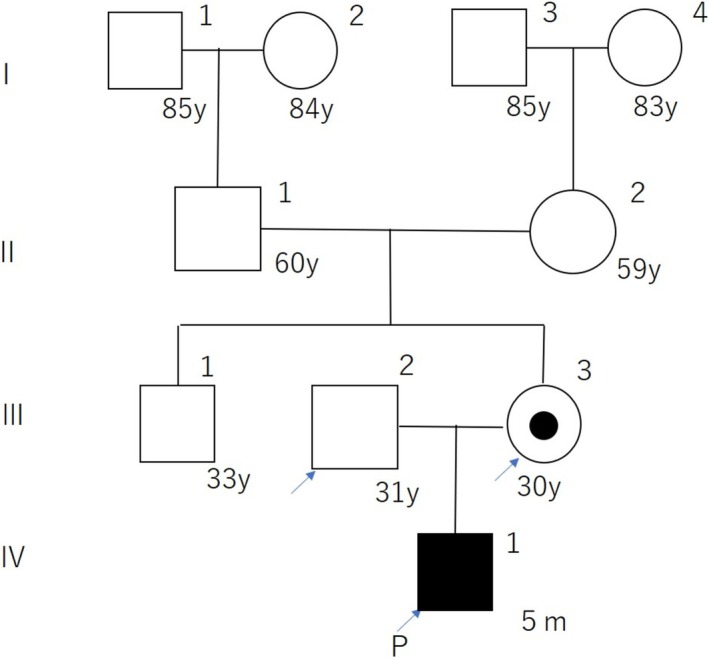 FIGURE 3
FIGURE 3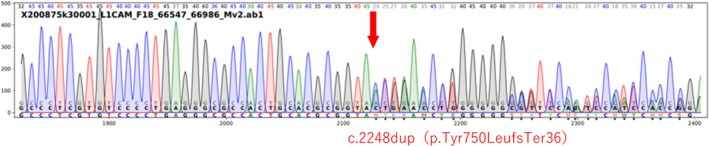 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFetal and Pediatric Neurological Disorders · Prenatal Screening and Diagnostics · RNA regulation and disease
Case History/Examination
1
A 29‐year‐old Japanese woman, Gravida 1 Para 0, conceived with ovulation induction. Her medical and family history were unremarkable. Routine ultrasound at 20 weeks' gestation revealed enlargement of the fetal lateral ventricles (posterior horn 16 mm) (Figures 1). Follow‐up imaging showed progressive ventriculomegaly and cortical thinning, suggesting fetal hydrocephalus.
Ultrasonography at 20 weeks of gestation revealed an enlargement of the posterior horn of the lateral ventricle to 16 mm.
MRI at 34 weeks gestation confirmed enlargement of the lateral and third ventricles, with suspected aqueductal stenosis (Figures 2A). An adducted left thumb was also observed (Figures 2B). The fetus was male. Given these findings and clinical suspicion of XLH, prenatal genetic testing was offered but declined.
Fetal MRI images at 34 weeks of gestation. (A) Axial T2‐weighted image showing marked enlargement of the lateral ventricles. (B) Sagittal T2‐weighted image showing adduction and flexion of the left thumb (red arrow). T1‐weighted images were not acquired in this case.
Differential Diagnosis, Investigations and Treatment
2
Biparietal diameter was significantly enlarged (110.1 mm, +7.15 SD). A cesarean section was planned at 36 weeks 3 days due to breech presentation. A male infant was delivered with Apgar scores of 7 and 9 at 1 and 5 min, respectively. Birth weight was 3054 g (+1.94 SD), and head circumference was 44.2 cm (+9.5 SD).
He was admitted to the NICU. On day 2, elevated intracranial pressure necessitated cerebrospinal fluid reservoir placement. Hirschsprung's disease was suspected and later confirmed by surgery at 38 days. A ventriculoperitoneal shunt was placed at 48 days. After ventriculoperitoneal shunt placement, no further progression of hydrocephalus has been observed. However, the child presents with severe developmental delay and spastic paraplegia, and is currently under regular follow‐up at our hospital's pediatric department. Genetic testing showed a hemizygous c.2248dup (p.Tyr750LeufsTer36) variant in the L1CAM gene. We then conducted another genetic counseling session with the client (mother) and her husband and made a carrier diagnosis for the client. The client was found to be heterozygous for the same variant as the proband (baby) (Figures 3, 4).
Pedigree of the patient and her family. Generations are shown in Roman numerals, individuals in Arabic numerals. Solid symbols indicate individuals diagnosed with XLH. The proband is marked by an arrow and the letter P.
Sanger sequencing chromatogram of the L1CAM gene showing a duplication of a thymine at position c.2248 (c.2248dupT), resulting in a frameshift (p.Tyr750LeufsTer36). Although the base numbering is not shown in the chromatogram, the duplication was confirmed by alignment with the reference sequence (NM_000425.3), and the downstream sequence shift is consistent with a single‐base duplication.
Conclusion and Results
3
Two years later, the mother conceived naturally. Non‐invasive prenatal testing (NIPT) indicated a female fetus. Ultrasound showed no hydrocephalus. A healthy girl was born by repeat cesarean section at 38 weeks. Although carrier status was unknown, genetic counseling for future testing was planned upon her reaching adulthood.
Discussion
4
X‐linked hereditary hydrocephalus (XLH) was first reported in 1949 as a disease characterized by hydrocephalus caused by stenosis of the cerebral aqueduct, neuromotor retardation, spastic paralysis of the lower limbs, and adduction flexion of the thumb [1]. The L1CAM gene has been identified as the gene responsible for XLH. L1CAM is a neuronal cell adhesion molecule located on X chromosome q28 and has important functions in the development of the nervous system [2].
With recent improvements in the diagnostic accuracy of ultrasound, the incidence of fetal ventricular enlargement detected during antenatal screening has increased. Recent reports suggest that the incidence of fetal ventriculomegaly is around 1% and is generally defined as a diameter of 10 mm or greater in the posterior horn of the lateral ventricles, regardless of gestational age. Severe ventriculomegaly is more likely than mild ventriculomegaly to cause clinical symptoms such as neurodevelopmental delay. If ventriculomegaly is detected on fetal ultrasound, detailed intracranial assessment is required. MRI is useful for fetal intracranial assessment. MRI for detailed intracranial observation is particularly useful in cases with enlarged ventricles on ultrasound [3]. Adducted thumbs are reported to be an early sign of neurodevelopmental disorders [4]. Izumi et al. reported that adducted thumbs are present in only half of patients before 24 weeks' gestation, but they are present in most cases of XLH in the second trimester [5]. Therefore, the timing of evaluation needs to be considered. In our case, the diagnosis of adducted thumbs was made by MRI, but there are no previous reports of adducted thumbs diagnosed by MRI. A more detailed evaluation of the brain by ultrasound and MRI may provide more information.
The mode and timing of delivery should be discussed. Increased head circumference may complicate delivery, even by cesarean section, increase the risk of maternal injury, and adversely affect the child's prognosis and should be considered on a case‐by‐case basis. There is no established method or timing of delivery in cases of fetal hydrocephalus, but cesarean delivery after confirmation of lung maturity is considered appropriate [6]. Kuller JA et al. suggested that cesarean delivery of a hydrocephalic fetus with macrocephaly contributes to a better prognosis [7]. In our case, we did not perform tests to confirm lung maturity. Although the fetus was delivered prematurely at 36 weeks' gestation, it was delivered at a time when lung maturity was expected.
The molecular mechanism and structure of the L1CAM protein are well understood. It is a plasma membrane protein of 1238 amino acids, with an extracellular portion of 1101 amino acids containing 6 IgG domains and 5 fibronectin III domains. Yamasaki M et al. classified the proteins into three classes according to the nature of these variants [8]. The variant in our case is class 3, which is the most severe. Michaelis RC et al. reported that the fibronectin domain variant is more severe than the IgG domain variant [9]. The c.2248dupT variant identified in this case is a novel frameshift in the fibronectin type III‐2 domain of L1CAM, a region where multiple pathogenic variants have been reported. Given the predicted loss of function and its location, this variant is considered likely pathogenic (PVS1) [10].
This variant is located within the fibronectin III‐2 domain of L1CAM, where several pathogenic missense and frameshift variants have been previously reported, such as p.Val788Phe and p.Tyr784Cys [11, 12]. These observations support the pathogenic relevance of this domain [13, 14, 15].
The probability of a de novo mutation in an X‐linked recessive condition is typically estimated at one‐third, based on classic genetic counseling principles [16]. There were no other XLH cases in the family; the probability of a de novo mutation was estimated to be about 1/3. The probability of the client being a carrier was estimated to be about 2/3, which should be taken into account when diagnosing carriers of X‐linked diseases, as the woman will be screened to see if she is a carrier.
Regarding prenatal diagnosis, Serikawa T et al. reported that in families where the first child has XLH and the mother is known to be a carrier, the next and subsequent pregnancies should be sexed by chromosome analysis, followed by L1CAM gene analysis if the child is a boy [17]. As in this case, using NIPT to diagnose the sex of the fetus may be useful in avoiding invasive tests such as amniocentesis. Preimplantation genetic diagnosis (PGD) is limited to in vitro fertilization, but PGD can reduce the burden on the mother. We need to offer this couple options based on the latest evidence when they consider their next pregnancy.
Conclusion
5
This case highlights the importance of detailed fetal imaging in diagnosing XLH. MRI findings, particularly adducted thumbs, may raise early suspicion. Identification of novel L1CAM variants is vital for expanding our understanding of this condition. Genetic counseling and testing remain essential for informed family planning.
Author Contributions
Ryosuke Horiuchi: investigation, writing – original draft. Hiroshi Sato: conceptualization, investigation, writing – original draft. Chinami Asai: investigation, writing – original draft. Fumika Hamaguchi: investigation. Yu Takaishi: investigation. Kensuke Fujiwara: data curation, investigation. Yukari Atsumi: data curation, investigation. Yukiko Ando: data curation, investigation. Takahito Kawata: data curation, investigation. Kazuyo Kakui: supervision, writing – review and editing.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. S. Bickers and R. D. Adams , “Hereditary Stenosis of the Aqueduct of Sylvius as a Cause of Congenital Hydrocephalus,” Brain 72, no. Pt. 2 (1949): 246–262.18136715 10.1093/brain/72.2.246 · doi ↗ · pubmed ↗
- 2A. Rosenthal , M. Jouet , and S. Kenwrick , “Aberrant Splicing of Neural Cell Adhesion Molecule L 1 m RNA in a Family With X‐Linked Hydrocephalus,” Nature Genetics 2, no. 2 (1992): 107–112.1303258 10.1038/ng 1092-107 · doi ↗ · pubmed ↗
- 3D. Di Mascio , A. Khalil , G. Pilu , et al., “Role of Prenatal MRI in Fetuses With Isolated Severe Ventriculomegaly: A Multicenter Study,” European Journal of Obstetrics, Gynecology, and Reproductive Biology 267 (2021): 105–110.34773875 10.1016/j.ejogrb.2021.10.014 · doi ↗ · pubmed ↗
- 4Y. S. Ouyang , Y. X. Zhang , X. N. Wu , et al., “Adducted Thumb as an Isolated Morphologic Finding: An Early Sonographic Sign of Impaired Neurodevelopment,” Medicine (Baltimore) 97, no. 38 (2018): e 12437.30235725 10.1097/MD.0000000000012437 PMC 6160029 · doi ↗ · pubmed ↗
- 5R. Izumi , H. Takahashi , Y. Kanemura , et al., “Adducted Thumb May Not Be Mandatory for Prenatal Diagnosis of X‐Linked Hydrocephalus in Early Second Trimester,” Taiwanese Journal of Obstetrics & Gynecology 61, no. 2 (2022): 353–355.35361400 10.1016/j.tjog.2022.02.027 · doi ↗ · pubmed ↗
- 6Fetology , “Chapter 16: Hydrocephalus,” in (Mc Graw‐Hill), 134–141.
- 7J. A. Kuller , V. L. Katz , S. R. Wells , L. N. Wright , and M. J. Mc Mahon , “Cesarean Delivery for Fetal Malformations,” Obstetrical & Gynecological Survey 51, no. 6 (1996): 371–375.8771576 10.1097/00006254-199606000-00022 · doi ↗ · pubmed ↗
- 8M. Yamasaki , P. Thompson , and V. Lemmon , “CRASH Syndrome: Mutations in L 1CAM Correlate With Severity of the Disease,” Neuropediatrics 28, no. 3 (1997): 175–178.9266556 10.1055/s-2007-973696 PMC 1563987 · doi ↗ · pubmed ↗