Extensive Arteriovenous Fistula Thrombosis With Glucagon-Like Peptide-1 Agonist
Muhammad Muneeb, Elizabeth Choi, Coralys Rodriguez, Kanika Goyal, Zainab Bhura, Ghadeer Hannoudi

TL;DR
A woman developed rare blood clots in her arm after increasing her dose of a GLP-1 receptor agonist, a drug known for heart and kidney benefits.
Contribution
This case report highlights a rare thrombotic complication linked to GLP-1 receptor agonists, adding to limited existing literature on this topic.
Findings
A 55-year-old patient developed extensive thrombosis in her AV fistula and surrounding vessels after increasing GLP-1 agonist dosage.
No inherited or acquired hypercoagulable states were found, suggesting a direct drug-related cause.
Discontinuation of the GLP-1 agonist prevented further thrombotic events during follow-up.
Abstract
Glucagon-like peptide-1 (GLP-1) receptor agonists are widely used due to their significant anti-atherosclerotic, cardiovascular, and renoprotective benefits. However, potential adverse effects must also be considered. Here, we present a rare case of GLP-1 receptor agonist-induced thrombotic complications in a middle-aged African American female, contributing to the limited existing literature on this topic. A 55-year-old African American female with a past medical history of deceased donor renal transplantation presented with pain, swelling, and erythema localized to the left arteriovenous (AV) fistula. She also reported fever, chills, and the absence of a palpable thrill over the fistula for approximately one week before presentation. On physical examination, she exhibited significant swelling of the left upper limb with no detectable thrill over the AV fistula. Venous and arterial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
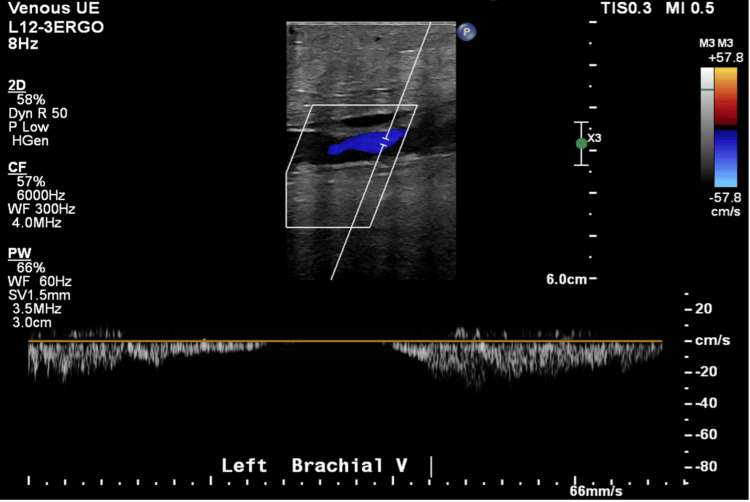 Figure 1
Figure 1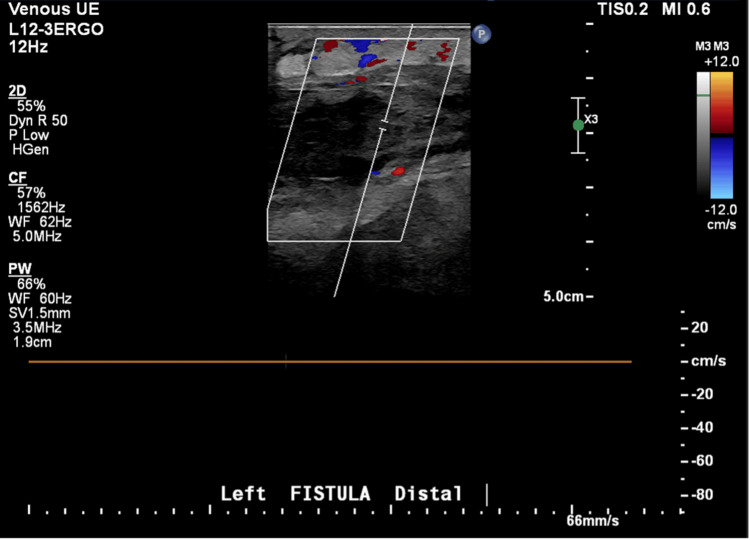 Figure 2
Figure 2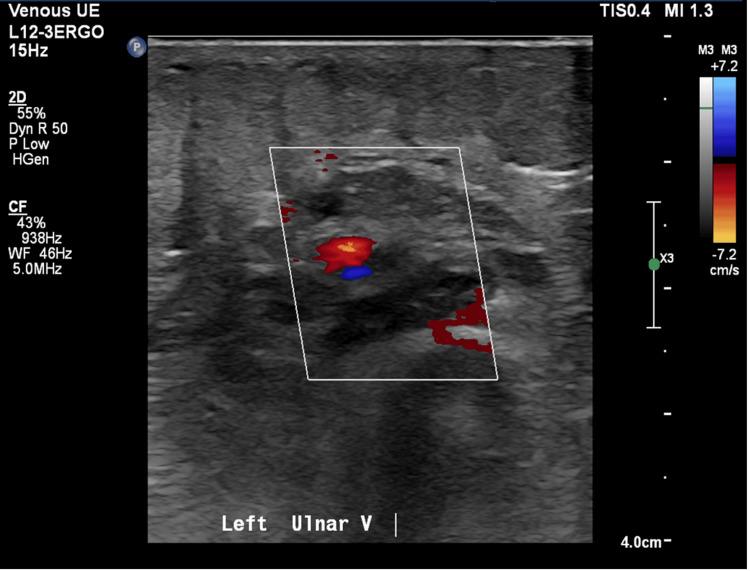 Figure 3
Figure 3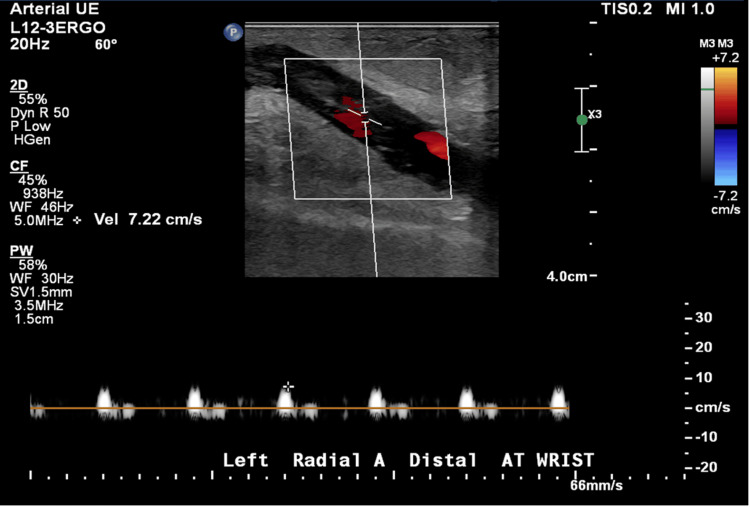 Figure 4
Figure 4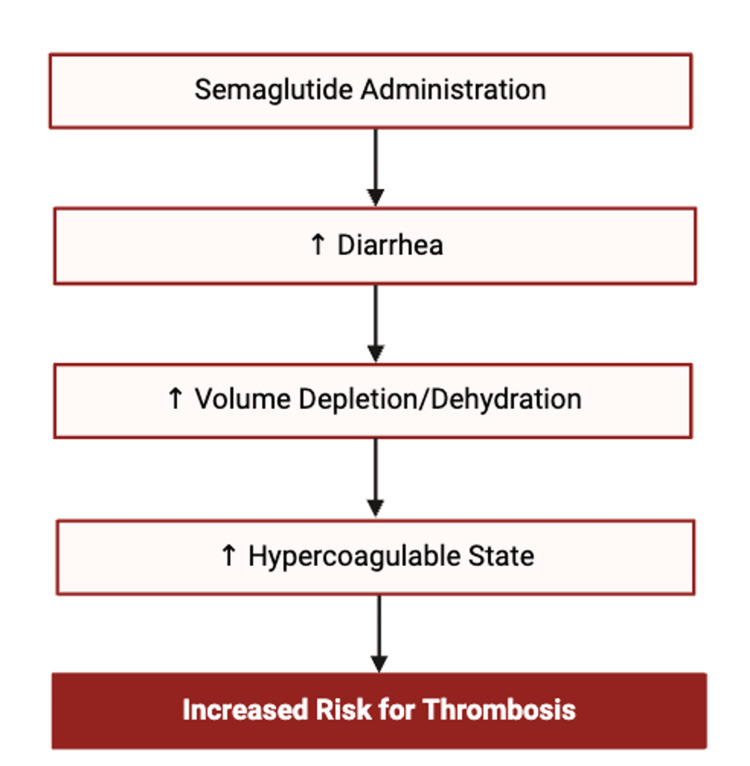 Figure 5
Figure 5| Laboratory test (unit) | Day of admission | Admission day 3 | Day of discharge | Normal values |
| White blood cell count (K/µL) | 13.3 | 10.4 | 11.6 | 3.7–11.0 |
| Red blood cell count (K/µL) | 3.86 | 3.08 | 3.11 | 3.8–5.2 |
| Hemoglobin (g/dL) | 11 | 8.7 | 8.7 | 12.0–16.0 |
| Hematocrit (%) | 34.5 | 27.4 | 27.7 | 35.0–46.0 |
| Mean corpuscular volume (fL) | 89.4 | 89 | 89.1 | 80.0–99.0 |
| Mean corpuscular hemoglobin concentration (g/dL) | 31.9 | 31.8 | 31.4 | 29.0–37.5 |
| Red cell distribution width (%) | 13.4 | 13.3 | 13.5 | 12.0–15.0 |
| Platelets (K/µL) | 433 | 420 | 470 | 150–450 |
| Prothrombin time (seconds) | 16.1 | - | - | 9.4–12.5 |
| International normalized ratio | 1.4 | - | - | <4.5 |
| Partial thromboplastin time (seconds) | 29.1 | - | - | 25.1–36.5 |
| Laboratory test (unit) | Results | Normal values |
| Beta-2 glycoprotein 1 IgA antibody (U/mL) | 1.9 | <7.0 |
| Beta-2 glycoprotein 1 IgG antibody (U/mL) | 0.8 <2.4 | <7.0 |
| Beta-2 glycoprotein IgM antibody (U/mL) | 65 | <7.0 |
| Protein S activity (%) | 124 | 65–140% |
| Protein C activity (%) | 2.2 | 70–135% |
| Cardiolipin IgA antibody | 0.6 | <14.0 |
| Cardiolipin IgG antibody, cardiolipin IgM antibody | 2.6 | <10.0 |
| Factor V Leiden | Negative | <10.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Diabetes Treatment and Management · Vascular anomalies and interventions
Introduction
Arteriovenous (AV) fistula thrombosis is one of the most common complications in patients undergoing long-term hemodialysis [1-3]. The development of such thromboses is attributed to the following factors: impaired venous outflow, inadequate arterial inflow, or predisposing conditions such as a hypercoagulable state or atherosclerotic cardiovascular disease [2]. Identified risk factors for AV fistula thrombosis include older age, female sex, elevated C-reactive protein (CRP) levels, and distal access sites [3]. In general, other conditions that increase the risk of thrombosis include the use of certain medications (e.g., immunosuppressive therapy), prolonged immobilization or hospitalization, malignancy, pregnancy, and diabetes mellitus [4-6].
Here, we describe a case involving a 55-year-old African American female with a history of deceased donor renal transplantation who presented with a six-day history of pain, swelling, and erythema over her left AV fistula, accompanied by loss of thrill. Duplex ultrasonography revealed extensive thrombosis within the AV fistula, with extension into the left radial artery and evidence of deep vein thrombosis (DVT) in the left brachiocephalic vein. No abscess formation was identified. While her medical history and comorbidities may have contributed to a prothrombotic state, the recent dose escalation from 0.5 mg to 2 mg of semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, was considered a significant contributing factor to the thrombotic event.
Case presentation
A 55-year-old African American female presented to the hospital with a one-week history of pain, swelling, and erythema localized to the AV fistula in her left arm. These symptoms were preceded by three to four episodes of diarrhea per day for a week, for which she had been hospitalized and treated with bowel rest and intravenous fluids.
Her past medical history was significant for end-stage renal disease secondary to hypertensive nephrosclerosis, for which she underwent a deceased donor renal transplant five years prior. The transplant was a four-antigen match, with alemtuzumab used for induction therapy. The patient had a functioning left upper extremity AV fistula created in 2010, which had not been in use since her transplant in 2019. Other known medical conditions include post-transplant diabetes mellitus, hypertension, and BK viremia. She had no known history of thrombosis or DVT. Her home medications included labetalol 200 mg twice daily, mycophenolate 500 mg twice daily, tacrolimus 3 mg daily, cinacalcet 30 mg daily, sodium bicarbonate 650 mg twice daily, and ferrous sulfate. She was also on semaglutide for weight loss, initiated five months prior at 0.25 mg and titrated up to 2 mg one month before presentation.
On presentation, the patient’s temperature was 101.3°F, blood pressure was 154/88 mmHg, heart rate was 124 beats per minute, and respiratory rate was 16 breaths per minute. The patient was alert, in no acute distress, nontoxic in appearance, and exhibited tachycardia with a regular rhythm. Her body mass index (BMI) was 36.67 kg/m². Local examination of the left upper extremity revealed swelling and erythema over the AV fistula, primarily in the antecubital region. The area was warm and tender on palpation, and no thrill was appreciated over the fistula.
Laboratory evaluation revealed a white blood cell count of 13.3 × 10⁹/L, hemoglobin of 10.7 g/dL, hematocrit of 34.5%, mean corpuscular volume of 89.4 fL, and platelet count of 433 × 10⁹/L. Renal function was stable with a creatinine of 1.14 mg/dL, blood urea nitrogen of 17 mg/dL, and an estimated glomerular filtration rate of 57 mL/minute/1.73 m² (Table 1). Coagulation studies revealed a prothrombin time of 16.1 seconds, an international normalized ratio of 1.4, and a partial thromboplastin time of 29.1 seconds (Table 2). Hemoglobin A1c was 6.6%.
An ECG demonstrated sinus tachycardia. Vascular duplex ultrasound of the left upper extremity revealed extensive thrombosis throughout the AV fistula with extension into the left radial artery, as well as occlusive DVT in the left brachiocephalic vein (Figures 1-4). A soft tissue ultrasound of the left upper extremity showed diffuse soft tissue edema but no discrete fluid collection to suggest abscess formation.
Left brachial vein duplex ultrasound.
Left upper extremity venous duplex ultrasound.
Left ulnar vein duplex ultrasound.
Left arterial upper extremity duplex ultrasound.
A transthoracic echocardiogram revealed a normal left ventricular cavity size and wall thickness. Systolic function was hyperdynamic, with an ejection fraction of 72%. There were no regional left ventricular wall motion abnormalities or diastolic dysfunction, and there was no evidence of a left ventricular clot. A comprehensive procoagulant workup was negative.
Initial treatment for cellulitis of the left forearm included vancomycin 750 mg every 12 hours and ceftriaxone 1 g daily for five days. Blood cultures were sterile, ruling out bacteremia. Regarding the AV fistula thrombosis, the vascular surgery team was consulted, and it was determined that there was no indication for surgical intervention. The patient was placed on intravenous heparin at a rate of 20 units/kg/hour, with ongoing thrombotic workup.
The patient’s condition was stabilized on day two of admission, and her symptoms began to improve. The patient was discharged after five days of hospitalization on oral doxycycline for 10 days and oral apixaban. The patient followed up with Nephrology one month later with stable kidney function. She was followed up by her transplant team, and semaglutide was discontinued. A full prothrombotic evaluation remained unremarkable, and a follow-up visit with her primary care physician was arranged.
Discussion
Diabetes mellitus is recognized as a substantial public health concern both in the United States and worldwide, with an estimated diabetic population of 643 million worldwide in 2030, and around 30-40% of diabetics experiencing renal disease [7,8]. Increasing need and interest in diabetic medications may reveal other potential modulators of thrombotic disease in patients with kidney disease.
GLP-1 receptor agonists, such as semaglutide, have gained widespread use in the management of type 2 diabetes due to their glycemic control, weight reduction, and cardioprotective benefits. Between January 2021 and December 2023, semaglutide prescriptions in the United States increased by 442%, from 471,876 to over 2.5 million fills, with a peak of nearly 2 million prescriptions in August 2023, a 392% increase from January 2021 [9]. While there may be adverse effects of semaglutide, it has shown great benefits in reducing systolic blood pressure, preventing major cardiovascular events, heart failure hospitalization, cardiovascular deaths, and stroke [10,11].
Recent case reports have documented instances of venous thromboembolism (VTE) in patients receiving GLP-1 receptor agonists for weight loss. These include portal vein thrombosis associated with semaglutide use [12], superior mesenteric vein thrombosis reported in patients after dose escalation of dulaglutide [13], and a case of DVT in a young man shortly after initiating tirzepatide therapy [14]. While these reports raise concern about a possible link between GLP-1 receptor agonists and VTE, especially in the context of weight loss treatment, they do not establish a causal relationship. Nevertheless, they provide preliminary evidence that warrants further investigation.
Interestingly, it had been previously proposed that GLP-1 agonists may play a role in reducing thrombus formation by activating endothelial nitric oxide synthase and increasing nitric oxide levels in platelets, which would decrease platelet activation and ultimately help prevent thrombosis [15]. Cameron-Vendrig et al. (2016) demonstrated that in vitro incubation of human megakaryocyte cells with GLP-1 agonist exenatide impaired thrombin, ADP, and collagen-mediated platelet aggregation [16].
However, emerging evidence complicates the narrative. A recent meta-analysis by Yin et al. (2021) reported a 266% increased risk of DVT associated with semaglutide use compared to control groups, despite an overall reduction in serious adverse events and a neutral impact on renal outcomes. The authors hypothesized that semaglutide-associated diarrhea may lead to dehydration, hemoconcentration, and increased blood viscosity, thereby contributing to thrombus formation [17]. In our case, a similar mechanism may have been at play. The patient experienced a week of diarrhea and dehydration shortly before the thrombotic event. The mechanism has been outlined in Figure 5.
Proposed mechanism of the association between glucagon-like peptide-1 agonist and increased risk of thrombosis.[17].
With limited resources and minimal publications addressing this issue, the complexity of establishing causality in this case is evident. Temporality did correlate with the event; however, whether GLP-1 agonists attenuate platelet aggregation by altering cellular mechanisms or increase the risk of thrombus formation by inducing a dehydrated status in the context of the patient’s age, sex, and immunocompromised status, the increase in the patient’s semaglutide dose was likely one of many contributing factors that led to her extensive fistula thrombosis. This case highlights the urgent need for further investigation into the thrombotic risks associated with GLP-1 receptor agonists.
Conclusions
Despite the potential risk of thrombosis associated with semaglutide, the therapeutic benefits may outweigh this risk. However, this case highlights a possible thrombotic complication in the setting of semaglutide use, whether due to rapid weight loss or dehydration from gastrointestinal side effects. Given the increasing use of GLP-1 receptor agonists, clinicians should be mindful to communicate this uncertainty to patients before starting treatment, especially in a population that is more susceptible to volume depletion. This case contributes to the limited existing literature and underscores the need for vigilance and individualized risk assessment when prescribing these agents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1KHA-CARI Guideline: vascular access - central venous catheters, arteriovenous fistulae and arteriovenous grafts Nephrology (Carlton) Polkinghorne KR Chin GK Mac Ginley RJ 7017051820132385597710.1111/nep.12132 · doi ↗ · pubmed ↗
- 2Overview of hemodialysis access and assessment Can Fam Physician Arasu R Jegatheesan D Sivakumaran Y 5775826820223596172010.46747/cfp.6808577 PMC 9374077 · doi ↗ · pubmed ↗
- 3Risk factors for arteriovenous fistula thrombus development: a systematic review and meta-analysis Kidney Blood Press Res Zhang Y Yi J Zhang R Peng Y Dong J Sha L 6436534720223611642810.1159/000526768 · doi ↗ · pubmed ↗
- 4The risk of thromboembolic events in kidney transplant patients Kidney Int Verhave JC Tagalakis V Suissa S Madore F Hébert MJ Cardinal H 145414608520142442940810.1038/ki.2013.536 · doi ↗ · pubmed ↗
- 5Deep Venous Thrombosis Risk Factors Stat Pearls Mc Lendon K Goyal A Attia M Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 470215/29262230 · pubmed ↗
- 6Diabetes mellitus and thrombosis Thromb Res Vazzana N Ranalli P Cuccurullo C DavìG 37137712920122219718010.1016/j.thromres.2011.11.052 · doi ↗ · pubmed ↗
- 7Diabetic kidney disease: an update Med Clin North Am Gupta S Dominguez M Golestaneh L 6897051072023 https://www.medical.theclinics.com/article/S 0025-7125(23)00037-8/abstract 3725800710.1016/j.mcna.2023.03.004 · doi ↗ · pubmed ↗
- 8International Diabetes Federation. Diabetes now affects one in 10 adults worldwide 5 2025 International Diabetes Federation 2021 https://idf.org/news/diabetes-now-affects-one-in-10-adults-worldwide/