Knowledge, Attitude, and Practice Related to Contraception Use Among Childbearing Women in the Al-Ahsa Region, Saudi Arabia
Haidar N Alhassan, Mohammed AlKhamis, Mohammed N Alkhudhair

TL;DR
The study examines how well women in Saudi Arabia's Al-Ahsa region understand and use contraception, finding high awareness but lingering misconceptions about its safety.
Contribution
This study provides insights into the knowledge, attitudes, and practices of contraception use among women in a specific Saudi region, highlighting barriers to adoption.
Findings
Most women (90.3%) were aware of contraception, but only 37.5% used it.
Oral contraceptive pills and male condoms were the most recognized and used methods.
Over half of participants believed contraceptives are harmful, indicating negative perceptions.
Abstract
Introduction: Family planning is crucial to manage population growth, reduce resource pressure, and enhance the quality of life while also promoting gender equality and improving educational options. While Saudi Arabia’s birth rate has declined, it remains high compared to high-income countries. Effective contraception reduces unintended pregnancies and associated maternal health risks. The study aimed to assess the knowledge, attitudes, and practices related to contraceptive methods among childbearing women in the Al-Ahsa region, Saudi Arabia, in 2025. Methods: This descriptive cross-sectional community-based study was conducted in 2025 among childbearing women residing in the Al-Ahsa region, Saudi Arabia. A convenience sampling yielded 392 participants. The data were collected using a pretested, validated online questionnaire and analyzed by Statistical Package for Social Sciences…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
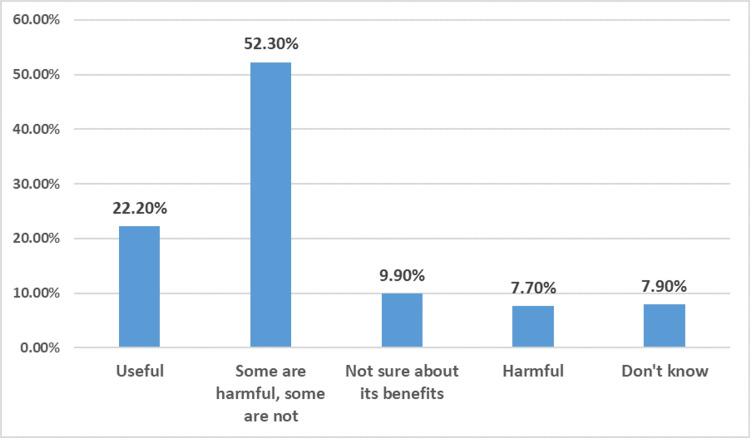 Figure 1
Figure 1| Socioeconomic characteristics | Frequency | Percentage | |
| Marital status | Single | 45 | 11.5% |
| Married | 327 | 83.4% | |
| Separated | 20 | 5.1% | |
| Age | 18-25 years | 82 | 20.9% |
| 26-35 years | 156 | 39.8% | |
| Above 35 years | 154 | 39.3% | |
| Education level | Primary school | 21 | 5.4% |
| Intermediate | 22 | 5.6% | |
| Secondary | 77 | 19.6% | |
| Diploma | 38 | 9.7% | |
| Bachelor's | 195 | 49.7% | |
| Master's or doctorate | 35 | 8.9% | |
| Illiteracy | 4 | 1.0% | |
| Job | Employed | 131 | 33.4% |
| Student | 61 | 15.6% | |
| Housewife | 178 | 45.4% | |
| Retired | 3 | 0.8% | |
| Unemployed | 19 | 4.8% | |
| Monthly income | <5,000 SAR | 225 | 57.4% |
| 5,000-10,000 SAR | 72 | 18.4% | |
| 11,000-15,000 SAR | 35 | 8.9% | |
| >15,000 SAR | 60 | 15.3% | |
| How long have you been married? | <1 year | 10 | 2.6% |
| 1-2 years | 30 | 7.7% | |
| 3-5 years | 56 | 14.3% | |
| >5 years | 241 | 61.5% | |
| Not married | 55 | 14.0% | |
| Number of children | No children | 77 | 19.6% |
| One child | 70 | 17.9% | |
| Two to four children | 184 | 46.9% | |
| Five or more children | 61 | 15.6% | |
| Previous history of abortion | Yes | 135 | 34.4% |
| No | 257 | 65.6% | |
| Knowledge regarding contraception | Frequency | Percentage | |
| Have you ever heard of contraception? | Yes | 354 | 90.3% |
| No | 38 | 9.7% | |
| According to your knowledge, what does contraception mean? | Method of family planning | 197 | 50.3% |
| Method to prevent unwanted pregnancy | 177 | 45.2% | |
| Could protect against sexual disease | 32 | 8.2% | |
| All of the above | 103 | 26.3% | |
| Do not know | 33 | 8.4% | |
| What type of contraception do you know of? | Male condom | 277 | 70.7% |
| Oral contraceptive pills | 325 | 82.9% | |
| Emergency contraception pill | 154 | 39.3% | |
| Intrauterine device | 238 | 60.7% | |
| Contraceptive implant | 230 | 58.7% | |
| Contraceptive patch | 166 | 42.3% | |
| Sterilization (vasectomy or fallopian ligation) | 131 | 33.4% | |
| Contraceptive injection | 132 | 33.7% | |
| Cervical cap | 61 | 15.6% | |
| Contraceptive ring | 89 | 22.7% | |
| Female condom | 93 | 23.7% | |
| Spermicides | 56 | 14.3% | |
| Do not know | 34 | 8.7% | |
| Do you need more education regarding family planning? | Yes | 159 | 40.6% |
| No | 233 | 59.4% | |
| Variables | Frequency | Percentage | |
| Do you prefer spacing births, meaning leaving a certain time interval between the two times you have children? | Yes | 365 | 93.1% |
| No | 27 | 6.9% | |
| What is your favorite time period? | <1 year | 9 | 2.3% |
| 1-2 years | 61 | 15.6% | |
| 3-4 years | 220 | 56.1% | |
| >4 years | 75 | 19.1% | |
| Do you use contraception? | Yes | 147 | 37.5% |
| No | 245 | 62.5% | |
| What is the reason for your use of contraception? | Prevent unplanned pregnancy | 131 | 33.4% |
| Regulate menstrual cycle | 8 | 2.0% | |
| Prevent pregnancy due to health problems | 5 | 1.3% | |
| Other | 12 | 3.1% | |
| The type of contraception used† | OCPs | 49 | 12.5% |
| Male condom | 50 | 12.8% | |
| IUD | 13 | 3.3% | |
| Natural family planning | 38 | 9.7% | |
| Contraceptive implant | 11 | 2.8% | |
| Cervical cap | 1 | 0.3% | |
| Withdrawal method | 10 | 2.6% | |
| Have you ever gotten pregnant while using contraception? | Yes | 28 | 7.1% |
| No | 364 | 92.9% | |
| What method of contraception did you use? | Natural method | 9 | 2.3% |
| Contraceptive pills | 11 | 2.8% | |
| Withdrawal method | 9 | 2.3% | |
| Male condom | 6 | 1.5% | |
| Contraceptive implant | 2 | 0.5% | |
| Did you experience any side effects while using birth control? | Yes | 52 | 13.3% |
| No | 340 | 86.7% | |
| What side effects did you experience? | Bleeding | 17 | 4.3% |
| Frequent nausea and vomiting | 12 | 3.1% | |
| Breast pain | 10 | 2.6% | |
| Mood changes | 23 | 5.9% | |
| Weight gain | 22 | 5.6% | |
| Hair loss | 17 | 4.3% | |
| Chronic headaches | 14 | 3.6% | |
| Current pregnancy | 35 | 8.9% | |
| Other symptoms | 7 | 1.8% | |
| Why are you not using birth control? | Using the natural method | 39 | 9.9% |
| Fear of side effects | 28 | 7.1% | |
| Mutual agreement between the couple | 32 | 8.2% | |
| I have a desire to have children | 51 | 13.0% | |
| For medical reasons or health issues | 20 | 5.1% | |
| Breastfeeding | 13 | 3.3% | |
| No support from my husband | 5 | 1.3% | |
| Unmarried | 48 | 12.2% | |
| Variables | Do you use contraception? | p value | ||
| Yes | No | |||
| Age categories | 18-25 years | 22 (26.8%) | 60 (73.2%) | 0.020* |
| 26-35 years | 70 (44.9%) | 86 (55.1%) | ||
| More than 35 years | 55 (35.7%) | 99 (64.3%) | ||
| Marital status | Single | 1 (2.2%) | 44 (97.8%) | <0.001* |
| Married | 145 (44.3%) | 182 (55.7%) | ||
| Separated | 1 (5.0%) | 19 (95.0%) | ||
| Education level | Primary school | 6 (28.6%) | 15 (71.4%) | 0.302 |
| Intermediate | 4 (18.2%) | 18 (81.8%) | ||
| Secondary | 31 (40.3%) | 46 (59.7%) | ||
| Diploma | 12 (31.6%) | 26 (68.4%) | ||
| Bachelor's | 75 (38.5%) | 120 (61.5%) | ||
| Master's or doctorate | 17 (48.6%) | 18 (51.4%) | ||
| Illiteracy | 2 (50.0%) | 2 (50.0%) | ||
| Occupation | Employed | 53 (40.5%) | 78 (59.5%) | 0.427 |
| Student | 21 (34.4%) | 40 (65.6%) | ||
| Housewife | 64 (36.0%) | 114 (64.0%) | ||
| Retired | 0 (0.0%) | 3 (100.0%) | ||
| Unemployed | 9 (47.4%) | 10 (52.6%) | ||
| Monthly income | <5,000 SAR | 81 (36.0%) | 144 (64.0%) | 0.405 |
| 5,000-10,000 SAR | 27 (37.5%) | 45 (62.5%) | ||
| 11,000-15,000 SAR | 11 (31.4%) | 24 (68.6%) | ||
| >15,000 SAR | 28 (46.7%) | 32 (53.3%) | ||
| How long have you been married? | <1 year | 2 (20.0%) | 8 (80.0%) | <0.001* |
| 1-2 years | 11 (36.7%) | 19 (63.3%) | ||
| 3-5 years | 28 (50.0%) | 28 (50.0%) | ||
| >5 years | 104 (43.2%) | 137 (56.8%) | ||
| Not married | 2 (3.6%) | 53 (96.4%) | ||
| How many times have you been pregnant? | Once | 23 (41.1%) | 33 (58.9%) | <0.001* |
| Twice | 36 (48.6%) | 38 (51.4%) | ||
| Three times | 23 (39.7%) | 35 (60.3%) | ||
| Four times | 21 (38.9%) | 33 (61.1%) | ||
| Five times or more | 40 (45.5%) | 48 (54.5%) | ||
| Not occurred | 4 (6.5%) | 58 (93.5%) | ||
| Number of children | No children | 3 (3.9%) | 74 (96.1%) | <0.001* |
| One child | 31 (44.3%) | 39 (55.7%) | ||
| 2-4 children | 83 (45.1%) | 101 (54.9%) | ||
| 5 or more children | 30 (49.2%) | 31 (50.8%) | ||
| Previous history of abortion | Yes | 56 (41.5%) | 79 (58.5%) | 0.238 |
| No | 91 (35.4%) | 166 (64.6%) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Reproductive Health and Contraception · Adolescent Sexual and Reproductive Health
Introduction
The world population in 2024 was eight billion, and it is still increasing [1-3]. Regulating fertility will help limit population growth, which will result in a decrease in the burden on resources of many developing countries; therefore, many developing countries consider limiting population growth a fundamental strategy to improve quality of life and standard of living, especially with the availability of effective contraception methods [4,5]. Even though the birth rate in the Kingdom of Saudi Arabia has decreased recently, it is still high compared with industrialized countries [5-7]. Family planning through contraceptive use plays a key role in reducing pregnancy rates [8]. Using contraceptive methods will lead to a reduction in the number of unintended pregnancies, which, in turn, reduces maternal morbidity and mortality, providing a substantial public health benefit [8,9]. There are multiple health benefits as well as health-related risks from using contraceptive methods, highlighting the importance of contraceptive counseling to support safe and effective use [8,10-13].
In 2022, the global contraceptive use was 65% for any method and 58.7% for modern methods in both married and union women [14]. Family planning has significantly increased over the past decades; the number of women who desire it increased from 900 million in 2000 to 1.1 billion in 2021 [15]. According to the United Nations, in 2023, 21% of women aged 15-49 in the Kingdom of Saudi Arabia used contraceptives, regardless of the method [14].
Literature reveals varying levels of knowledge, positive attitudes, and common practices regarding contraception among women in different regions in Saudi Arabia. Despite the general high awareness of contraception, there are notable differences in detailed knowledge and factors influencing its usage [16-18].
There is limited research on contraceptive knowledge, attitudes, and practices (KAP) among childbearing women in the Al-Ahsa region, Saudi Arabia. While studies exploring contraceptive KAP have been conducted in other regions of the Kingdom, the unique sociocultural and socioeconomic characteristics of Al-Ahsa necessitate localized data collection. These localized KAP data are vital for developing effective, culturally sensitive public health strategies to improve contraceptive use and reproductive health. This study aims to fill this critical knowledge gap, providing region-specific insights that will contribute to a more comprehensive national understanding of contraceptive behavior. This, in turn, will inform evidence-based policy development and resource allocation to enhance maternal and child health outcomes throughout Saudi Arabia. Subsequently, the aim of this study is to assess the knowledge, attitudes, and practices relating to contraceptive methods among women in the Al-Ahsa region, Saudi Arabia, in 2025.
Materials and methods
Study design
A descriptive, cross-sectional, community-based study was conducted in 2025 among childbearing women in the Al-Ahsa region, Saudi Arabia. By using Open Epi version 3.0 (www.openepi.com; Bill and Melinda Gates Foundation, Atlanta, GA), the population size of Saudi women living in Al-Ahsa is about 416,844, according to the General Authority for the Statistics of the Kingdom of Saudi Arabia [19]. Assuming 50% of women knew about family planning, the minimum sample size to achieve the confidence interval level of 95% and 5% margin of error was 385. After accounting for 10% and excluding some responses, the final sample included 392 participants via convenience sampling.
Study instrument
Data were collected using a pretested, online questionnaire that had been previously used and validated in a published work in another similar study [17]. The questionnaire included questions about sociodemographic characteristics, knowledge, attitudes, and practices regarding contraceptive method usage. The study utilized the Arabic version of the questionnaire after obtaining consent from its authors. The questionnaire was designed for confidentiality and anonymity, so no personally identifiable information was collected.
Data analysis
Data were collected online and exported into an Excel sheet (Microsoft Corporation, Redmond, WA), coded, and then analyzed using the Statistical Package for Social Sciences software for Windows, version 27 (IBM Corp., Armonk, NY). Continuous variables were presented as means and standard deviations, and categorical variables were presented as frequencies and percentages. The chi-square test was used to determine the relationship between contraceptive use and sociodemographic characteristics, with a p value of ≤0.05 considered statistically significant.
Ethical statement
This study was ethically approved by the Institutional Review Board of the Al-Ahsa cluster (R441024-EP-2024). Before participation, all subjects provided electronic informed consent. This process included a comprehensive explanation of the study's objectives, as well as an explicit assurance of their right to withdraw from the study at any point without consequence. Consent was obtained electronically to document their agreement to submit their responses.
Results
In a total of 392 responses, the majority of women were married (83.4%), with a mean age of 33.52 (±8.94) years, and the largest age group was between 26 and 35 years (39.8%). Nearly half of the participants (49.7%) held a bachelor's degree, and 33.4% were employed, while 45.4% were housewives. More than half (57.4%) of participants reported a monthly income of less than 5,000 SAR. More than half of the participants had been married for over five years (61.5%). Regarding fertility, 46.9% had two to four children, while 34.4% reported a previous history of abortion (Table 1).
The majority of women (90.3%) had heard of contraception. When asked about its meaning, 50.3% identified it as a method of family planning, 45.2% as a method to prevent unwanted pregnancy, and 8.2% believed it protects against sexually transmitted diseases. Regarding awareness of contraceptive methods, oral contraceptive pills (OCPs; 82.9%) and male condoms (70.7%) were the most recognized, followed by intrauterine devices (IUDs; 60.7%) and contraceptive implants (58.7%). Less commonly known methods included cervical caps (15.6%), contraceptive rings (22.7%), and spermicides (14.3%). Despite this, 40.6% of participants expressed a need for more education on family planning (Table 2).
Regarding attitude toward contraception usage, the majority (52.3%) believed that "some contraceptives are harmful while others are not," reflecting a mixed perception of safety. A smaller percent (22.2%) viewed contraception as useful, while 9.9% were unsure about its benefits. Additionally, 7.7% considered contraceptive methods harmful, and 7.9% reported that they did not know (Figure 1).
Attitude of responders regarding contraception usage (n = 392)
The vast majority (93.1%) of women reported preferring to space births, indicating a strong inclination toward allowing time intervals between pregnancies, while only 6.9% did not prefer spacing. Regarding the preferred time between births, the majority (56.1%) favored a three-to-four-year interval, followed by 19.1% who preferred more than four years and 15.6% who preferred one to two years (Table 3).
Regarding the practices of contraception use, more than one-third of responders (37.5%) reported using contraception, with the most common reason being prevention of unplanned pregnancy (33.4%). OCPs and male condoms were the most used methods (12.5% and 12.8%, respectively), followed by natural family planning (9.7%) and IUDs (3.3%). In addition, a small proportion of responders (7.1%) reported pregnancy while using contraception, most commonly with natural methods or withdrawal. Among contraception users, 13.3% experienced side effects. The most reported were mood changes (5.9%), weight gain (5.6%), and bleeding (4.3%). Despite this, 86.7% did not report any side effects (Table 3).
Regarding reasons for nonuse, 62.5% were not using contraception. The primary reasons included desire for children (13%), being unmarried (12.2%), using natural methods (9.9%), mutual agreement with the partner (8.2%), and fear of side effects (7.1%). Less commonly cited reasons included health issues, breastfeeding, or lack of partner support (Table 3).
The chi-square analysis reveals there were significant associations with age, marital status, duration of marriage, times of previous pregnancy history, and number of children. Specifically, women aged 26-35, those married for three to five years, multigravida, and those who have multiple children are more likely to use contraception. Conversely, education level, occupation, monthly income, and previous history of abortion had no statistically significant association with contraception usage (Table 4).
Discussion
Childbirth is the primary cause of mortality among women of reproductive age, with one in seven women in this demographic dying because of complications related to childbirth [20]. In our study, 90% of women know what contraception means, 50% understand that it serves as a method of family planning, 45% recognize it to prevent unwanted pregnancies, and 8% identify it as a method for protection against sexually transmitted diseases. A recent study conducted in Abha, KSA, indicated that 80.6% of their participants were aware of family planning, and among them, 68.1% were able to define family planning accurately [21].
Regarding family planning methods, OCPs were recognized by 82.9% of the population as the most familiar method, followed by male condoms at 70.7%, IUDs at 60.7%, and contraceptive implants at 58.7%, while other methods were mentioned by only a few participants. These findings are similar to a recent study in the Makkah region, which showed that women of childbearing age recognized OCPs, IUDs, and male condoms the most, with rates of 97%, 92%, and 88%, respectively. Additionally, another study conducted among Saudi men showed that OCP, condoms, and the withdrawal method were the most recognized methods [22]. Furthermore, regarding permanent contraception such as sterilization (vasectomy or fallopian ligation), our participants showed fair knowledge, with one-third (33.4%) indicating that they are aware of it. This percentage was higher than another Saudi study that indicated that a few women were aware of fallopian ligation (15.6%) and male sterilization (11.2%) [23].
This study revealed that approximately one-third of women (37%) use contraception (either traditional or modern methods). Similarly, Saudi studies conducted in the Abha, Makkah, and Al-Qassim regions revealed that 29%, 37%, and 45% of their women used contraception, respectively [7,17,21]. Inconsistently, this rate of contraception usage was lower than the findings from various studies conducted in different areas, such as Asser-KSA (75%), Syria (47%), and Egypt (60%) [24,25]. The reduced rate of contraception usage in this study may be attributed to the selection criteria, which include women with different education levels and age groups, as well as unmarried women.
The current study revealed that the male condom was the major method used by 12.8%, followed by OCPs and natural family planning methods by 12.5% and 9.7%, respectively. Conversely, other methods like IUDs, contraceptive implants, and cervical caps had lower usage rates. This may be due to inadequate promotion by medical professionals, restricted access, and patient discomfort with invasive procedures for limited usage of these methods. A study from Singapore mentioned that male condoms were the most widely known and practiced method among their population, followed by OCPs, which is consistent with our study [26]. Inconsistently, a systematic review study revealed that OCPs were the most common contraception used in Saudi Arabia, followed by IUD [27]. Unlike previous Saudi studies, the permanent methods, such as vasectomy or fallopian ligation, were not used among our population [7]. This variation may be attributed to the participants' traditions and Islamic culture, which accept only temporary delays in pregnancy while rejecting permanent sterilization. This result contrasts with global findings, whereas female sterilization was one of the most commonly utilized modern methods among married women [28].
The present study revealed that more than one-fifth of our population (22%) thought that contraception is useful, 52% considered some forms to be harmful, and 9.9% were not sure about its benefits, while 7.7% perceived it as harmful. Studies from the Makkah Region and Al-Medina City revealed that more than half of their participants agreed that some contraceptives are beneficial and some are not, which is consistent with our study [17,29]. Inconsistently, a study from Indonesia indicated that 79.12% of their participants concurred that the utilization of contraception is beneficial [30]. These findings demonstrate different degrees of trust and awareness, indicating the need for more effective education and communication about the safety and effectiveness of contraceptive choices.
Furthermore, the vast majority of the participants (93%) preferred spacing births, whereas the favorite time interval was three to four years for more than half of the participants (56%). These results are inconsistent with previous Saudi studies in Al-Qassim center and Dammam city that showed the preferred interval period was two to three years, while a study in Hail mentioned that the favorite interval was two to four years [7,31].
This study revealed that the vast majority of women who used contraception used it to decrease unwanted pregnancies. Instances of unwanted pregnancies influence breastfeeding practices [32]. Literature examining abortion as a method of fertility control has indicated that women primarily turn to abortion when family planning services are lacking or inadequate [33]. Lower rates of abortion and pregnancy contribute to decreased maternal mortality by minimizing the frequency of risk exposure, as well as decreasing stillbirths and improving child mortality rates.
Regarding barriers to using birth control methods, the primary reason cited was the desire to have children, accounting for 13%. This was followed by being currently unmarried in 12.2%, currently pregnant in 8.9%, mutual agreement between partners in 8%, fear of side effects in 7%, and medical reasons in 5%, while 9.9% of women believed that employing natural methods was beneficial for them. A study conducted in Sierra Leone mentioned that the primary reason for not using contraception was unwillingness to disclose at 52.6%, followed by a wish for a child at 19.2%, apprehension regarding side effects at 15.7%, being currently pregnant at 8.7%, and being against religious beliefs at 3.5% [34]. A study in Al-Qassim center, KSA, revealed that the children's blessing was the major reason for contraceptive refusal in 69.5%, followed by fear of health problems (19%) and fear of affecting marital life (11%) [7]. Another study conducted in Cameroon revealed that the main reasons for not using contraception included insufficient information (31.4%), perceived uselessness (31.4%), and concerns regarding side effects (14.3%) [35].
The current study demonstrated a significant association between age and contraception-using rate, whereas mothers aged 26-35 years and those aged more than 35 years had the highest rate. Al Sheeha mentioned that the contraception use rate was higher in groups over 30 years old, with a strong, significant association [7]. Inconsistently, a study in the Makkah region mentioned that the highest contraception use was presented among the 18-25 age group with an insignificant association [17]. Older mothers attributed their feeling that they have enough children and want to be more concerned with their study and work, unlike younger ones.
Moreover, the present study revealed that there was a significant correlation between the number of children and the contraception usage rate, in which the rate was increasing as the number of children increased. Combined with this rate, 40% of our population stated that they need more information regarding contraception. This indicates the need for areas for improvement in public awareness and reproductive health education in Al-Ahsa Governorate.
Strengths and limitations of the study
This study provides good insights about contraceptive KAP among women in the Al-Ahsa region of Saudi Arabia, supported by a reasonable sample size of 392. However, the cross-sectional design limits causal inferences, and the convenience sampling may introduce selection bias, hindering generalizability. Reliance on self-reported data and an online questionnaire raises concerns about recall bias, social desirability bias, and potential exclusion of women with limited internet access.
Conclusions
This study demonstrates a good level of awareness regarding contraception; a notable finding was the persistence of negative perceptions about its safety among more than half of the participants. Despite these concerns, over a third of the respondents reported using contraception, primarily to prevent unplanned pregnancies, with OCPs and male condoms being the most popular methods. The study further concludes that contraceptive use is significantly associated with specific demographic factors, including being in the 26-35 age group, having been married for three to five years, and having experienced multiple pregnancies or having several children. To address these findings, the study strongly recommends targeted public health campaigns designed to directly counter myths and misconceptions about contraception, thereby promoting a more positive and accurate understanding of its benefits and safety. Furthermore, it suggests focusing educational efforts on specific demographic groups, such as younger married women and those who are considering or actively expanding their families, to provide tailored information on various contraceptive options suitable for different life stages. These recommendations aim to bridge the gap between awareness and positive attitudes, ultimately leading to improved contraceptive practices.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Knowledge, attitude, practice and preferences of contraceptive methods in Udupi District, Karnataka J Family Reprod Health Sherpa SZ Sheilini M Nayak A 11512072013 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4064783/24971113 PMC 4064783 · pubmed ↗
- 2Contraceptive methods and factors associated with modern contraceptive in use. [Online ahead of print]J Fam Reprod Health Qazi HA Hashmi A Raza SA Soomro JA Ghauri A 2010 https://jfrh.tums.ac.ir/index.php/jfrh/article/view/88/88
- 3Knowledge, attitude and practices regarding contraceptive pill and its side effects among women in Jazan Region, Saudi Arabia Clin Pract Alameer MI Muqri KY Awlaqi AA 2682751220223564530910.3390/clinpract 12030032 PMC 9149825 · doi ↗ · pubmed ↗
- 4Knowledge, Attitude and Practices Regarding Contraceptive Pill and Its Side Effects Among Women in Jazan Region, Saudi Arabia Almualm M Khamis Y Pulau Pinang, Malaysia University of Science Malaysia 2007 http://eprints.usm.my/9109/1/KNOWLEDGE,_ATTITUDE_AND_PRACTICE_OF_HUSBANDS_TOWARDS_MODERN_FAMILY_PLANNING_IN_MUKALLA,_YEMEN.pdf
- 5Universal health coverage - there is more to it than meets the eye J Family Med Prim Care Faizi N Kazmi S 169170620172902677710.4103/jfmpc.jfmpc_13_17PMC 5629889 · doi ↗ · pubmed ↗
- 6Saudi Arabia demographics profile 6 2025 2021 https://www.indexmundi.com/saudi_arabia/demographics_profile.html.
- 7Awareness and use of contraceptives among Saudi women attending primary care centers in Al-Qassim, Saudi Arabia Int J Health Sci (Qassim) Al Sheeha M 112142010 https://pmc.ncbi.nlm.nih.gov/articles/PMC 3068803/21475521 PMC 3068803 · pubmed ↗
- 8Contraception 6 2025 n.d.https://www.who.int/health-topics/contraception