Childhood Obstructive Sleep Apnea and Systemic Blood Pressure and Kidney Function: A Systematic Review and Meta-Analysis
Sara Rodriguez-Lopez, Daniel Ofosu, Christopher Gerdung, Diana Keto-Lambert, Meghan Sebastianski, Meng Lin, Maria Castro-Codesal

TL;DR
This study finds that childhood obstructive sleep apnea is linked to higher blood pressure, but treatment alone may not lower it.
Contribution
The study provides the first comprehensive meta-analysis on the relationship between childhood OSA and systemic BP outcomes.
Findings
Children with OSA had significantly higher daytime and nighttime systolic and diastolic blood pressure compared to controls.
OSA treatment (adenotonsillectomy or positive airway pressure) did not significantly reduce blood pressure in children.
There is limited research on the effects of childhood OSA on kidney function.
Abstract
Background: Obstructive sleep apnea (OSA) is a recognized risk factor for high blood pressure (BP) and chronic renal dysfunction in adults. However, it remains uncertain whether a similar association exists in children. Objectives: This study assessed the associations between childhood OSA and systemic BP and renal outcomes. Additionally, it examined the effects of OSA treatments on BP in children. Methods: A systematic literature search was conducted to identify relevant studies up to August 2024. Results: Sixty-four studies, consisting of 44 observational studies and 20 OSA interventional studies, were included. Compared with healthy control groups, children with OSA had significantly higher daytime systolic BP (3.30 mmHg; 95% CI, 2.07–4.53), daytime diastolic BP (1.27 mmHg; 95% CI, 0.69–1.84), nighttime systolic BP (4.08 mmHg; 95% CI, 2.71–5.46), nighttime diastolic BP (2.12 mmHg;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
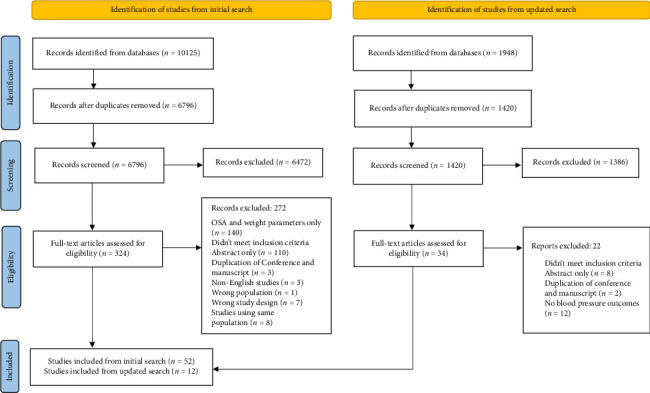 Figure 1
Figure 1 Figure 2
Figure 2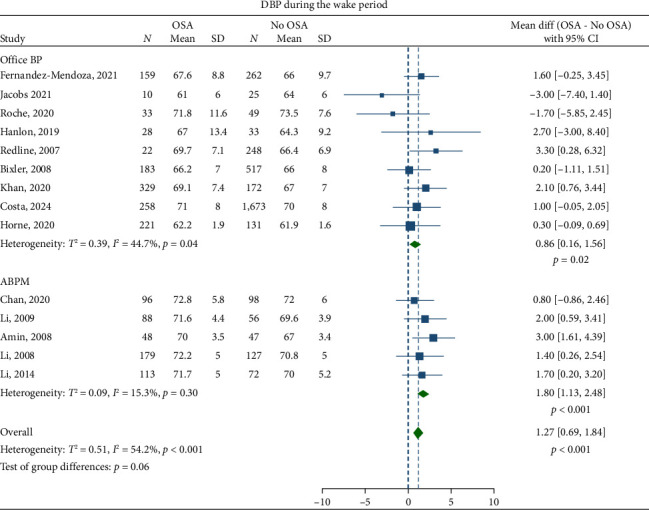 Figure 3
Figure 3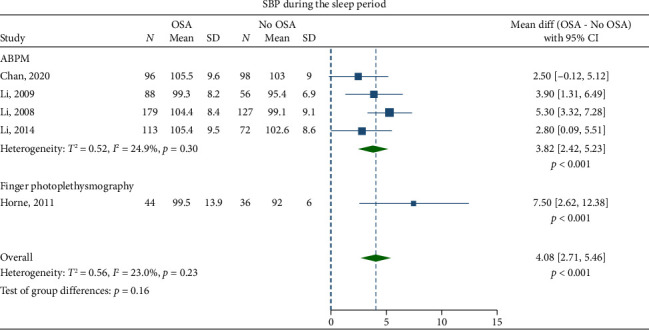 Figure 4
Figure 4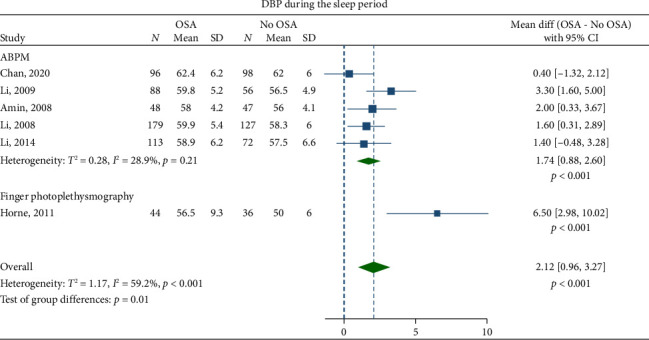 Figure 5
Figure 5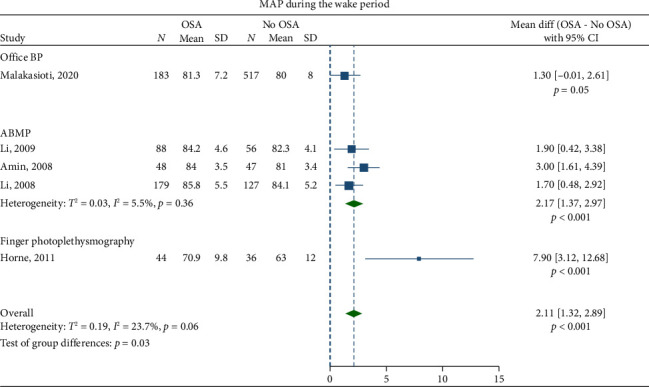 Figure 6
Figure 6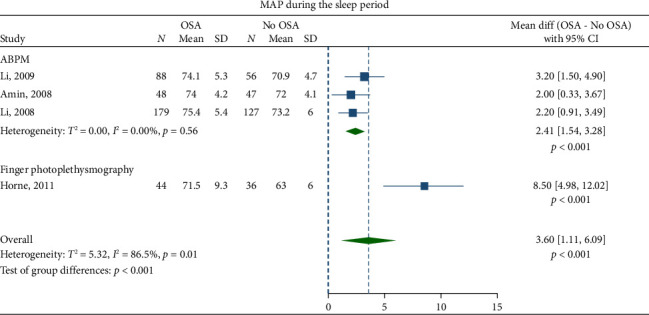 Figure 7
Figure 7- —Alberta Strategy for Patient-Oriented Research (SPOR) Support Unit
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Cardiovascular and Diving-Related Complications · Neuroscience of respiration and sleep
1. Introduction
Obstructive sleep apnea (OSA) is characterized by recurrent events of partial or complete upper airway obstruction during sleep, resulting in disruption of normal ventilation and sleep patterns [1]. It has become increasingly common in children with rates up to 5.7% in the general pediatric population [2], and up to nearly 80% in children with obesity [3–5]. In adults, OSA is a known risk factor for high blood pressure (BP) [6–9], and several evidence syntheses are available [10–12].
An increasing number of publications in children have also suggested a link between OSA and high BP [13–19], although the evidence remains conflicting. Two previous meta-analyses [20, 21] have reported conflicting results regarding the association between childhood OSA and an increased risk of adverse BP outcomes. As a result, the impact of childhood OSA on BP remains unclear. Additionally, recent studies have emerged that were not included in the earlier meta-analyses. This underscores the need to summarize the latest evidence to clarify the association between childhood OSA and systemic BP.
Adenotonsillectomy (AT) is the initial treatment for children with OSA [22]. Positive airway pressure (PAP) therapy is often used to treat residual OSA after AT or if AT is not an option. This is especially true in children with obesity [22, 23]. Recent data suggest that these treatments can effectively improve BP outcomes in children with OSA [24–29]. However, there is limited research synthesizing the effects of AT on BP outcomes in children with OSA, and the results are inconsistent [30, 31]. Similarly, there is a lack of synthesis on the impact of PAP therapy on BP outcomes in children with OSA.
There are concerns among pediatric specialists about early kidney damage in children with OSA, which may also contribute to hypertension [32]. However, the association between OSA and renal outcomes in children is not as clear as in adults [33], as there is no systematic review summarizing the evidence on this topic.
The primary objective of this systematic review is to summarize the current evidence on the association between childhood OSA and systemic BP and renal outcomes. A secondary objective is to investigate the potential impact of OSA treatments on BP outcomes. This synthesis will help determine whether respiratory interventions to address OSA have the potential to improve cardiovascular health.
2. Methods
2.1. Study Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines [34]. The protocol has been published elsewhere [35].
2.2. Search Strategy
The search strategy (eTable 1) consisted of terms related to OSA, systemic BP (e.g., systolic/diastolic BP [SBP/DBP] and mean arterial pressure [MAP] during sleep or wakefulness), obesity, and renal function. They were combined to create a comprehensive search in Ovid Medline and then translated into Ovid Embase, CINAHL via EBSCOhost, and Wiley Cochrane Library (which includes the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, the Database of Abstracts of Reviews of Effects, the Health Technology Assessment Database, and the NHS Economic Evaluation Database). A previously validated filter for studies in pediatric populations was updated and included in the search [36]. There were no language restrictions or time limits applied to the search strategy. An update of the search was run in August 2024.
2.3. Eligibility Criteria
We included studies that focused on children and adolescents aged 0–18 years with OSA and OSA syndrome (OSAS) as defined by the American Academy of Sleep Medicine [37]. We considered all types of observational and intervention studies for inclusion, such as controlled before–after studies, cross-sectional studies, longitudinal observational studies, case–control studies, retrospective cohort research, and case series. We included studies that had control subjects (e.g., healthy controls or primary snoring) as well as those without control subjects. Furthermore, we included studies that examined OSA interventions and those that did not.
Case reports, case series with fewer than seven subjects, abstracts, comments, editorials, letters, review articles, and animal studies were excluded.
2.4. Data Management and Synthesis
Records identified by the search strategy were imported into an EndNote library (Version X9, Clarivate Analytics) after removing duplicates and conducting double screening. Two researchers independently screened the titles, abstracts, and full text to identify eligible articles. Any disagreements were resolved by a third reviewer.
Using a predesigned standardized Microsoft Excel form (Microsoft, Redmond, Washington, USA), the following data items were extracted: first author, year and country of publication, study design, follow-up duration, sample size, average age or age range of study population, exclusion criteria, definition of OSA, methods of BP measurement, type of intervention, and control subjects, if applicable.
2.5. Quality Assessment and Certainty of Evidence
The quality assessment of the included studies was independently conducted by two reviewers using the Quality Assessment Tool for Quantitative Studies [38]. Any discrepancies were resolved through consensus. The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach [39] was used to assess the certainty of the evidence at the outcome level.
2.6. Meta-Analysis
We gathered both awake and sleep measures of SBP, DBP, and MAP for meta-analysis and outcomes were pooled using random-effects models. Continuous outcomes were summarized using the mean difference between children with OSA and healthy control group (no OSA), and statistical heterogeneity was quantified by using the I^2^ statistic. Publication bias was checked using regression-based Egger test. Meta-regressions were used to examine whether certain variables (mean age, mean body mass index [BMI], percentage of male participants, obesity, and hypertension) influenced the size of the difference in BP between children with OSA and control groups or the size of the intervention effect (change in BP postintervention). All the meta-analysis was performed using STATA 18 SE software (StataCorp LLC).
3. Results
3.1. Characteristics of Included Studies
Out of the 6796 nonduplicate records initially identified by the search strategy, 324 full texts were retrieved for eligibility assessment and 52 met the inclusion criteria. The updated search yielded 1420 articles of which 34 full texts were evaluated and 12 studies were included (Figure 1).
A total of 64 studies were included, consisting of 44 observational studies and 20 interventional studies. The majority of studies were conducted in Asia (38%) and North America (36%), with a smaller proportion from Europe (16%). Over 70% of the studies were conducted in the last decade.
The definition of OSA was based on polysomnography (PSG) parameters performed under standard recommendations [37, 40], with apnea–hypopnea index (AHI) > 1 event/hour used in most studies as per standard guidelines [41]. The majority of studies categorized OSA by severity into “mild,” “moderate,” “severe,” and “moderate/severe.” The threshold for “moderate/severe” or “severe” OSA ranged from AHI > 5 to AHI > 15. Systemic hypertension was defined by BP values > 95th percentile of standardized normative data. BP readings were reported as mean (standard deviation [SD]), median (interquartile range [IQR]), percentiles, Z-scores, or BP index.
Most studies excluded patients with a priori diagnosis of systemic hypertension or those taking medications that could affect BP. The majority of studies were classified as moderate quality (eTable 2), and the certainty of evidence for outcomes was low (eTable 3).
3.2. Observational Studies
Among the 44 observational studies included (Table 1), 38 were cross-sectional and six were longitudinal [43, 46, 52, 59]. Thirty-six of these studies were prospective, with sample sizes ranging from 23 to 1689 participants. Nineteen studies included healthy children as controls, while14 studies included children with primary snoring (defined as snoring and AHI < 1).
Eighteen studies measured BP using 24-h or nocturnal ambulatory BP monitoring (ABPM) [13–15, 18, 42, 45, 51, 62–67, 69, 76–78, 80], 23 measured office BP manually by sphygmomanometer or automated oscillometric device [43, 44, 46–50, 52, 53, 55–61, 68, 70–76, 81] and six studies used continuous BP measurement via finger photoplethysmography [19, 54, 57, 72, 79, 81].
3.3. Interventional Studies
Twenty interventional studies were included (Table 2): seven before–after prospective cohorts, six before–after retrospective cohorts, and seven randomized controlled trials (RCTs). Sixteen studies evaluated AT, three studied PAP therapy including continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BPAP) [26, 89, 95], and one investigated multidisciplinary weight loss intervention [94]. Follow-up durations ranged from 3 to 24 months.
Five studies used 24-h or nocturnal BP monitoring [28, 84–89, 93], 12 measured casual BP readings [24, 26, 27, 29, 90–92, 94, 96], and three studies [82, 83, 95] did not specify the measurement method.
3.4. Childhood OSA and Systemic BP Outcomes
Children with OSA had significantly higher awake SBP (mean difference: 3.30 mmHg; 95% CI, 2.07–4.53) and DBP (1.27 mmHg; 95% CI, 0.69–1.84) compared to the healthy control group (Figures 2 and 3). Nighttime SBP (4.08 mmHg; 95% CI, 2.71–5.46) and DBP (2.12 mmHg; 95% CI, 0.96–3.27) were also elevated in children with OSA (Figures 4 and 5). Awake MAP (2.11 mmHg; 95% CI, 1.32–2.89) and sleep MAP (3.60 mmHg; 95% CI, 1.11–6.09) were higher in children with OSA (Figures 6 and 7). ABPM provided significant evidence for BP comparisons (Figures 2, 3, 4, 5, 6, and 7).
Meta-regression analyses showed that obesity was significantly associated with an increase in awake SBP (p=0.003) in children with OSA. Studies with obesity rates ≤ 50% reported mean difference in awake SBP of 2.3 mmHg (95% CI, 1.4–3.3), whereas those with obesity rates > 50% reported a mean difference of 6.0 mmHg (95% CI, 3.8–8.2).
3.5. Effect of AT Treatment on BP Outcomes
Seven of 11 studies assessing AT on BP outcomes [24, 28, 29, 86, 88, 90, 91] reported significant BP improvements postsurgery (3–24 months). Subgroup analyses in some studies indicated greater benefits in children with baseline systemic hypertension [24, 28, 86, 88, 91] and in nonobese school-age children [90]. Three studies [28, 88, 97] showed persistence or new-onset hypertension despite improved AHI post-AT (3–6 months).
Meta-analysis of studies reporting mean BP change after AT [24, 29, 83] showed no significant differences in SBP (−0.48 mmHg; 95% CI, −11.6 to 10.2) and DBP (−2.25 mmHg; 95% CI, −12.25 to 7.74) (eFigures 1-2).
3.6. Effect of PAP Therapy on BP Outcomes
Three studies examined BP changes following PAP therapy. Two studies [95, 98] reported significant reductions in SBP after PAP treatment. One retrospective study [95] found adequate CPAP adherence in 33 hypertensive children with OSA was associated with a significant decrease in SBP z-score percentile (−3.5 ± 2.1 SBP percentile points per 100 days), compared to the 20 children nonadherent to CPAP, who had a 5.0 ± 1.3 increase in percentile points per 100 days. Another retrospective study [98] observed a 5-mmHg SBP reduction after six months of CPAP in a group of 25 school-age children with OSA and with or without obesity at the 6-month follow-up office visit after CPAP initiation. A subgroup analyses also found that children with a higher BMI had greater decrease in SBP. A third prospective study [89], on a cohort of 25 school-age children with moderate–severe OSA (AHI > 5 events/h) and obesity initiated on CPAP or BPAP, found no significant changes in ABPM parameters (absolute BP or nocturnal BP dipping) after 12 months of PAP therapy despite normalization of AHI.
3.7. Effect of Lifestyle Intervention on BP Outcomes
Roche et al. [94] evaluated a multidisciplinary weight loss intervention in 50 adolescents with obesity and with or without sleep-disordered breathing (SDB). BP improvements were observed only in participants with SDB whose condition was normalized following a 9- to 12-month weight loss intervention.
3.8. Childhood OSA and Renal Outcomes
Two studies [3, 99] assessed urinary albumin loss in children with OSA. Neither studies found an association between childhood OSA and albuminuria.
4. Discussion
This systematic review synthesized the existing literature on the association between childhood OSA and systemic BP, and kidney function. It also examined the effects of OSA treatment on BP outcomes in children. To our knowledge, this study is the most recent and largest in sample size on this topic. Additionally, it is the first to systematically analyze the impact of various OSA treatments, including PAP therapy and lifestyle modification, on BP outcomes in the pediatric population, aside from AT.
Our findings indicated that children with OSA are at a higher risk of higher BP compared to healthy non-OSA controls. However, treatment of OSA either with AT or PAP therapy alone did not always demonstrate better control of BP values on meta-analysis, despite that some studies showed encouraging results. Interventional studies continue to be limited, particularly those assessing the effect of PAP therapy and no studies were found assessing a combination of PAP and other nonsurgical treatments such as lifestyle modifications or medication management. Research on childhood OSA and renal outcomes is even more limited.
The elevated awake and sleep SBP observed in children with OSA align with prior meta-analysis that has established that moderate-to-severe childhood OSA is associated with a higher risk of adverse SBP outcomes [20]. More notably, the increased nighttime SBP and DBP further support the hypothesis that sleep disturbances associated with OSA negatively impact nocturnal BP regulation [100], a critical finding given the importance of nighttime BP as a predictor of long-term cardiovascular outcomes [101]. An important finding of this study is that the higher the prevalence of obesity in study cohorts, the greater the difference in awake SBP between children with OSA and healthy controls. This indicates that obesity exacerbates the impact of OSA on daytime BP, which is consistent with the known interaction between obesity and cardiovascular risk [61, 80, 102] in the pediatric population. The interaction and causal relationship among all three conditions is complex and likely synergistic [103, 104]. Obesity likely contributes to these differences through various mechanisms, including increased sympathetic nervous system activity, altered chemoreceptor sensitivity, and the proinflammatory state associated with excess adipose tissue [105, 106]. Children with both OSA and obesity may thus experience an amplified cardiovascular burden compared to children with OSA alone [15, 42, 55], highlighting the importance of addressing weight management in conjunction with OSA treatment to mitigate these risks.
ABPM provided consistent evidence for the BP comparisons. This is not surprising as ABPM is superior to office BP when evaluating abnormalities in BP during sleep [103], and, therefore, has shown stronger correlation with OSA [17]. ABPM identifies patients with masked hypertension and decreased physiological nocturnal dipping, an early sign of impaired BP control in children with OSA [14, 77, 80]. Performing an ABPM is, therefore, the recommended option in these children.
Evidence regarding reversible changes in BP after OSA treatment alone in children is more limited and less clear, and consistent with previous meta-analysis by Kang et al. [30] that also did not find a significant decrease in office or ABPM SBP or DBP after AT. This is not surprising considering the limited number of studies that could be meta-analyzed and the fact that most studies excluded children with previously diagnosed systemic hypertension, making it difficult to demonstrate significant impact of OSA treatment on BP outcomes. Further interventional studies in children with diagnosed systemic hypertension and OSA are, indeed, needed, to analyze the impact of OSA treatment on BP outcomes alone and/or in combination with other measures such as lifestyle changes and/or BP medication.
Another area of uncertainty is the progression of cardiovascular disease in children with OSA and BP post-OSA treatment. Some studies [28, 83, 86, 88] unexpectedly showed short-term significant increases in BP postoperatively in nonhypertensive children at baseline. An increase in BMI and somatic growth after surgery is a concern. However, no longitudinal studies have looked at the impact of OSA treatment long term as well as on the further development of hypertension during childhood and into adulthood. Further longitudinal studies are needed using appropriate measures to assess changes in BP after OSA treatment with AT, PAP therapy, or in combination with lifestyle changes and/or BP medication control.
In adults, a previous meta-analysis found that CPAP treatment was associated with a significant decrease in both day and night BP in patients with resistant hypertension [107], although with a low effect size [108]. This effect was not observed in our pediatric meta-analysis, partially due to the limited evidence available as observed in previous review [109]. Of the three studies analyzed, two reported significant improvements in SBP following PAP treatment. However, Katz's [89] study did not demonstrate a significant change in BP after PAP therapy, though there were trends indicating clinically relevant improvements in systolic BP load. The authors acknowledged that the small sample size, high attrition rate, and lack of ethnic diversity could have contributed to the lack of significant findings. Given the relatively few studies assessing the impact of PAP therapy on BP outcomes, further research is needed. Specifically, multi-ethnic cohort longitudinal studies with larger sample sizes and extended follow-ups would be beneficial to better understand the association between PAP therapy and BP outcomes. Furthermore, only 2 studies were found assessing the association between OSA and kidney outcomes, which might be due to the fact that kidney dysfunction associated with childhood OSA continues to be uncommon in children compared to adults.
Detecting and treating hypertension in children and youth is crucial to tackle its long-term cardiovascular morbidity. Previous data on BP tracking from childhood to adulthood demonstrate that higher BP in childhood correlates with hypertension in adulthood [110], a major contributor to cardiovascular morbidity and mortality worldwide [111]. Children with OSA, especially if there is concomitant obesity, should have their BP monitored, ideally by ABPM [112] for early detection of hypertension and appropriate multidisciplinary management. Conversely, children with hypertension should be assessed for symptoms of OSA, especially if there is concomitant obesity.
This systematic review was limited by the presence of moderate risk of bias in most included studies. Additionally, the included studies excluded children with prior diagnosis of hypertension or those taking antihypertensive medications, which introduces a risk of bias by potentially eliminating patients with more severe forms of hypertension. This likely reduced the likelihood of detecting significant associations. Most studies included in the analysis were observational, which may lower the certainty of the evidence presented. However, given the lack of RCTs in this field, observational studies provide valuable insights into the studied outcomes.
5. Conclusion
Childhood OSA is associated with deleterious BP outcomes, with obesity being a major contributor to both significant elevation of daytime SPB and OSA. OSA treatment (AT or PAP) alone, however, did not show clear effects on reducing BP outcomes, despite an encouraging trend to lower BP measures in some of the studies included in this systematic review. Given the worldwide increasing incidence of systemic hypertension in children and youth and the demonstrated correlation between childhood and adulthood hypertension, children and youth with systemic hypertension should be assessed for OSA symptoms and vice versa, especially if there is concomitant obesity, and contributing factors should be properly managed multidisciplinary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Thoracic Society Standards and Indications for Cardiopulmonary Sleep Studies in Children American Journal of Respiratory and Critical Care Medicine 1996153866878856414710.1164/ajrccm.153.2.8564147 · doi ↗ · pubmed ↗
- 2Bixler E. O. Vgontzas A. N. Lin H. M. Sleep Disordered Breathing in Children in a General Population Sample: Prevalence and Risk Factors Sleep 200932673173610.1093/sleep/32.6.7312-s 2.0-6524915499519544748 PMC 2690559 · doi ↗ · pubmed ↗
- 3Verhulst S. L. Van Hoeck K. Schrauwen N. Sleep-Disordered Breathing and Proteinuria in Overweight and Obese Children and Adolescents Hormone Research in Paediatrícs 200870422422910.1159/0001515942-s 2.0-5084911877718772595 · doi ↗ · pubmed ↗
- 4Dayyat E. Kheirandish-Gozal L. Gozal D. Childhood Obstructive Sleep Apnea: One or Two Distinct Disease Entities? Sleep Medicine Clinics 20072343344410.1016/j.jsmc.2007.05.0042-s 2.0-6064909294118769509 PMC 2084206 · doi ↗ · pubmed ↗
- 5Kohler M. J. van den Heuvel C. J. Is There a Clear Link Between Overweight/Obesity and Sleep Disordered Breathing in Children? Sleep Medicine Reviews 200812534736110.1016/j.smrv.2008.04.0082-s 2.0-5124912222318790410 · doi ↗ · pubmed ↗
- 6Marin J. M. Agusti A. Villar I. Association Between Treated and Untreated Obstructive Sleep Apnea and Risk of Hypertension JAMA 2012307202169217610.1001/jama.2012.34182-s 2.0-8486137597222618924 PMC 4657563 · doi ↗ · pubmed ↗
- 7Yaggi H. K. Concato J. Kernan W. N. Lichtman J. H. Brass L. M. Mohsenin V. Obstructive Sleep Apnea as a Risk Factor for Stroke and Death New England Journal of Medicine 2005353192034204110.1056/nejmoa 0431042-s 2.0-2774447429916282178 · doi ↗ · pubmed ↗
- 8Peppard P. E. Young T. Palta M. Skatrud J. Prospective Study of the Association Between Sleep-Disordered Breathing and Hypertension New England Journal of Medicine 2000342191378138410.1056/nejm 2000051134219012-s 2.0-003463647710805822 · doi ↗ · pubmed ↗