Risk of relapse: TB treatment outcome associates with differentially culturable M. tuberculosis counts in sputum samples
J. Decker, G.V. Mukamolova, N. Garton, D.J. Grint, M.R. Barer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
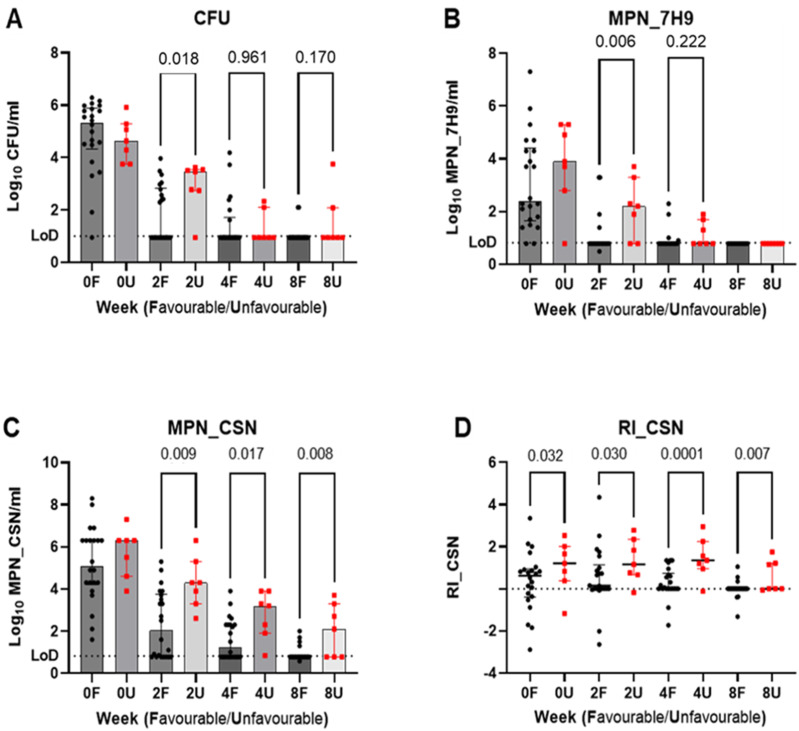 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Diagnosis and treatment of tuberculosis
Dear Editor,
Prediction of TB treatment outcomes early during therapy is highly desirable both in the management of individuals and in clinical trials. Although disease free status following six months of standard treatment provides an important frame of reference, it is recognised that some patients with drug sensitive TB relapse, with a return to active disease due to their original Mycobacterium tuberculosis (Mtb) strain. The frequency of relapse in the face of acceptable treatment adherence is not easily determined, and requires strain genome sequence analysis, but is estimated at 5%.^1^ In recent clinical trials, direct assessment of relapse rates established with 6–12 months follow-up are compared between standard treatment and test regimens to determine non-inferiority. Although the objective of shorter regimens is to achieve equivalent success rates to standard 6-month treatment it is generally recognised that shorter treatment is often associated with higher relapse rates.^2^ The accepted standard of 6–12 months follow-up to detect relapses places significant resource burden on clinical trials to differentiate between relapse and new infection, to assess programme success. Analyses capable of predicting unsatisfactory treatment outcome, including relapse, at or subsequent to treatment initiation, would therefore be extremely beneficial.
Multiple factors have been associated with TB relapse, and the ability of Mtb to form antibiotic tolerant bacilli, referred to in this context as ‘persisters’, is considered a major factor.^3^ Persisters, which survive antimicrobial exposure in vitro, are thought to contribute both to the need for prolonged treatment and subsequent relapse.^4^ We previously suggested that microscopy-based enumeration of lipid bodies containing Mtb cells in sputum (a persister-like property) might associate with unsatisfactory treatment outcomes.^5,6^ We subsequently obtained evidence supporting this in a clinical study.^7^ Although microscopy requires AFB positive sputum, differentially culturable Mtb (DCMtb) associated with a persister phenotype, are readily detected at levels down to a few bacilli per sample.^8^ DCMtb do not form colonies when inoculated onto solid media but, in liquid media supplemented with culture supernatant (CSN) harvested from exponentially growing Mtb cultures, resuscitate and grow to visible densities and can be enumerated by limiting dilution most probable number (MPN) assays. CSN contains the resuscitation promoting factor (Rpf) molecules, principally responsible for resuscitation activity but also other, yet to be defined, activities contribute.^9^ The biological activities of purified Rpfs defy stable storage, thus CSN remains the material used to demonstrate DCMtb. Relative numbers of DCMtb are quantified by the resuscitation index (RI) which reflects the excess of bacilli enabled to grow by CSN over those forming colonies (see Figure). DCMtb clearly associate with TB relapse in mice,^10^ and are shown to be tolerant to certain drugs.^8,11^ Furthermore, DCMtb have been detected in higher proportions in sputum from treated patients,^12–15^ suggesting their potential contribution to unfavourable treatment outcomes, but there is no direct evidence for this. One study described detection of DCMtb after the successful completion of treatment^12^ and a separate project demonstrated that TB sputum from patients with unfavourable outcomes always had DCMtb.^15^ However, low numbers of TB relapses in both studies precluded a robust evaluation of DCMtb abundance as a predictive indicator of TB treatment outcomes.
The TB Alliance Mark-TB Biobank (previously known as the CTB2 repository) has sputum samples from patients with fully documented treatment regimens and outcomes. In discussion with the biobank board, we first determined that DCMtb could be quantified in such samples, then agreed on the work reported here, which comprises a retrospective case-control study comparing the levels of DCMtb in serial (0, 2, 4 and 8 week) sputum samples taken from 40 sputum-positive TB patients treated with standard 2HRZE/4HR. Prior sample storage times were all in excess of 5 years.
We analysed sample sets from 29 patients, 22 with favourable and 7 with unfavourable treatment outcomes (samples from 11 individuals were excluded due to culture contamination, insufficient sample to support analysis, or failure to meet inclusion criteria). The unfavourable outcome group had clearly documented, bacteriologically confirmed re-occurrence of disease within 12 months of apparently successful treatment completion. Broadly comparable demographic and clinical features of the individuals with favourable and unfavourable outcomes are shown in the Table. Quantitative Mtb growth assays were performed by three different methods, colony forming units on agar (CFU) and limiting dilution most probable number (MPN) assays in liquid media with or without CSN supplementation (MPN_CSN and MPN_7H9, respectively). Following thawing, samples were decontaminated with NaOH, neutralised, and centrifuged pellets resuspended in Middlebrook 7H9 medium back to the original sputum volume then subjected to growth assays.^11^ Serial tenfold dilutions of the decontaminated sputum were made in 7H9 medium and in 7H9+CSN in triplicate as previously described with incubation for up to 12 weeks.^11^ The limits of detection for CFU and MPN assays were 6 and 9 propagating units/ml, respectively.
The declining patterns of counts obtained by the three growth assays are shown in Figure panels A–C. While higher MPN counts were consistently present in samples from the unfavourable group, this was most apparent with CSN addition and the RIs (Figure panel D) show a clear excess of DCMtb. This was most significant at week 4 and a ROC analysis of this data revealed an AUC of 0.805 (95% CI, 0.571–1.000, p = 0.017). Using a threshold RI value of 0.815 determined using Youden’s index, the sensitivity, specificity, positive and negative predictive values (95% CI) for unfavourable outcomes were 86% (49-99), 77% (57–90), 55% (28–79) and 94% (74–100) respectively with a diagnostic odds ratio of 20.4 (1.9–244; p=0.0055). ROC analyses of all other growth analyses (A–C) and time points showing significantly higher values in the samples from individuals with unfavourable outcomes gave AUCs less than 0.8 and lower discriminatory values.
Although this study benefitted from well-documented treatment outcomes, the numbers analysed were modest and fully powered studies will be required to validate the wider applicability of our observations. Other limitations include our use of stored samples, which raises the possibility that freezing may have differentially affected the bacillary populations enumerated (e.g. CFUs). Although we have previously demonstrated that freezing decontaminated sputum samples with addition of 10% glycerol does not significantly alter this balance,^11^ we cannot exclude a differential effect in the samples processed after the length of storage applied here. Finally, given the labour intensive and time-consuming assays applied, development of more amenable assay methods will be needed before assessment of DCMtb can be applied in the management of individual patients or in clinical trials.
Overall, we conclude that determining the Mtb resuscitation indices in stored sputum samples taken 4 weeks into treatment of pulmonary TB has promise as a means of detecting unsatisfactory outcomes, but fully powered studies are needed to validate this approach.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mitchison DA. The diagnosis and therapy of tuberculosis during the past 100 years. Am J Respir Crit Care Med 2005;171:699-706.15709048 10.1164/rccm.200411-1603 OE · doi ↗ · pubmed ↗
- 2Fox W. Whither short-course chemotherapy. British Journal of Diseases of the Chest 1981;75:331-357.7030377 10.1016/0007-0971(81)90022-x · doi ↗ · pubmed ↗
- 3Dartois VA and Rubin EJ. Anti-tuberculosis treatment strategies and drug development: challenges and priorities. Nature Rev Microbiol 2022;20:685-701.35478222 10.1038/s 41579-022-00731-y PMC 9045034 · doi ↗ · pubmed ↗
- 4Zhang Y, Yew WW, Barer MR. Targeting persisters for tuberculosis control. Antimicrobial agents and chemotherapy 2012;56:2223-2230.22391538 10.1128/AAC.06288-11PMC 3346619 · doi ↗ · pubmed ↗
- 5Garton NJ, Cytological and transcript analyses reveal fat and lazy persister-like bacilli in tuberculous sputum. P Lo S Med 2008;5:e 75.18384229 10.1371/journal.pmed.0050075 PMC 2276522 · doi ↗ · pubmed ↗
- 6Tarekegn BG, Host and pathogen factors that influence variability of Mycobacterium tuberculosis lipid body content in sputum from patients with tuberculosis: an observational study. Lancet Microbe. 2024;5(9):100885.38906163 10.1016/S 2666-5247(24)00108-3 · doi ↗ · pubmed ↗
- 7Sloan DJ, Pharmacodynamic Modeling of Bacillary Elimination Rates and Detection of Bacterial Lipid Bodies in Sputum to Predict and Understand Outcomes in Treatment of Pulmonary Tuberculosis. Clin Infect Dis 2015;61:1-8.25778753 10.1093/cid/civ 195PMC 4463005 · doi ↗ · pubmed ↗
- 8Mukamolova GV, Resuscitation-promoting factors reveal an occult population of tubercle Bacilli in Sputum. Am J Respir Crit Care Med 2010;181:174-180.19875686 10.1164/rccm.200905-0661 OCPMC 2809243 · doi ↗ · pubmed ↗