Therapeutic Effects of Electroencephalogram-Based Bioelectric Stimulation on Cognitive–Behavioural Outcomes in Children With Dual Diagnosis of Autism Spectrum Disorder and Intellectual Disability
Jiufang He, Yiping Shi, Xike Wang

TL;DR
This study shows that adding EEG-based bioelectric stimulation to standard therapies improves cognitive and behavioral outcomes in children with autism and intellectual disability.
Contribution
The novel contribution is demonstrating the added therapeutic benefits of EEG-based bioelectric stimulation in children with dual diagnosis of ASD and ID.
Findings
Children receiving EBBS had significantly lower CARS scores and improved MoCA scores compared to conventional therapy.
EBBS led to increased serum levels of 25(OH)D, folic acid, and BDNF, and better developmental outcomes in fine motor, language, and social skills.
Quality of life indicators were significantly better in the EBBS group compared to conventional treatment.
Abstract
This investigation evaluates the interventional effects of electroencephalogram-based bioelectric stimulation (EBBS) on intellectual development and behavioural symptoms in children with autism spectrum disorder (ASD) and comorbid intellectual disability (ID). By utilising a retrospective cohort design, the research team analysed 310 clinically diagnosed cases of ASD and ID that were stratified into two intervention groups: a conventional group (n = 163) receiving conventional interventions (behavioural applied behaviour analysis (ABA) therapy and structured instruction) and an observation group (n = 147) receiving the same behavioural interventions combined with EBBS. Before and following the treatment, the childhood autism rating scale (CARS), Montreal cognitive assessment (MoCA), developmental age and developmental quotient (DQ) and infants–junior middle school students' social-life…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
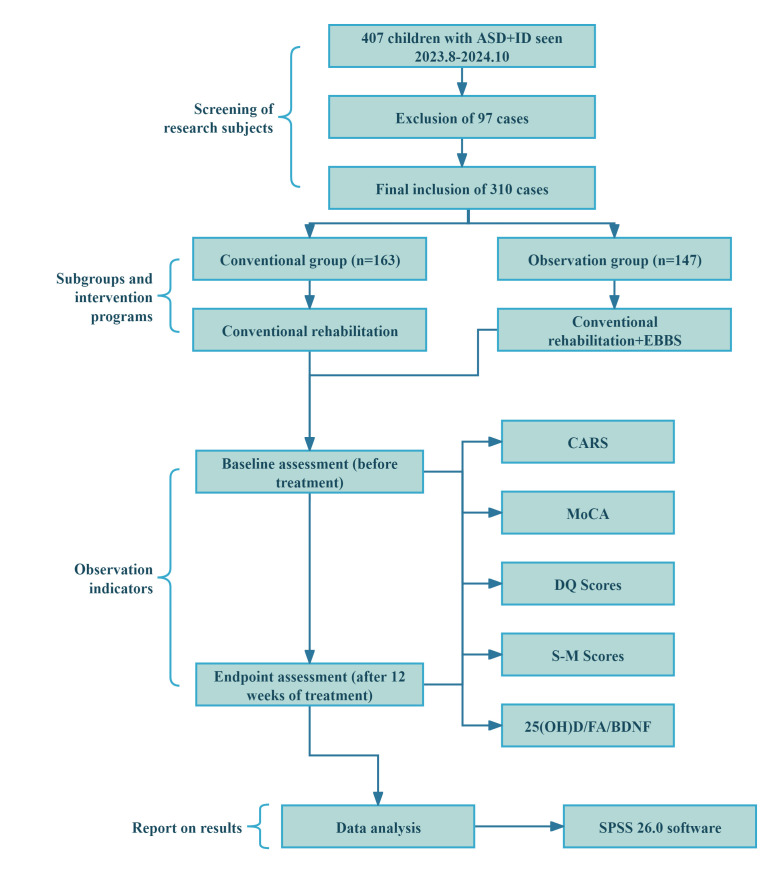 Fig. 1
Fig. 1| Conventional group (n = 163) | Observation group (n = 147) | Statistical |
| ||
| Age | 4.25 | 4.35 | t = 1.097 | 0.273 | |
| Boys | 94 (57.67) | 76 (51.70) | 0.292 | ||
| Girls | 69 (42.33) | 71 (48.30) | |||
| Duration of ASD (months) | 21.90 | 22.39 | t = 0.812 | 0.418 | |
| Family history of ASD | 0.494 | ||||
| Yes | 16 (9.82) | 18 (12.24) | |||
| No | 147 (90.18) | 129 (87.76) | |||
| Only child family | 0.303 | ||||
| Yes | 152 (93.25) | 141 (95.92) | |||
| No | 11 (6.75) | 6 (4.08) | |||
| Degree of ASD | U = 3.000 | 0.700 | |||
| Mild | 24 (14.72) | 18 (12.24) | |||
| Moderate | 94 (57.67) | 93 (63.27) | |||
| Severe | 45 (27.61) | 36 (24.49) | |||
| Conventional group (n = 163) | Observation group (n = 147) | t |
| BH Threshold ( | ||||
| CARS | Baseline | 37.94 | 38.75 | 1.074 | 0.284 | - | - | - |
| After treatment | 31.61 | 28.95 | 4.651 | 11 | 0.034 | 0.001 | ||
| t | 32.973 | 13.621 | ||||||
|
|
| Conventional group (n = 163) | Observation group (n = 147) | t |
| BH Threshold ( | ||||
| 25(OH)D (ng/mL) | Baseline | 24.68 | 24.38 | 0.595 | 0.553 | - | - | - |
| After treatment | 28.51 | 31.37 | 4.664 | 4 | 0.013 | 0.001 | ||
| t | 7.699 | 11.251 | ||||||
|
| ||||||||
| FA (ng/mL) | Baseline | 15.39 | 15.57 | 0.428 | 0.669 | - | - | - |
| After treatment | 20.66 | 22.85 | 4.674 | 3 | 0.009 | 0.001 | ||
| t | 12.731 | 14.968 | ||||||
|
| ||||||||
| BDNF (ng/mL) | Baseline | 5.24 | 5.13 | 0.834 | 0.405 | - | - | - |
| After treatment | 6.41 | 7.20 | 4.458 | 2 | 0.006 | 0.001 | ||
| t | 7.987 | 12.313 | ||||||
|
|
| Conventional group (n = 163) | Observation group (n = 147) | t |
| BH Threshold ( | ||||
| MoCA | Baseline | 16.99 | 17.22 | 0.578 | 0.563 | - | - | - |
| After treatment | 23.32 | 24.76 | 3.039 | 0.003 | 13 | 0.041 | 0.003 | |
| t | 14.243 | 16.973 | ||||||
|
|
| Conventional group (n = 163) | Observation group (n = 147) | t |
| BH Threshold ( | ||||
| Gross motor | Baseline | 64.76 | 64.15 | 0.536 | 0.592 | - | - | - |
| After treatment | 66.19 | 78.00 | 11.443 | 1 | 0.003 | 0.001 | ||
| t | 1.283 | 13.241 | ||||||
|
| 0.200 | |||||||
| Fine motor | Baseline | 51.07 | 52.42 | 1.646 | 0.101 | - | - | - |
| After treatment | 62.18 | 65.20 | 2.980 | 0.003 | 14 | 0.044 | 0.003 | |
| t | 12.631 | 13.281 | ||||||
|
| ||||||||
| Language | Baseline | 41.98 | 41.29 | 0.685 | 0.494 | - | - | - |
| After treatment | 51.50 | 54.34 | 3.119 | 0.002 | 12 | 0.038 | 0.003 | |
| t | 10.174 | 13.274 | ||||||
|
| ||||||||
| Adaptive behaviour | Baseline | 49.79 | 49.35 | 0.482 | 0.631 | - | - | - |
| After treatment | 49.81 | 53.50 | 4.053 | 5 | 0.016 | 0.001 | ||
| t | 0.020 | 4.678 | ||||||
|
| 0.984 | |||||||
| Social skills | Baseline | 48.66 | 49.36 | 0.695 | 0.487 | - | - | - |
| After treatment | 49.99 | 52.72 | 3.045 | 0.003 | 15 | 0.047 | 0.003 | |
| t | 1.294 | 3.955 | ||||||
|
| 0.200 |
| Conventional group (n = 163) | Observation group (n = 147) | t |
| BH Threshold ( | ||||
| Selrhelp | Baseline | 6.71 | 6.14 | 1.736 | 0.084 | - | - | - |
| After treatment | 6.96 | 7.52 | 2.639 | 0.009 | 16 | 0.050 | 0.009 | |
| t | 0.876 | 5.552 | ||||||
|
| 0.382 | |||||||
| Locomorion | Baseline | 3.58 | 3.63 | 0.294 | 0.769 | - | - | - |
| After treatment | 4.12 | 4.92 | 5.995 | 6 | 0.019 | 0.001 | ||
| t | 4.105 | 8.559 | ||||||
|
| ||||||||
| Occupation | Baseline | 3.93 | 4.01 | 0.333 | 0.739 | - | - | - |
| After treatment | 4.06 | 4.98 | 8.123 | 7 | 0.022 | 0.001 | ||
| t | 1.361 | 6.931 | ||||||
|
| 0.175 | |||||||
| Communication | Baseline | 3.66 | 3.64 | 0.106 | 0.916 | - | - | - |
| After treatment | 3.67 | 4.22 | 3.445 | 8 | 0.025 | 0.001 | ||
| t | 0.079 | 3.495 | ||||||
|
| 0.937 | |||||||
| Socialization | Baseline | 3.46 | 3.45 | 0.071 | 0.944 | - | - | - |
| After treatment | 4.53 | 5.16 | 4.215 | 9 | 0.028 | 0.001 | ||
| t | 7.221 | 10.734 | ||||||
|
| ||||||||
| Self-direction | Baseline | 1.63 | 1.73 | 1.733 | 0.084 | - | - | - |
| After treatment | 2.17 | 2.67 | 6.556 | 10 | 0.031 | 0.001 | ||
| t | 7.775 | 7.775 | ||||||
|
|
- —Natural Science Foundation of China - Regional Science Foundation Project
- —Guizhou Province Science and Technology Plan Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutism Spectrum Disorder Research · Attention Deficit Hyperactivity Disorder · EEG and Brain-Computer Interfaces
Introduction
The global prevalence of autism spectrum disorder (ASD), a complex neurodevelopmental condition marked by social communication impairments, repetitive and stereotypical behaviours and restricted interests, has witnessed a dramatic surge in recent decades. The World Health Organization’s statistics reveal an alarming trend, with a staggering 1 in 54 children globally receiving an ASD diagnosis [1]. The frequent co-occurrence of intellectual disability (ID) is of particular clinical significance, with research suggesting that approximately 30%–50% of individuals with ASD demonstrate comorbid cognitive impairments [2]. This dual diagnosis presents a challenging clinical profile, characterised by profound cognitive impairments, remarkably adaptive functioning deficits and severe learning difficulties, resulting in substantial caregiver burden and socioeconomic effect [3]. Epidemiological studies in China reveal an ASD prevalence of approximately 1%, with ID co-occurring in over 40% of cases. The disorder exhibits a significant male predominance [4]. Although behavioural interventions, rehabilitation training and pharmacological treatments can provide partial symptomatic relief for core ASD features in some ASD cases, their efficacy in enhancing cognitive development among children with comorbid ASD–ID remains suboptimal. This situation underscores the critical need for developing innovative therapeutic strategies to overcome existing treatment limitations [5].
Electroencephalogram (EEG)-based bioelectric stimulation (EBBS) has emerged as a promising non-invasive neuromodulation approach for neurodevelopmental disorders [6]. Through the analysis of individual EEG rhythmic patterns and delivery of biologically inspired electrical signals to targeted brain regions, EBBS can normalise aberrant neural oscillations while enhancing synaptic plasticity and neural circuit reorganisation [7]. Growing evidence suggests EBBS’s therapeutic potential in enhancing attention, executive capabilities and memory across various conditions, from cognitive rehabilitation in post-stroke patients to children with attention deficit hyperactivity disorder and learning difficulties [8, 9]. Nevertheless, its application in ASD–ID therapy remains a largely uncharted territory. A critical gap exists in current ASD research: investigations predominantly emphasise social behaviour modification while largely neglecting dual-dimensional interventions targeting cognitive development and behavioural manifestations [10]. Furthermore, the long-term therapeutic effects of EBBS remain fundamental questions that need to be addressed.
This research concentrates on the impact of EBBS on intellectual growth and behavioural manifestations in children with ASD–ID comorbidity. The imperative nature of this study can be attributed to three key factors. Firstly, the ASD-ID comorbidity presents unique clinical challenges and cognitive and behavioural issues that conventional therapies often fail to address effectively [11]. Secondly, EBBS, through its targeted regulation of abnormal EEG activities, might open a novel avenue of ‘neural remodelling’ for neurodevelopmental disorders [12]. Thirdly, the current literature suffers from methodological limitations, with most studies employing unidimensional outcome measures rather than integrating cognitive metrics [e.g., standardised intelligence quotient (IQ) measures], behavioural assessments (e.g., stereotypic behaviours and emotional dysregulation) and neurophysiological biomarkers [13]. To address these limitations, our study aims to offer evidence-based support for refining the comprehensive intervention strategies for ASD–ID comorbidity, thereby filling a significant void in this research area.
Materials and Methods
Study Design
By employing a retrospective approach, this study initially identified 407 paediatric patients diagnosed with ASD–ID who received treatment at our hospital from August 2023 to October 2024. Power analysis performed using G*Power software 3.1 (University of Düsseldorf, Düsseldorf, North Rhine-Westphalia, Germany) (two-tailed test, effect size = 0.3, = 0.05 and power = 0.95) determined a minimum required sample size of 134 participants. Following the rigorous application of inclusion and exclusion criteria, the final cohort comprised 310 subjects, stratified into two treatment groups: 163 children assigned to conventional therapy (conventional group) and 147 receiving EBBS (observation group). The conventional group received 12 weeks of applied behaviour analysis (ABA) therapy (30 minutes/session, six sessions/week) and structured teaching (30 minutes/session, six sessions/week) with no additional interventions. In addition to the same ABA therapy and structured teaching, the observation group underwent EBBS sessions (20 minutes/day, 5 days/week) using the HB520D system. The main process of this study is shown in Fig. 1. The study protocol received ethical approval from Guizhou Provincial People’s Hospital (Approval Number: 2021-57)’s ethics committee, and all the participants’ legal guardians provided documented informed consent prior to enrolment.
Flow chart of this study. Note: EBBS, Electroencephalogram-based bioelectric stimulation; ASD, Autism Spectrum Disorder; CARS, Childhood Autism Rating Scale; 25(OH)D, 25-Hydroxyvitamin D; FA, Folic Acid; BDNF, Brain-Derived Neurotrophic Factor; MoCA, Montreal Cognitive Assessment; DQ, Developmental Quotient; S–M, Infants–Junior Middle School Students’ Social–Life Abilities Scale.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) confirmed diagnosis of ASD; (2) concurrent ID as defined in the Diagnostic and Statistical Manual of Mental Disorders [14] and categorised as mild [requiring minimal support (e.g., social communication difficulties with limited impact on daily functioning)], moderate [requiring substantial support (e.g., marked deficits in verbal/nonverbal communication)] and severe [requiring very substantial support (e.g., extreme communication deficits and repetitive behaviours)]; (3) completion of at least 3 months of consistent treatment in our hospital; (4) age 12 years; and (5) availability of complete medical records.
The exclusion criteria were as follows: (1) behavioural presentations not attributable to a primary ASD diagnosis; (2) significant comorbid medical conditions including acute infections, cardiopulmonary dysfunction or severe organ system pathologies; (3) comorbid conditions that could interfere with the treatment of the primary diagnosis; (4) presence of implanted electronic medical devices (e.g., pacemakers); and (5) current or historical diagnosis of seizure disorders.
Therapeutic Interventions
Conventional rehabilitation protocol: (1) ABA therapy: This evidence-based intervention employs behavioural shaping principles with positive reinforcement to enhance various developmental skills. The structured protocol involves four key phases: therapist instruction delivery, child response elicitation, therapist feedback provision and inter-trial interval. In practice, the therapist designs suitable functional games tailored to the child’s developmental functions and interacts with the child. During this interactive process, the therapist provides prompts or assistance to guide the child in performing correct behaviours. As the training progresses, the amount of assistance is gradually decreased until the child can independently execute the correct actions without any external help. A short interlude is scheduled between the training of every two decomposed actions. This treatment was administered six times per week, with each session lasting 30 minutes. (2) Structured teaching: This method focuses on targeted training to address deficits in language, communication, sensory perception and behavioural issues. By using clear and easily understandable visual cues, the therapist tailors the training content and requirements to the child’s abilities and elaborates them to the child in detail. The training scope covers a wide range of aspects, including fine motor skills, gross motor imitation, cognitive abilities, perception skills, language comprehension and expression, hand–eye coordination, social interaction, daily living activities and emotional regulation. The training environment is specially arranged, emphasising structured scheduling and visual prompts. Various methods such as verbal cues, written instructions, labels, body gestures and icons are employed to enhance the child’s understanding and mastery of the training content. This protocol was delivered in 30-minute sessions, six times weekly throughout the 12-week intervention period.
EBBS protocol: The therapeutic regimen incorporates the HB520D EEG biofeedback
system as an adjunct to conventional rehabilitation. Following device
initialisation, the main electrode output line is connected to crescent-shaped
electrodes. The bilateral postauricular mastoid processes are cleansed with
sterile saline and allowed to air-dry before electrode placement. The HB520D
system delivers (Haobro, Suzhou, Jiangsu, China) transcranial alternating current
stimulation at a frequency of 10 Hz (alpha band), with a biphasic square waveform
(pulse width: 200 ms; inter-pulse interval: 50 ms). Current intensity is
individualised, starting at 0.5 mA (35% device output) and titrated weekly by
0.1–0.2 mA based on real-time EEG feedback. Electrodes (Ag/AgCl, 5 cm^2^) are
placed bilaterally over the mastoid processes (Cb1/Cb2 according to the 10–20
EEG system). Alpha Power Quantification: Spectral analysis was performed using
fast Fourier transformation (FFT) to compute absolute alpha power
(812 Hz) in the occipital regions. Real-time feedback was
visualized via a dynamic spectrogram displaying alpha amplitude modulation.
Target Achievement Criteria: Stimulation intensity (0.51.5 mA)
was adjusted weekly based on the following thresholds: Baseline Phase: Achieve
70% alpha power enhancement in occipital regions compared to
pre-intervention baseline for 5 consecutive minutes. Titration Phase: Increment
current by 0.1~0.2 mA if alpha power remained below 85% of
target; maintain or reduce intensity if 90% target was sustained. The
EBBS protocol comprised daily 20-minute sessions, administered 5 days per week
over a 12-week intervention period.
Baseline Data Collection
Demographic and clinical characteristics including age, gender and disease duration were systematically recorded for all the participants.
Detection of Cytokines
Serum biomarkers including 25-hydroxyvitamin D [25(OH)D], folic acid (FA) and brain-derived neurotrophic factor (BDNF) were measured at baseline and post intervention (within 24 hours after the final EBBS session). Blood samples were analysed using ELISA kits (manufacturer: BioVision Inc., Beijing, China) and processed on a BioTek Synergy H1 microplate reader (absorbance: 450 nm) following the manufacturer protocols. The intra- and inter-assay coefficients of variation were 8% and 12%, respectively.
Scale Assessments
All the scales were administered at two time points: baseline (pre-intervention) and immediately post intervention (12 weeks). Assessments were conducted by trained clinicians blinded to group allocation.
(1) The Childhood autism rating scale (CARS) [15] assesses autism severity across 15 behavioural domains (e.g., social interaction and communication). It comprises 15 items scored on a 4-point Likert scale (1 = ‘normal for age’ to 4 = ‘severely abnormal’). The total score ranges from 15 to 60. Scores 29 indicate non-autistic, 30–36.5 indicate mild-to-moderate autism and 37 indicate severe autism. The Chinese version demonstrates Cronbach’s = 0.92, test–retest reliability (ICC = 0.89) and convergent validity with ADOS-2 (r = 0.75) [16].
(2) The Montreal cognitive assessment (MoCA) [17] evaluates global cognitive function (attention, memory, language and visuospatial abilities). It comprises 30 items across seven domains. The total score ranges from 0 to 30. Scores 26 indicate normal cognition, and 26 suggest cognitive impairment. The Chinese version shows Cronbach’s = 0.85, inter–rater reliability ( = 0.82) and discriminant validity between ASD-ID and typical development (AUC = 0.91) [18].
(3) The developmental age is used to quantify developmental progress relative to chronological age and was calculated in this study using the Chinese psycho-educational profile. It evaluates five functional domains: gross motor, fine motor, language, adaptive behaviour and social skills. Each subdimension contains three items, each scored on a 0–2 scale, and the total score is converted to age-equivalent values. Linear interpolation can be performed if the total score spans two age stages (for example, the cognitive dimension score corresponds to 18–24 months and is calculated according to the actual score proportion). In terms of internal consistency, its Cronbach’s = 0.89. Regarding convergent validity, it correlates with Bayley scales (r = 0.78) [19]. The developmental quotient (DQ) was calculated as [20] developmental age / chronological age 100.
(4) The infants–junior middle school students’ social–life abilities scale (S–M) [21] examines six competency areas: selrhelp, locomorion, occupation, communication, socialization and self-direction. Result assessment: 5 is classified as extremely severe. A score of 6 is considered severe. 7 points moderate; 8 points is mild. 9 points is the edge. A score of 10 or above is normal. In terms of internal consistency, its Cronbach’s = 0.88 (Chinese version). Regarding convergent validity, it is strongly correlated with the Vineland adaptive behaviour scale (r = 0.79) [22].
Statistical Analysis
Statistical analysis was conducted using SPSS 26.0 software (IBM, Armonk, NY, USA). Categorical variables were compared using the chi-square test. For ordinal variables (e.g., ASD severity), non-parametric tests were performed (Mann–Whitney U test for two-group comparisons). Continuous variables first underwent normality assessment using the Shapiro–Wilk test to determine if the data conform to a normal distribution. Normally distributed data were analysed using independent samples t-tests and paired t-tests. Statistical significance was evaluated using the Benjamini-Hochberg (BH) procedure to control the false discovery rate (FDR) due to multiple comparisons. Significance was determined as follows: reject H0 if p(𝑘) threshold_k_. Adjusted p-values (q-values) were computed as q_(𝑘)_ = min [*p_(𝑘)_ *N/k,1]. All 16 tests remained significant after BH correction (q 0.05). Adjusted p-values were reported for all outcomes, with the significance threshold set at *p * 0.05.
Results
Comparison of Clinical Characteristics
The baseline characteristics (age, disease duration and gender) showed no statistically significant differences between the two groups (*p * 0.05). Not only that, there were no differences in the course of ASD, family medical history, and severity between the two groups (*p * 0.05), confirming their comparability (Table 1).
Comparison of ASD Improvement
No differences in baseline CARS score were observed between the two groups (*p * 0.05). Both groups showed decreased CARS scores after intervention (*p * 0.05). Compared with the conventional group, the observation group demonstrated significantly lower CARS scores after treatment (*p * 0.05).
Comparison of Serum Cytokine Levels
Baseline cytokine concentrations showed no intergroup differences for any measured biomarkers (*p * 0.05). Post treatment, both groups exhibited significant elevation in 25(OH)D, FA and BDNF levels (*p * 0.05). Particularly, the observation group showed significantly greater increases than the conventional group (*p * 0.05).
Comparison of Cognitive Function
Cognitive assessment demonstrated equivalent baseline performance on MoCA measures (*p * 0.05). Following intervention, both groups showed cognitive enhancement (as evidenced by their increased MoCA scores). However, the observation group demonstrated significantly greater improvements than the conventional group (*p * 0.05).
Comparison of Developmental Age and DQ
Baseline DQ scores were similar between the groups (*p * 0.05). Post treatment, the conventional group showed no significant changes in gross motor, adaptive behaviour or social skills (*p * 0.05) but demonstrated improvement in fine motor and language domains (*p * 0.05). The observation group exhibited significant improvement in all domains (gross motor, fine motor, language, adaptive behaviour and social skills), with scores significantly higher than those of the conventional group (*p * 0.05).
Comparison of Daily Living Skills
According to the S–M scale results, the conventional group showed improved scores in locomorion, socialization and self-direction (*p * 0.05) but no significant changes in selrhelp, occupation or communication (*p * 0.05). By contrast, the observation group demonstrated significant improvement in all S–M domains, with scores significantly higher than those of the conventional group (*p * 0.05).
Adjustment of Results
Using the Benjamini-Hochberg procedure, all 16 post-hoc tests retained statistical significance after adjusting for multiple comparisons (adjusted q-values 0.05; see Tables 2,3,4,5,6 for detailed results).
Discussion
Different from conventional therapies that primarily target behavioural modification through external reinforcement [23], EBBS directly modulates neural activity via bioelectric stimulation [24]. This dual-action mechanism—normalising aberrant EEG oscillations while enhancing synaptic plasticity—enables simultaneous improvements in cognitive function (e.g., MoCA scores) and behavioural symptoms (e.g., CARS reduction). Such multidimensional efficacy is critical for ASD–ID comorbidity, where ID-related cognitive impairments often hinder responsiveness to behavioural training alone.
Comparative analysis of ASD symptom improvement revealed superior outcomes in the observation group, as evidenced by their significantly lower CARS scores compared with those of the controls. Current clinical research has confirmed that conventional comprehensive rehabilitation therapy works by guiding children with ASD to participate in various activities, thereby training and enhancing their neuronal responsiveness. As a core component of this approach, ABA specifically aims to modify abnormal behaviours in ASD while promoting the development of multiple competencies. Meanwhile, structured teaching capitalises on visual learning strengths to enhance environmental perception and task execution while reducing anxiety and stress when confronted with unfamiliar situations [25]. Nevertheless, for children with ASD–ID comorbidity, the cognitive and developmental limitations characteristic of ID markedly impair their learning capacity and training responsiveness, resulting in their suboptimal responses to conventional rehabilitation strategies [26].
In this study, the superior ASD improvement observed in the observation group may be mechanistically explained by several factors: (1) EBBS operates through the cerebellum–thalamus–cerebral cortex neural network, with direct projections to the cerebellar fastigial nucleus via cortical pathways. This dual mechanism of cortical excitation coupled with neurodevelopmental stimulation significantly contributes to cerebral functional enhancement [27]. The significantly elevated post-treatment levels of 25(OH)D [28] and FA [29] in the observation group relative to those of the controls can also confirm our view. The observed elevation in 25(OH)D and FA may reflect the secondary effects of EBBS. Enhanced neural activity and cerebral perfusion can improve nutrient absorption or metabolic regulation. Alternatively, behavioural improvements (e.g., reduced food selectivity) might indirectly increase dietary intake of vitamin D and folate. However, the direct causal links require further investigation. (2) Axonal shortening, degeneration and transport impairment are characteristic neuropathological features in ID [30]. Experimental evidence from Athavale et al. [31] animal studies indicates that EBBS exhibits potent axonal regeneration-inducing properties that facilitate synaptic remodelling. Such effects benefit the recovery of cognitive learning and memory processes. The significant post-treatment elevation of BDNF levels in the observation group provides further confirmation, as BDNF is known to mediate neuronal regeneration, differentiation and developmental processes and play a vital role in the repair, injury and development of the nervous system [32]. These findings are corroborated by Villalobos J et al.’s [33] demonstration of EBBS-mediated neurological improvement in diabetic rat models, showing remarkable consistency with our clinical observations. (3) EBBS employs advanced digital frequency synthesis technology to transform specific pulse sequences and bioelectrical signals into EEG-simulated bio-currents. These precisely modulated currents are then delivered through bilateral mastoid (postauricular) electrodes to target the cerebellar fastigial nucleus region. Leveraging the principles of fastigial nucleus electrical stimulation, this innovative approach induces beneficial neuroplastic changes, including brain tissue reorganisation and enhanced cerebral blood perfusion [34]. Our study results provide compelling evidence for EBBS’s cognitive-enhancing effects, with the observation group demonstrating significantly superior post-treatment MoCA scores compared with the control participants.
Longitudinal assessment revealed pronounced improvements in developmental age and DQ among the EBBS-treated subjects. As a standardised metric for evaluating intellectual functioning in children with intellectual disabilities, developmental age and DQ calculation involves the ratio of mental age to chronological age. During the treatment course, the developmental age and DQ can register a positive elevation only when the increment in mental age surpasses that of the chronological age [35]. The observed increase in developmental age and DQ indicates that the mental age progression in the observation group outpaced normal chronological aging during the treatment period, representing meaningful cognitive gains. The treatment response rate in this study directly reflects the intervention efficacy within the group, corroborating the effectiveness of the EBBS protocol. These findings align with those reported by Wang C et al. [36], who investigated the application of EBBS in treating refractory hypertension. Quality of life assessments using the S–M scale further corroborated these positive outcomes, with the observation group showing greater improvements in daily functioning and overall quality of life compared with the controls. An interesting methodological observation revealed apparent discrepancies between fine motor skill assessments (developmental age and DQ) and functional ability measures (S–M scale). This discordance reflects fundamental differences in the assessment’s focus rather than contradictory results—the developmental age and DQ demands highly precise fine-finger movements from children, whereas the S–M scale places emphasis on the functional operations and capabilities accomplished by children using both hands. Nevertheless, the research group acknowledge the possibility of random variation influencing these outcomes, necessitating further investigation through large-scale studies.
For ASD–ID intervention, EBBS should be integrated as an adjunct to multidisciplinary frameworks. For instance, combining EBBS with ABA therapy could synergise neuromodulation (targeting cognitive deficits) and behavioural shaping (addressing social communication). Future protocols might sequence EBBS sessions before structured teaching to prime neural responsiveness. Additionally, serum biomarker (e.g., BDNF) monitoring could personalise stimulation parameters, ensuring optimal synergy with pharmacological or occupational therapies. Such integration requires collaborative efforts among neurologists, psychologists and rehabilitation specialists to tailor multimodal interventions.
As a retrospective study, this research lacks a sham stimulation control group. Although the observation group showed significant improvements compared with the control group, the placebo effect cannot be entirely ruled out. Future randomised controlled trials should incorporate blinded sham-controlled designs to isolate the specific effects of EBBS. Additionally, the absence of supporting in vitro studies prevents us from drawing definitive conclusions about EBBS’s precise biological mechanisms, representing an important area for subsequent investigation.
Conclusion
This study provides substantive evidence that EBBS intervention significantly improves cognitive function, behavioural symptoms and adaptive living skills among children with comorbid ASD–ID. The parallel elevations observed in serum 25(OH)D, FA and BDNF levels suggest that EBBS’s therapeutic effects may be mediated through the dual mechanisms of neural circuit remodelling and metabolic pathway modulation.
Availability of Data and Materials
The data used and/or analyzed during the current study are available from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hirota T King BH Autism Spectrum Disorder: A Review JAMA 202332915716810.1001/jama.2022.2366136625807 · doi ↗ · pubmed ↗
- 2Maguire E Mulryan N Sheerin F Mc Callion P Mc Carron M Autism spectrum disorder in older adults with intellectual disability: a scoping review Irish Journal of Psychological Medicine 20223928730010.1017/ipm.2021.6534612183 · doi ↗ · pubmed ↗
- 3Stefanski A Calle-López Y Leu C Pérez-Palma E Pestana-Knight E Lal D Clinical sequencing yield in epilepsy, autism spectrum disorder, and intellectual disability: A systematic review and meta-analysis Epilepsia 20216214315110.1111/epi.1675533200402 PMC 7839709 · doi ↗ · pubmed ↗
- 4Xie S Karlsson H Dalman C Widman L Rai D Gardner RM et al The Familial Risk of Autism Spectrum Disorder with and without Intellectual Disability Autism Research: Official Journal of the International Society for Autism Research 2020132242225010.1002/aur.241733103358 PMC 7821228 · doi ↗ · pubmed ↗
- 5Marrus N Koth KA Hellings JA Mc Donald R Gwynette MF Muhle R et al Psychiatry training in autism spectrum disorder and intellectual disability: Ongoing gaps and emerging opportunities Autism: the International Journal of Research and Practice 20232767968910.1177/1362361322111219735920285 · doi ↗ · pubmed ↗
- 6Kayarian FB Jannati A Rotenberg A Santarnecchi E Targeting Gamma-Related Pathophysiology in Autism Spectrum Disorder Using Transcranial Electrical Stimulation: Opportunities and Challenges Autism Research: Official Journal of the International Society for Autism Research 2020131051107110.1002/aur.231232468731 PMC 7387209 · doi ↗ · pubmed ↗
- 7Casanova MF Shaban M Ghazal M El-Baz AS Casanova EL Sokhadze EM Ringing Decay of Gamma Oscillations and Transcranial Magnetic Stimulation Therapy in Autism Spectrum Disorder Applied Psychophysiology and Biofeedback 20214616117310.1007/s 10484-021-09509-z 33877491 · doi ↗ · pubmed ↗
- 8Schlaeppi JA Affentranger L Bervini D Z’Graggen WJ Raabe A Pollo C Electrical Stimulation for Cerebral Vasospasm After Subarachnoid Hemorrhage: A Systematic Review Neuromodulation: Journal of the International Neuromodulation Society 2022251227123910.1016/j.neurom.2022.01.02035382977 · doi ↗ · pubmed ↗