Endoscopic full-thickness resection: precision and efficacy in treating a giant duodenal stromal tumor
Jiang Du, Yuan Gao, Lifan Zhang, Qiongying Zhang, Bing Hu, Yi Mou

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
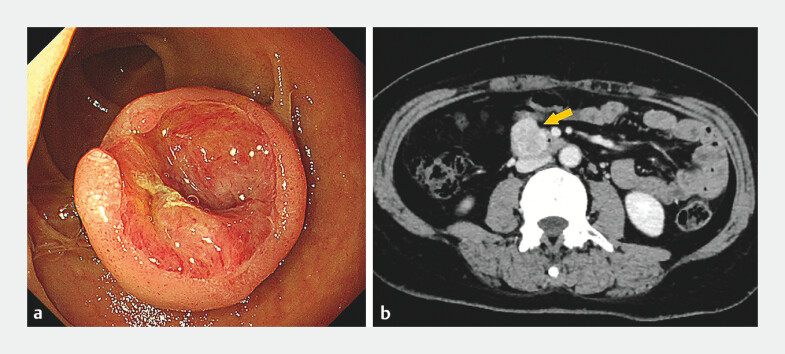 Fig. 1
Fig. 1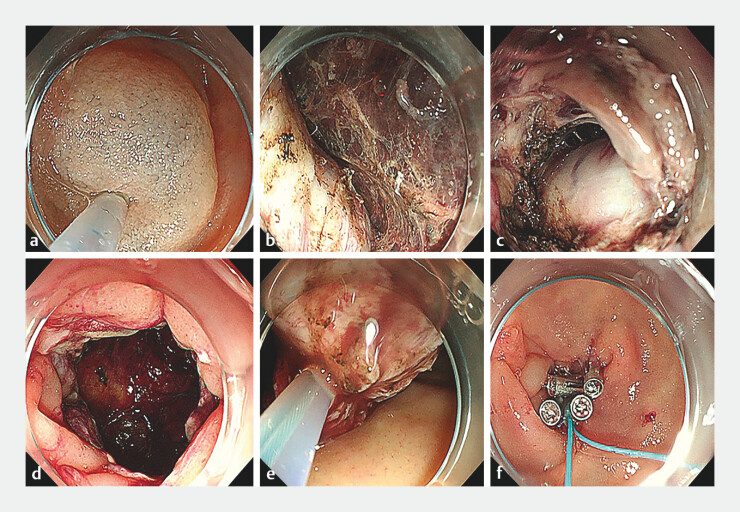 Fig. 2
Fig. 2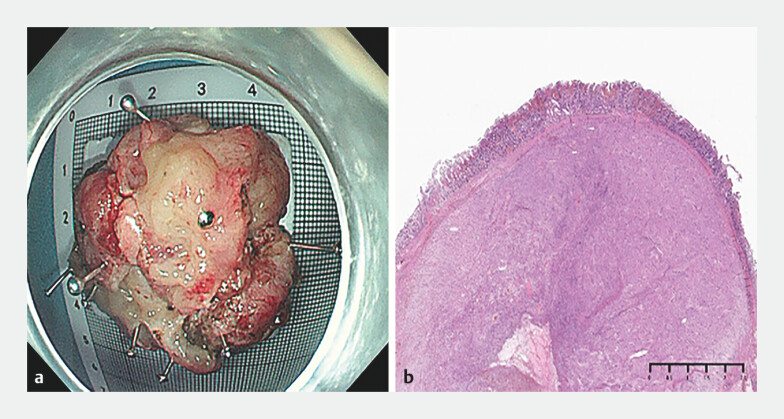 Fig. 3
Fig. 3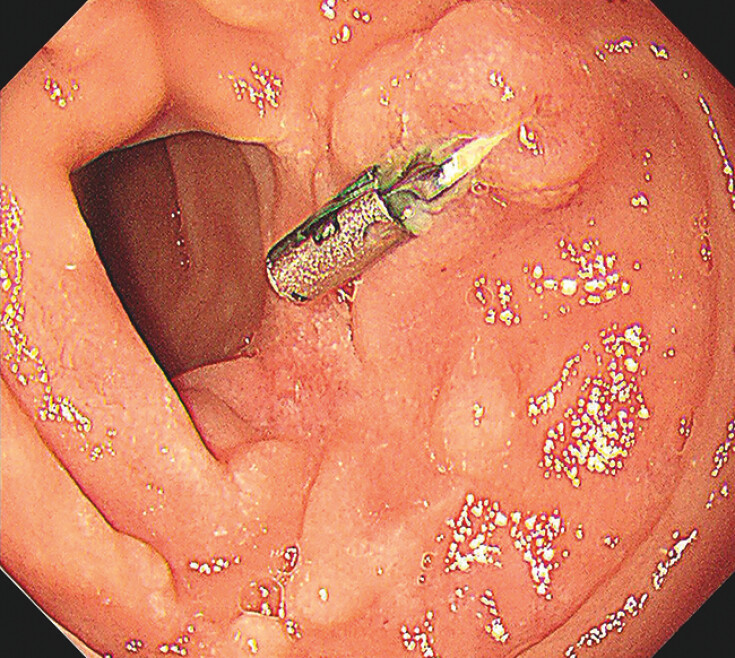 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastric Cancer Management and Outcomes · Gastrointestinal disorders and treatments
Duodenal stromal tumors, a rare subset of gastrointestinal stromal tumor (GIST), have traditionally been managed by surgical resection 1 ; however, owing to the complex anatomy of the duodenum, surgical approaches such as pancreaticoduodenectomy are associated with high morbidity and poor long-term outcomes 2 3 . Endoscopic full-thickness resection (EFTR) is emerging as a promising minimally invasive technique for treating gastrointestinal tumors 4 . Here, we present a case demonstrating the successful application of EFTR in treating a giant duodenal stromal tumor.
A 47-year-old woman presented with melena. Gastroscopy revealed a 2-cm submucosal lesion with surface ulceration in the duodenum ( Fig. 1 ). Pathologic examination of a biopsy suggested it was a GIST. Given the patient’s condition, endoscopic dissection was chosen as the treatment option ( Fig. 2 ; Video 1 ). First, a submucosal injection was carried out to facilitate the dissection. The tumor was then dissected layer by layer, and it was found that the tumor extended outside the lumen. An EFTR was performed until the tumor was completely resected. After that, the defect was closed with a double-layer purse-string suture. A nylon loop and titanium clips were used for the closure. Abdominal paracentesis was performed to evacuate intra-abdominal gas, and a nasoenteric tube was inserted for gastrointestinal decompression.
Preoperative examination of the duodenal lesion showing: a the appearance on gastroscopy with white light; b a contrast-enhanced computed tomography image suggestive of a gastrointestinal stromal tumor (yellow arrow).
Endoscopic images during endoscopic full-thickness resection for a duodenal stromal tumor showing: a submucosal injection being performed; b layer by layer resection of the tumor; c extension of the tumor outside the lumen; d continued full-thickness incision until the tumor was completely dissected; e removal of the tumor using a snare; f closure of the defect with a double-layer purse-string suture.
Endoscopic full-thickness resection is performed to precisely and effectively resect a giant duodenal stromal tumor.Video 1
The resected specimen measured approximately 4.0 × 3.0 × 2.0 cm. Postoperative pathology confirmed it to be a GIST, with R0 resection ( Fig. 3 ). During a 2-year follow-up period, there were no complications, nor evidence of tumor recurrence or metastasis ( Fig. 4 ).
Appearance of the resected specimen, which was confirmed to be a gastrointestinal stromal tumor: a macroscopically; b histopathologically with hematoxylin and eosin (H&E) staining.
Appearance of the wound on follow-up gastroscopy 6 months after endoscopic full-thickness resection.
EFTR offers a less invasive alternative to traditional surgery for duodenal stromal tumors, particularly addressing the high morbidity associated with pancreaticoduodenectomy. This case highlights the potential of EFTR in treating duodenal stromal tumors, providing a new treatment option with reduced trauma and better prognosis.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Casali PG Blay JY Abecassis N Gastrointestinal stromal tumours: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 202233203310.1016/j.annonc.2021.09.00534560242 · doi ↗ · pubmed ↗
- 2Uchima H Garsot E Colán-Hernández J Endoscopic full-thickness resection of a duodenal gastrointestinal stromal tumor with extraluminal component: the usefulness of traction and sutures Endoscopy 202254 E 730E 73110.1055/a-1773-026035272380 · doi ↗ · pubmed ↗
- 3Chou CK Chen CC Tai CM Defect closure with endoscopic suturing improves endoscopic full-thickness resection of duodenal gastrointestinal stromal tumors Endoscopy 202355 E 688E 68910.1055/a-2072-354637142246 PMC 10159778 · doi ↗ · pubmed ↗
- 4Deprez PH Moons LMGOʼToole D Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225441242910.1055/a-1751-574235180797 · doi ↗ · pubmed ↗