Pancreatic Schwannoma: A Rare Culprit But Accurate Diagnosis Can Avoid Resection
Shin Kato, Mariko Tsukamoto, Taichi Murai, Koji Hirata, Yuta Koike

TL;DR
A rare pancreatic tumor called schwannoma was accurately diagnosed using imaging and biopsy, avoiding unnecessary surgery.
Contribution
Demonstrates how EUS-guided biopsy and immunohistochemistry can accurately diagnose pancreatic schwannomas preoperatively.
Findings
Schwannoma was diagnosed via EUS-guided biopsy and confirmed by S-100 positivity and other marker negativity.
Conservative management was successful with no tumor growth over two years of follow-up.
Accurate diagnosis avoided unnecessary surgical resection in this case.
Abstract
Pancreatic schwannomas are extremely rare benign tumors originating from Schwann cells of peripheral nerves, often mimicking more common pancreatic tumors, such as neuroendocrine neoplasms or solid pseudopapillary neoplasms, making preoperative diagnosis challenging. We describe a 65-year-old asymptomatic man referred for evaluation of an incidental pancreatic body mass detected by ultrasound. Laboratory findings, including liver enzymes and tumor markers (CA19-9 and CEA), were normal. Contrast-enhanced CT revealed a well-defined 20 mm mass with delayed enhancement, and MRI showed low intensity on T1-weighted images, mildly high on T2, and slight diffusion restriction. Based on imaging, a pancreatic neuroendocrine neoplasm was initially suspected. Endoscopic ultrasound-guided tissue acquisition with a 22-gauge needle was performed. Histology revealed bundles of spindle-shaped cells with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1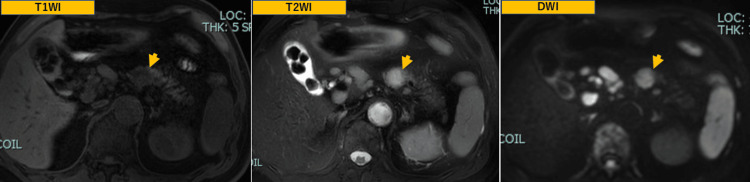 Figure 2
Figure 2 Figure 3
Figure 3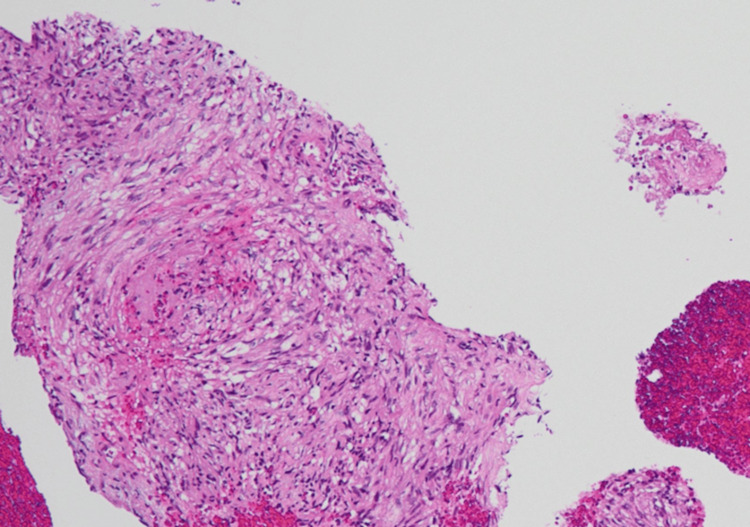 Figure 4
Figure 4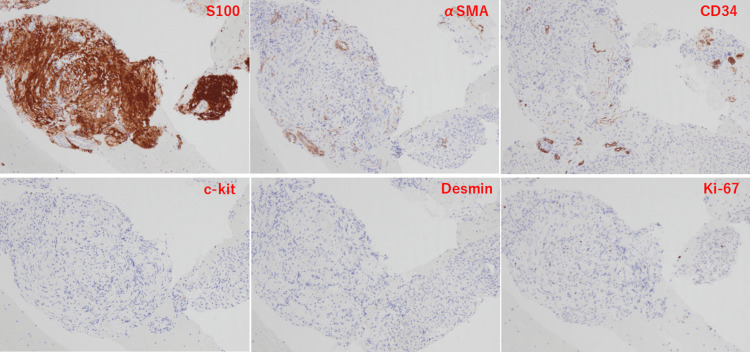 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Neuroendocrine Tumor Research Advances · Pancreatic and Hepatic Oncology Research
Introduction
Schwannomas are benign, slow-growing, encapsulated tumors derived from Schwann cells of the peripheral nerve sheaths and initially reported by Verocay in 1910 [1]. They typically arise in the head, neck, and mediastinum [2], while only 0.7% of schwannomas arise in the retroperitoneum, including the pancreas [3], with fewer than 100 cases reported in the English literature worldwide.
Radiologically, pancreatic schwannomas often present as well-defined solid or mixed solid-cystic lesions, mimicking pancreatic neuroendocrine neoplasm (PNEN), solid-pseudopapillary neoplasm (SPN), or even malignant tumors, such as adenocarcinoma or adenosquamous carcinoma [4,5]. Accurate preoperative diagnosis remains challenging but is clinically important, as most pancreatic schwannomas have a benign course and surgical resection can often be avoided.
Case presentation
A 65-year-old asymptomatic man with no significant past medical history, family history of pancreatic cancer, or habits of smoking and drinking was referred to our hospital for further evaluation of a pancreatic body mass incidentally identified on a routine health check-up ultrasound.
Laboratory tests showed no abnormalities, including liver function tests, serum amylase, lipase, and tumor markers (CA19-9 and CEA). Contrast-enhanced CT revealed a round, 20 mm, well-circumscribed mass in the pancreatic body with delayed enhancement and no involvement of the main pancreatic duct (Figure 1).
CT imagesDynamic CT showed a 20 mm round, expansile mass (arrow head) with a smooth surface in the pancreatic body, without involvement of the main pancreatic duct. The mass was mildly enhanced in the early phase and showed gradual and marked enhancement in the delayed phase.
MRI demonstrated low intensity on T1-weighted images, mildly high intensity on T2-weighted images, and slight restriction on diffusion-weighted imaging of the mass (Figure 2).
MRI imagesMRI demonstrated low intensity on T1-weighted images, mildly high intensity on T2-weighted images, and slight restriction on diffusion-weighted imaging of the mass (arrow head).
Based on imaging, the differential diagnosis included PNEN (somewhat atypical because it was not strongly hypervascular), SPN, and adenosquamous carcinoma.
For definitive diagnosis, endoscopic ultrasound-guided tissue acquisition (EUS-TA) was performed using a 22-gauge Franseen needle (SonoTip TopGain, Medico’s Hirata Inc., Osaka, Japan) (Figure 3).
EUS imageEndoscopic ultrasound (EUS) presented a low echoic, smooth surface mass on pancreatic body. EUS tissue acquisition (EUS-TA) was performed using a 22-gauge Franseen needle for two times puncture with aspiration.
Histopathological examination revealed bundles of spindle-shaped cells with mildly atypical nuclei and clear to pale eosinophilic cytoplasm (Figure 4).
Hematoxylin-eosin stainHematoxylin-eosin stain of specimen showed bundles of spindle-shaped cells with mildly atypical nuclei and clear to pale eosinophilic cytoplasm (magnification ×100).
Immunohistochemical staining showed diffuse positivity for S-100 protein and negativity for αSMA, CD34, c-Kit, Desmin, chromogranin A, and synaptophysin, consistent with schwannoma. Low expression of Ki-67 labelling index was also observed (Figure 5).
Immunohistochemical stainingImmunohistochemical staining showed diffuse positivity for S-100 protein and negativity for αSMA, CD34, c-Kit, and desmin. Low expression of Ki-67 labelling index was also observed (magnification ×100).
Given the benign nature of the pancreatic schwannoma and the absence of symptoms, the patient was managed conservatively with imaging surveillance instead of surgery. Over two years of follow-up, there was no evidence of tumor growth.
Discussion
Pancreatic schwannomas are exceedingly rare, accounting for less than 1% of all pancreatic neoplasms [6,7]. These tumors often appear as round solid lesions, sometimes with necrosis or cystic degeneration [8], and may show a range of contrast enhancement patterns on CT, from hypervascular to delayed enhancement - all of which are nonspecific. On MRI, schwannomas present as homogeneously hypointensity on T1WI and hyperintense on T2WI. However, these findings sometimes appear heterogeneously hyperintense due to the variable degeneration background of the tumor, which is non-specific, similar to other pancreatic tumors [4,5]. Current report also described that pancreatic schwannomas frequently show increased FDG uptake on PET/CT, contrary to their benign features [9]. Because of their rarity and imaging overlap, they are frequently misdiagnosed as PNEN or SPN.
EUS-TA plays a critical role in the preoperative evaluation of pancreatic schwannomas [10-13]. The presence of spindle-shaped cells and a characteristic immunohistochemical profile - strong S-100 positivity and absence of epithelial and mesenchymal markers (AE1/AE3, c-Kit, CD34, and desmin) - helps confirm the diagnosis.
Accurate preoperative diagnosis is clinically important: while PNEN and SPN are often surgically resected due to malignant potential, pancreatic schwannomas are typically benign and slow-growing and rarely undergo malignant transformation [14]. There is no established index to strongly suspect malignancy unique character to pancreatic schwannoma, and the criteria for peripheral nerve and soft tissue-derived schwannomas have been used alternatively. According to these diagnostic criteria, findings suggestive of malignancy include tumor diameter greater than 5 cm, hemorrhagic necrosis, high Ki-67 labelling index, and a tendency to invade surrounding tissues [15]. Pancreatic schwannomas without these findings have a very high probability of being benign, and imaging follow-up rather than resection could be the gold standard. Thus, unnecessary surgery and its associated risks can be avoided through correct diagnosis.
Our case underscores the importance of including schwannomas in the differential diagnosis of solid pancreatic lesions and highlights the value of EUS-guided biopsy with immunohistochemistry for precise diagnosis.
Conclusions
Pancreatic schwannomas, though rare, should be considered in the differential diagnosis of well-defined pancreatic masses. EUS-guided sampling with immunohistochemistry is essential for accurate preoperative diagnosis and may help avoid unnecessary surgical intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1[On the knowledge of "neurofibromas"]Beitr Z Path Anat Verocay J 169481910 https://cir.nii.ac.jp/crid/1571135649651787520
- 2Case report 872. "Ancient" schwannoma (degenerated neurilemoma)Skeletal Radiol Schultz E Sapan MR Mc Heffey-Atkinson B Naidich JB Arlen M 593595231994782499610.1007/BF 00223102 · doi ↗ · pubmed ↗
- 3Benign solitary schwannomas (neurilemomas)Cancer Das Gupta TK Brasfield RD Strong EW Hajdu SI 355366241969579677910.1002/1097-0142(196908)24:2<355::aid-cncr 2820240218>3.0.co;2-2 · doi ↗ · pubmed ↗
- 4Pancreatic schwannoma: literature review J Surg Educ Gupta A Subhas G Mittal VK Jacobs MJ 1681736620091971291710.1016/j.jsurg.2008.12.001 · doi ↗ · pubmed ↗
- 5Pancreatic schwannoma- CT and MRI findings: a rare case report and review of literature Ann Med Surg (Lond) Aichouni N Abbou W Nasri S 1026646820213440113610.1016/j.amsu.2021.102664 PMC 8355828 · doi ↗ · pubmed ↗
- 6Pancreatic schwannoma: an uncommon but important entity J Gastrointest Surg Almo KM Traverso LW 359363520011198597510.1016/s 1091-255x(01)80062-7 · doi ↗ · pubmed ↗
- 7Pancreatic schwannoma: a rare case and a brief literature review Int J Surg Case Rep Ercan M Aziret M Bal A 1011042220162708498410.1016/j.ijscr.2016.03.014PMC 4844663 · doi ↗ · pubmed ↗
- 8Pancreatic schwannoma with cystic degeneration: a case report and literature review Taehan Yongsang Uihakhoe Chi Park JS Min SJ Kim H Choi JA 1942008220213623744910.3348/jksr.2020.0031 PMC 9432392 · doi ↗ · pubmed ↗