Recurrent intra-mural esophageal abscess as a complication of untreated eosinophilic esophagitis
Marianne Hupé, Amaury DʼAngelo, Arthur Berger, Frank Zerbib

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
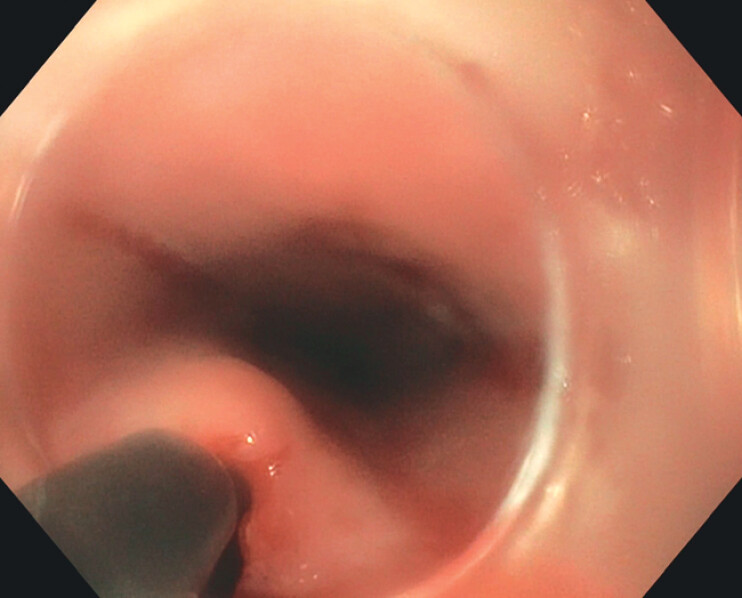 Fig. 1
Fig. 1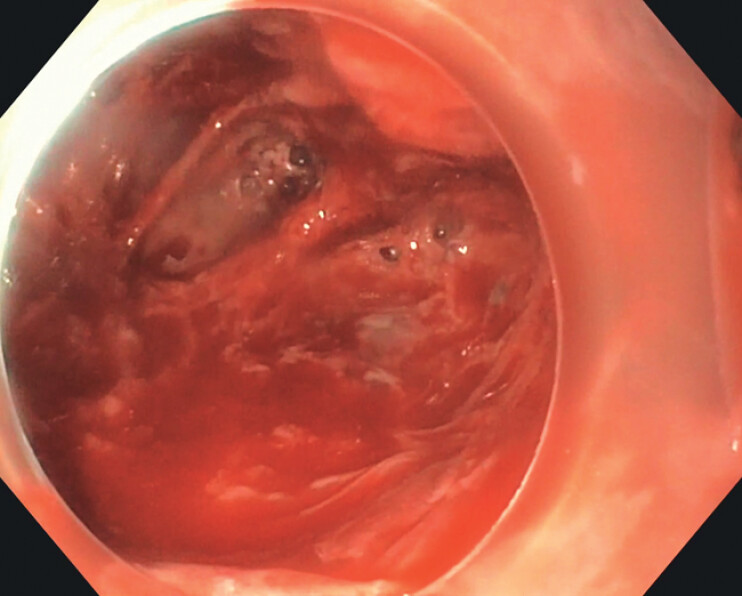 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Esophagitis · Esophageal and GI Pathology · Eosinophilic Disorders and Syndromes
Eosinophilic esophagitis (EoE) is a condition characterized by abnormal infiltration of the esophageal mucosa with eosinophils, leading to symptoms such as dysphagia. Common complications, often seen in undertreated cases, include fibrosis-related issues such as food impaction and strictures 1 . We present the case of a patient born in 1999 who, in spring 2021, was admitted with septic dysphagia, leading to the diagnosis of an intramural esophageal abscess. Endoscopy revealed a mucosal tear located 25 cm from the superior dental arch (SDA), while histology confirmed esophageal eosinophilic infiltration exceeding 20 eosinophils per high-power field (HPF). The abscess was resolved with antibiotic therapy, and the patient was prescribed proton pump inhibitors (PPIs). However, due to poor treatment compliance, subsequent gastroscopies revealed a stricture, which required dilation in September 2021.
In March 2022, the patient was readmitted for recurrent septic dysphagia. A computed tomography scan revealed another esophageal abscess. Endoscopy ( Video 1 ) showed a secondary opening at 30 cm from the SDA, overlying a parietal bulge extending to 36 cm ( Fig. 1 ). Spontaneous pus drainage was facilitated using a Hook knife, followed by irrigation for cavity cleansing ( Fig. 2 ).
Endoscopic drainage of intramural abscess related to eosinophilic esophagitis.
Intramural cavity aspect after endoscopic drainage.
Endoscopic view of an intramural esophageal abscess, with commentary, before and after drainage using a Hook knife.Video 1
By May 2022, the patient was asymptomatic and compliant with PPI therapy; however, endoscopy revealed esophageal rings, and histology showed persistent eosinophilic infiltration. His treatment was switched to orodispersible budesonide.
In July 2022, the patient presented again with dysphagia. Endoscopy revealed grade C esophagitis and an aggravating stricture, which was dilated to 17 mm using a bougie. Combination therapy with PPIs and budesonide was initiated. A follow-up in September 2022 showed a resolution of esophagitis and a decrease in eosinophilic infiltration to nine HPF. The patient remains asymptomatic.
This case highlights the complexity of managing EoE, a condition potentially linked to reflux, and illustrates a rare complication underscoring the importance of achieving histological remission.
Endoscopy_UCTN_Code_CCL_1AB_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.