The Becker Method: A Straightforward Method for Accurate Dental Age Assessment in the Clinical Setting
Maya Dora Davidovitch, Avi Leibovich, Stella Chaushu

TL;DR
The Becker method is a practical and accurate way to assess dental age in children and adolescents compared to the Demirjian method.
Contribution
This study evaluates and validates the Becker method as a simpler and more accurate alternative to existing dental age assessment techniques.
Findings
The Becker method showed less overestimation of dental age compared to the Demirjian method.
The Becker method had an average overestimation of 0.659 years for females and 0.123 years for males.
The method is user-friendly and suitable for clinical settings without sacrificing accuracy.
Abstract
Background: Accurate dental age (DA) assessment is important in the clinical decision-making process of pediatric dentists and orthodontists. While clinical methods based on tooth emergence are inaccurate, techniques using tooth calcification for assessing DA are more precise but impractical for clinical use due to their complexity. Becker proposed a more straightforward and practical method for accurate DA assessment based on root apex closure. However, its level of accuracy has not been determined. Aim: To evaluate the reliability of the Becker method by comparing it to the Demirjian method. Design: This cross-sectional study analyzed panoramic radiographs from a cohort of 377 Israeli children and adolescents aged between 8 and 15 years. DA was evaluated using the Demirjian and Becker methods and compared with the chronological age (CA) of each participant. Results: Both methods…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
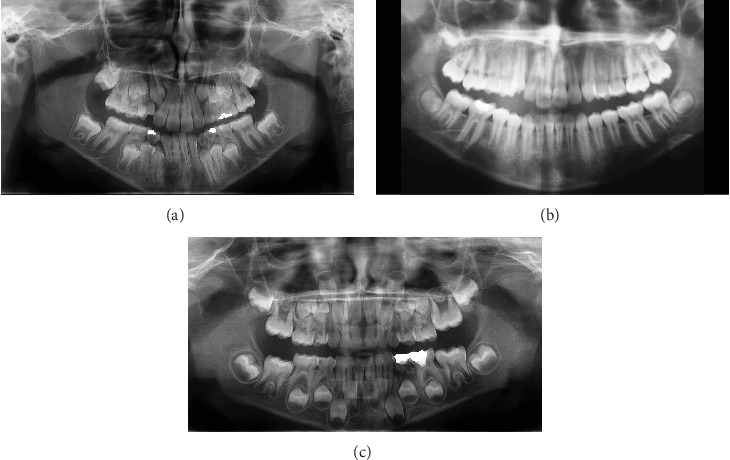 Figure 1
Figure 1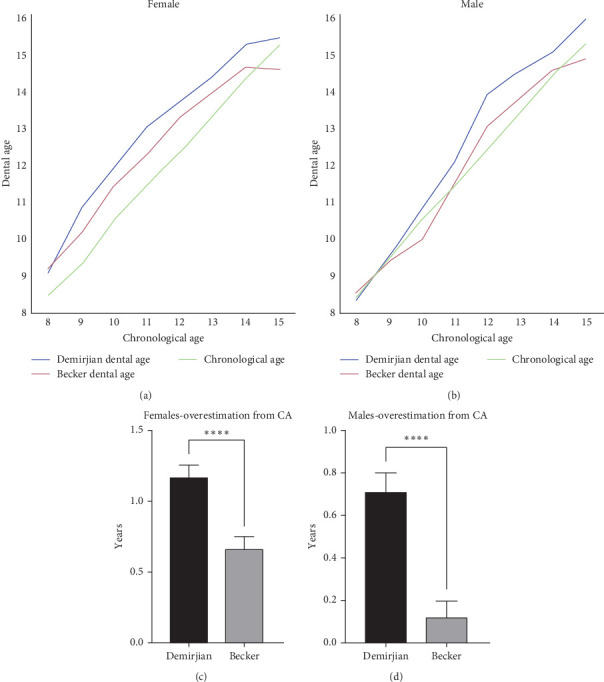 Figure 2
Figure 2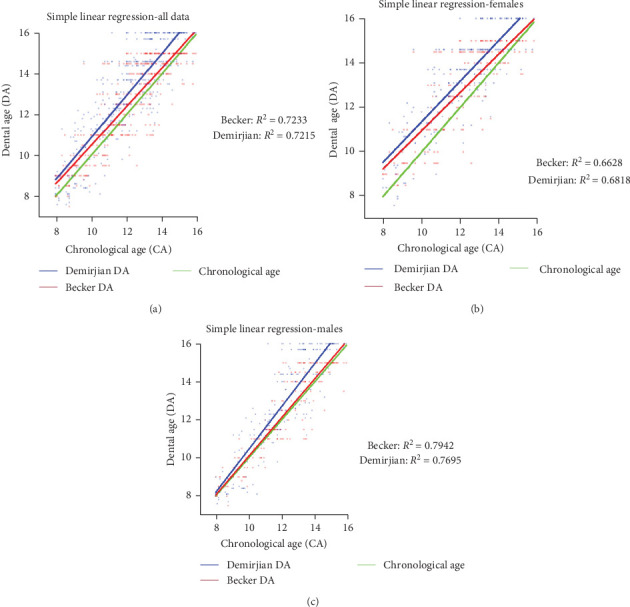 Figure 3
Figure 3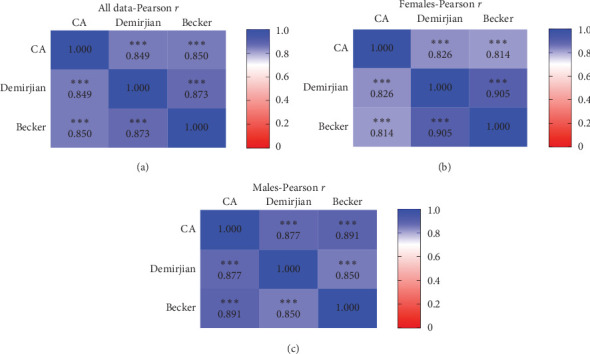 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Anthropology and Bioarchaeology Studies · dental development and anomalies · Dental Radiography and Imaging
Summary
- • Evaluating dental age (DA) holds significant importance in the clinical decision-making process for both orthodontists and pedodontists.
- • DA assessment based on teeth eruption is often inaccurate and misleading. More accurate methods based on tooth formation are too complex for clinical implementation.
- • The Becker method is a practical approach for assessing DA in clinical settings, based on tooth formation rather than eruption, making it more accurate.
1. Introduction
Methods to determine the dental age (DA) of children and adolescents are of great value, especially in pediatric dentistry and orthodontics [1, 2]. Before initiating treatment, clinicians assess the extent of dental development by determining the patient's DA. The evaluation of DA is crucial in effectively planning orthodontic treatment. It aids in assessing the timing of tooth eruption, and identifying teeth that are impacted [3]. DA assessment helps in determining the optimal timing for orthodontic treatment, including the selection of fixed or removable appliances and planning for orthodontic tooth extractions. Assessing DA is also important for determining the most appropriate timing and options for treatment in pediatric dentistry. This includes decisions regarding the extraction of over-retained primary teeth, space maintenance strategies, and the optimal timing for the extraction of severely compromised permanent first molars to facilitate spontaneous space closure [4]. Furthermore, DA assessment is essential in forensic science for determining chronological age (CA), as there exists a strong correlation between CA and DA [5–8].
Assessment of DA can be determined radiographically or by direct clinical visualization of the dentition. The latter method is based on the emergence of teeth in the oral cavity, as observed clinically without the need for auxiliary diagnostic tools. This method has validity because it has been shown that the average timing of the eruption of teeth is fairly constant and can be employed in ascertaining an age range for a given individual. However, it would be a mistake to depend solely on the timing of tooth eruption as a method for estimation. While different groups of teeth typically erupt at specific times (with half to two-thirds of the final root length) [9], this process can be affected by local and environmental factors such as habits, available space in the dental arch, extraction or early loss of primary teeth, and tipping or impaction of teeth, eventually leading to significant variations in eruption timing [3, 10, 11].
In contrast to tooth emergence, tooth calcification is a continuous process that is assessed by permanent records such as dental radiographs and is unaffected by the local conditions mentioned above. In addition, the stages of calcification of the permanent dentition during dental development are predominantly governed by genetic factors rather than environmental influences [12–17]. Therefore, assessment of dental calcification has been showed to be a more accurate method of determining DA than tooth emergence.
Several radiographic methods to estimate DA have been proposed. These methods define the stages of mineralization of each individual tooth as observed in dental radiographs, and describe them in words and in illustrated diagrams and tables [18]. Empirical definitions of these stages were displayed in the classic works of Schour and Massler [19], Moorrees et al. [14, 20], Nolla [13], Demirjian et al. [21], Koyoumdjisky-Kaye et al. [22], and other notable sources [3].
1.1. The Demirjian Method
The most frequently used and accepted analysis of DA assessment is the Demirjian's method [21]. Originally described in 1973 by Demirjian, Goldstein, and Tanner, this method is based on a large French-Canadian sample with DA estimation being determined by the development of the permanent dentition of a subject's mandibular left quadrant of permanent teeth, excluding the third molars. Tooth formation is ranked according to eight stages (A–H). The determined developmental stage for each tooth is assigned a biologically weighted score. The data is converted to a DA by using available standard tables for each gender. The cumbersome nature of the Demirjian method has made it unsuitable for practical use in a clinical setting, thus making it more appropriate as a tool for clinical research.
1.2. Becker's Method
Becker proposed a simpler method of DA assessment in 1997 and 1998 [3, 23, 24] with the express purpose of enabling DA diagnosis quickly, at the orthodontist's chairside. The method is considerably simpler, as it does not require tables or calculations. Instead, it diagnoses directly from a qualitative examination of the panoramic radiograph or full-mouth periapical survey. The Becker method requires the observer to be familiar with the average CAs for the permanent teeth's emergence in a specific population. This method differs from other methods by its focus on the identifiable completion of formation and closure of the root apices of the teeth, which normally occur approximately 3 years after the tooth has achieved functional eruption [25]. The disappearance of the root-forming dental papilla which signifies the closure of the root apex is the most accurate feature to recognize, identify and diagnose; therefore, it can be used as a reliable baseline from which to begin the evaluation of the patient's DA [3, 23, 24]. The process follows a stepwise approach where the teeth are categorized into groups according to their eruption timing (Table 1). The DA is determined based on the last group of teeth that exhibit closed apices. This is most reliably determined when a subject has reached at least the DA of 9 years, because prior to this, the apices of all unerupted and erupting permanent teeth are still open.
Thus, in Figure 1A the DA is 9.5 as the permanent molars and mandibular lateral incisors are the final set of teeth to exhibit closed apices. Likewise, in older individuals (Figure 1B), where the maxillary central and lateral incisors are the final set of teeth with closed apices, the estimated DA ranges from 10.5 to 11.
Prior to reaching the DA of 9 years (Figure 1C), none of the permanent teeth will have apexified roots. Thus, the observer need to estimate percentages of root development, crown formation and, in much younger children, even the initiation of crown calcification. Assessing age in this manner is more subjective and less accurate. In Figure 1C the root formation in the lower central incisors and 1st permanent molars/lateral incisors is approximately 2/3 to 1/2 respectively indicating a DA of around 6 years.
The primary goal of this study is to compare the Becker method, which is based on the timing of root apex closure, to the Demirjian method in determining DA in relation to CA, in order to evaluate the reliability of the former.
2. Materials and Methods
2.1. Subjects
Panoramic radiographs of 377 subjects who presented for treatment in the Department of Orthodontics postgraduate clinic at the Hebrew University Faculty of Dental Medicine were utilized to determine DA in this cross-sectional investigation. Inclusion criteria for subjects in this study were: 8–15 years of age, with high-quality radiographic diagnostic records. Subjects were excluded if they had a history of dental trauma, congenitally missing teeth, or syndromes, or if they had undergone any previous orthodontic treatment. The sex and age distribution of the study sample are shown in Table 2. The study received ethical approval from the Helsinki Committee of Hadassah University Hospital (Approval No. 0129-22).
Each subject's CA at the time of being x-rayed was calculated.
DA was estimated according to the methods described by Demirjian et al. [21] and Becker [3]. These evaluations were conducted by the main examiner (author MDD), who was blinded to the CA values. Initially, the examiner assessed the DA using one technique and then, several weeks later, used the second method to analyze the data.
2.2. Statistical Analysis
Differences between DA and CA were analyzed using the Wilcoxon signed rank test for paired samples with a non-normal distribution. A p-value of <0.05 was considered statistically significant. Simple linear regression analysis and correlation (Pearson's r coefficient) was used to study the association between DA and CA for girls and boys separately, as well as for the whole group. These analyses were performed using Prism version 10.2.2, GraphPad Software, Boston, Massachusetts, USA.
2.3. Intra and Interobserver Reliability
A randomly selected 25 male and female samples each (n = 50) were first assessed twice during an interval of at least 2 weeks, with repeat evaluations by another examiner (AL). Both examiners were blinded to the CA values. To evaluate reproducibility and accuracy, both interobserver and intraobserver assessments were performed using intraclass correlation coefficient (ICC). The calculation was performed using the intraclass_corr() function from the pingouin library In Python [26].
3. Results
Reliability of the measurements within the same examiner (Intraexaminer—Table 3) was calculated using ICC [26] and showed high values (0.944–0.966) for both examiners using both Demirjian and Becker methods. Consistency between examiners (Interexaminer—Table 4) was also calculated using ICC [26] and were high for both the Demirijian and Becker methods with coefficient scores ranging from 0.918 to 0.971.
Comparison between Demirjian's and Becker's DA estimation methods were analyzed separately for females and males, as well as collectively for both genders across the different age groups. The results are displayed in Tables 5 and 6, for females and males, respectively. The mean CA of the study group was 12.104 (SD = 1.938) years for females, 12.056 (SD = 2.042) years for males, and 12.08 (SD = 1.989) years for the entire study group.
As shown in Figure 2, and Tables 5 and 6, both the Demirjian and Becker methods show an overall overestimation of the DA compared to the CA, for both females and males, with the Demirjian method exhibiting a significantly greater overestimation (Figure 2C,D) compared to the Becker method. It was also found that several exceptions were seen, namely, that in the 9, 10, 15 male and 15 female age group (Tables 5 and 6), the Becker methods did not exhibit an overestimation of CA while the Demirjian method did.
Simple linear regression was used to evaluate the relationship between the two DA calculation methods and CA (Figure 3). Upon examining the graph representing all patients irrespective of gender, both the Demirjian and Becker methods exhibit similar goodness-of-fit values (Figure 3A; R^2^ = 0.72). Slightly lower values are observed when analyzing the graphs based on gender, with higher values observed in the males group (Figure 3B,C). However, both methods still show similar values. The slopes of the graphs are quite similar and closely resemble the CA values. In the graph representing all patients, the slopes for the Demirjian and Becker methods were 1.03 and 0.946, respectively, and were not significantly different (p=0.07). In the female group, these values were 0.9102 and 0.8587 (p=0.02), respectively, and in the male group, the values were 1.129 and 1.019 (p=0.01), respectively. When compared to the slope of CA (value = 1), both methods exhibit a good level of fitness to the CA graph.
To better assess the correlation between the DA calculation methods and the CA, we conducted a Pearson r correlation test (Figure 4). In the graph representing all patients irrespective of gender, there was a strong, positive, and significant correlation between the DA methods and the CA, with correlation coefficients of 0.849 (p < 0.0001) for Demirjian and 0.85 (p < 0.0001) for Becker (Figure 4A). Similarly, in the female group, the correlation coefficients were 0.826 (p < 0.0001) and 0.814 (p < 0.0001), respectively (Figure 4B). The male group exhibited higher values, with correlation coefficients of 0.877 (p < 0.0001) and 0.891 (p < 0.0001), respectively (Figure 4C). We observed similar coefficients values when directly comparing the Demirjian method to the Becker method, ranging from 0.85 to 0.905 (p < 0.0001) depending on the specific group analyzed (Figure 4).
4. Discussion
Accurate assessment of DA is essential for both dental and forensic applications. Evaluation of the accuracy of DA estimation techniques commonly involves a comparison between the estimated DA and the actual CA [7, 27–29]. Besides accuracy, the DA estimation technique should be simple, reproducible, and easily adaptable to different populations.
Both the Demirjian method and the Becker method exhibited high ICC values for DA assessment (Tables 3 and 4), indicating consistent results between observers. Consistent outcomes were also observed when the same observer conducted measurements at different times.
Given that the examiners in our study had varying levels of experience, the remarkable reliability we observed among them implies that extensive experience is unnecessary for effectively using either method.
Numerous studies have already showed a significantly high correlation between DA assessment and CA [8]. In our study, we show similar results using the Demirjian and Becker methods for both genders, with correlation coefficients reaching up to 0.9.
Our results also revealed a consistent trend of overestimating DA compared to CA when applying the Demirjian method, consistent with previous reports [30–32]. Notably, Demirjian et al. [21] acknowledged the potential limitation of their standards, derived from a sizable sample of mid-20^th^-century French-Canadian origin, and suggested caution when applying the method to different populations, advocating for potential adjustments. Existing literature indicates the necessity of population-specific calibration for DA assessment methods, given the variability in dental development across diverse populations and also over time due to secular trends [33].
Comparison of the Becker to the Demirjian methods in this study revealed that both tend to overestimate DA compared to CA (Figure 3), however, the Becker method demonstrated a significantly smaller mean difference from CA in both genders (The average overestimation of Becker method was 0.659 years for females and 0.123 years for males, and of Demirjian method 1.167 and 0.713 years, respectively, Tables 5 and 6; Figure 2C,D).
In forensic medicine, the generally accepted margin of error between estimated DA and CA for individuals ranges from 0.5 to 1.0 years [7]. While comparable data are not available in orthodontics and pedodontics, it is reasonable to assume a similar range, as greater discrepancies could significantly influence clinical decision-making processes that rely on DA assessments. Our study showed that for both males and females of all ages, the Becker method estimated DA within an acceptable range of CA. However, the Demirjian method showed greater discrepancies in several age groups (Tables 5 and 6). Therefore, the Becker method appears more accurate for estimating DA in the Israeli population.
Esan et al.'s [34] meta-analysis of studies comparing the Willems and Demirjian methods showed similar results. Willems, an improved method using a modern European reference population and revised maturity scores, addresses the Demirjian method's overestimation of DA. Their findings indicated Willems provided a better fit to CA across diverse populations, with average overestimations of 0.29 years (females) and 0.26 years (males), compared to Demirjian's 0.72 and 0.62 years, respectively [34].
Similarly, the Becker method's superiority likely stems from using contemporary Israeli eruption data [22] and its methodological simplicity as the Becker method focuses on the easily identifiable and most reliable feature—root apex closure. This biological landmark is less subjective than the complex staging system used in the Demirjian method, potentially reducing assessment variability.
The Becker method's simplicity lies not only in its ability to calculate DA effortlessly but also in its independence from fixed tables and figures, unlike other methods. Adapting the Demirjian method to any population is cumbersome, requiring changes to all tables and illustrations; however, the Becker method's flexibility allows easy adaptation to various populations by simply updating eruption timing data within the stepwise assessment, based on available population-specific data [33]. Such updates, however, require validation through additional research.
We also discovered additional trends in different age groups. One notable finding was that the Becker method underestimated DA at the age of 15. This discrepancy could be attributed to the Demirjian method's extension beyond the age of 15, a range surpassing the limit of the Becker method, reaching up to the age of 16 (Tables 5 and 6, and Figures 2 and 3).
The limitations of this study include potential sample population bias, as the research was confined to Israeli children seeking orthodontic treatment who had panoramic radiographs available. This may restrict the generalizability of the findings to other ethnic groups. Additionally, in children below the age of nine, where the Becker method's predictive accuracy might be weaker since none of the teeth display closed apices, making assessment is more challenging (Figure 1C; Tables 5 and 6). Although our data did not show a decrease in accuracy of the Becker method for ages below nine, it is important to note that this age group was under-represented since it is typically less prevalent in orthodontic populations due to their dental developmental stage and presents unique challenges for age estimation methodologies. The Becker method should therefore be used cautiously with younger children.
5. Conclusion
Both the Becker and Demirjian methods demonstrated a consistent but significant overestimation of DA up to age 15, with the Becker method showing the closer agreement with CA. The findings presented herein suggest that the Becker method may be considered as a comparatively simple and reliable alternative, encouraging further exploration of its application in diverse clinical settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cruz-Landeira A. Linares-Argote J. Martinez-Rodriguez M. Rodriguez-Calvo M. S. Otero X. L. Concheiro L. Dental Age Estimation in Spanish and Venezuelan Children. Comparison of Demirjian and Chaillet’s Scores International Journal of Legal Medicine 2010124210511210.1007/s 00414-009-0380-52-s 2.0-7764923243319859725 · doi ↗ · pubmed ↗
- 2Maber M. Liversidge H. M. Hector M. P. Accuracy of Age Estimation of Radiographic Methods Using Developing Teeth Forensic Science International 2006159 Suppl 1S 68731653358410.1016/j.forsciint.2006.02.019 · doi ↗ · pubmed ↗
- 3Becker A. General Principles Related to the Diagnosis and Treatment of Impacted Teeth Orthodontic Treatment of Impacted Teeth 20121910.1002/97811187096412-s 2.0-84891583635 · doi ↗
- 4Aldahool Y. Sonesson M. Dimberg L. Spontaneous Space Closure in Patients Treated With Early Extraction of the First Permanent Molar: A Retrospective Cohort Study Using Radiographs The Angle Orthodontist 202494218018610.2319/061923-423.138381800 PMC 10893924 · doi ↗ · pubmed ↗
- 5Green L. J. The Interrelationships Among Height, Weight and Chronological, Dental and Skeletal Ages The Angle Orthodontist 1961313189193
- 6Rozylo-Kalinowska I. Kolasa-Raczka A. Kalinowski P. Relationship Between Dental Age According to Demirjian and Cervical Vertebrae Maturity in Polish Children The European Journal of Orthodontics 2011331758310.1093/ejo/cjq 0312-s 2.0-7955153416620558591 · doi ↗ · pubmed ↗
- 7Sobieska E. Fester A. Nieborak M. Zadurska M. Assessment of the Dental Age of Children in the Polish Population With Comparison of the Demirjian and the Willems Methods Medical Science Monitor 2018248315832110.12659/MSM.9106572-s 2.0-8505656338030449880 PMC 6256839 · doi ↗ · pubmed ↗
- 8Demirjian A. Buschang P. H. Tanguay R. Patterson D. K. Interrelationships Among Measures of Somatic, Skeletal, Dental, and Sexual Maturity American Journal of Orthodontics 198588543343810.1016/0002-9416(85)90070-32-s 2.0-00223831293864376 · doi ↗ · pubmed ↗