Torsion of an Accessory Spleen Presenting as Acute Right Iliac Fossa Pain: A Case Report
Jamal Ouachaou, Aicha Driouich, Mohammed Sidayne, Fatimazahrae El Khettab, Zarrouki Youssef

TL;DR
A rare case of a young woman experiencing sudden abdominal pain due to a twisted accessory spleen is reported, emphasizing the challenges in diagnosis and the role of laparoscopy.
Contribution
This paper presents a rare clinical case of accessory spleen torsion diagnosed laparoscopically and reviews its medical management.
Findings
Accessory spleen torsion is a rare and challenging cause of acute abdominal pain.
Laparoscopy proved crucial for both diagnosing and treating the condition preoperatively.
Medical literature on managing this condition is limited and requires further exploration.
Abstract
Accessory spleens are typically identified incidentally. Torsion of an accessory spleen, however, is an exceptionally rare cause of acute abdominal pain and presents a significant diagnostic challenge due to its non-specific clinical presentation. We report the unusual case of a young woman admitted to the emergency department for an acute abdomen, leading to the laparoscopic diagnosis of accessory spleen torsion. This case highlights the diagnostic difficulties encountered preoperatively and underscores the pivotal role of laparoscopy in both the diagnosis and treatment of this rare condition. A review of the literature on medical management is also included.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
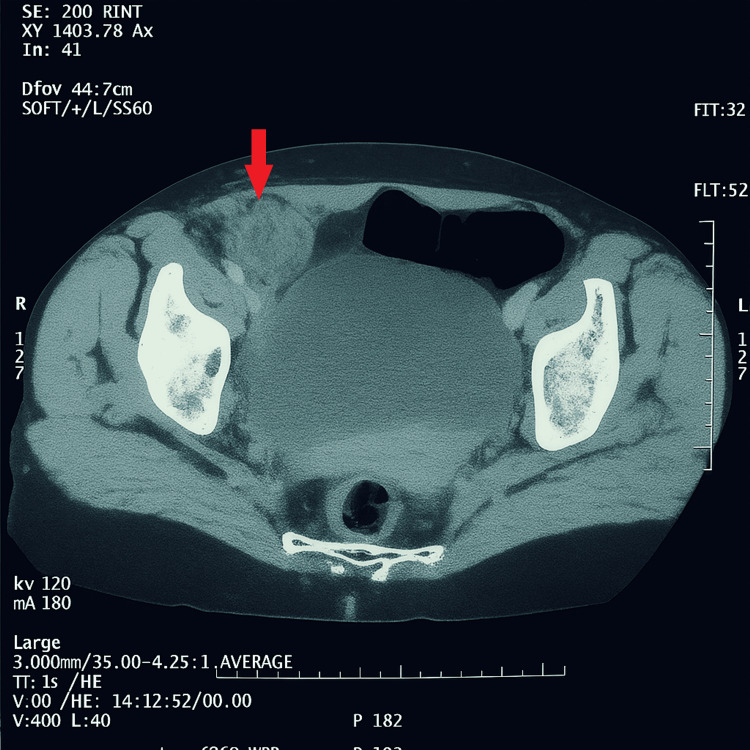 Figure 1
Figure 1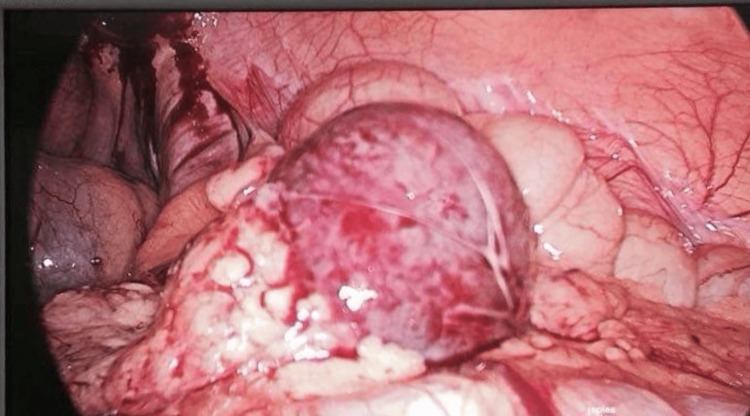 Figure 2
Figure 2 Figure 3
Figure 3| Test | Result (SI units) | Normal range (SI units) |
| Hemoglobin g/dl | 10.50 | 8.4-11.2 |
| Hematocrit % | 0.43 | 0.40-0.54 |
| White blood cells /µL | 6900 | 4000-10000 |
| Platelets cells/µL | 350000 | 150,000-400,000 |
| Urea (mg/L) | 0,42 | 0.25-0.48 |
| Creatinine µmol/L | 80,3 | 60-110 |
| Sodium mmol/L | 142 | 135-145 |
| Potassium mmol/L | 4.2 | 3.5-5.0 |
| Prothrombin ratio % | 90 | 70-100 |
| C-reactive protein (CRP) (mg/L) | 11 | <2 |
| Human chorionic gonadotropin (HCG) (mIU/mL) | 2 | <5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Trauma Management and Diagnosis · Appendicitis Diagnosis and Management
Introduction
An accessory spleen is a congenital anatomic abnormality characterized by ectopic splenic tissue that does not fuse with the main splenic mass [1]. It is a common condition that has been noted in 10% of abdominal CT scans [2]. However, torsion of an accessory spleen is an extremely rare cause of acute abdominal pain. Only a few cases have been reported in the medical literature [3]. Its clinical presentation is non-specific, and in most cases, the diagnosis is made during surgery, even with the use of computed tomography [4]. Herein, we describe the rare case of a young patient admitted to the emergency department for an acute abdomen caused by torsion of an accessory spleen.
Case presentation
A healthy 28-year-old woman, with no medical history, presented with acute right iliac fossa pain evolving over the past three days, described as sharp and persistent, and associated with nausea and vomiting. There is no urinary complaint and no menstrual delay; her last period was 10 days ago. On examination, she was mildly distressed and preferred to lie still. Abdominal palpation revealed tenderness in the right iliac fossa with guarding and rebound tenderness; Rovsing’s sign was positive. Vital signs showed a temperature of 38.1°C, heart rate of 94 bpm, blood pressure of 120/76 mmHg, respiratory rate of 18 breaths per minute, and oxygen saturation of 98% on room air. A pregnancy test, complete blood count (CBC), C-reactive protein (CRP), urinalysis, and abdominal-pelvic ultrasound were requested. Acute appendicitis was the leading diagnosis, with ovarian torsion and ruptured cyst considered in the differential. Laboratory analysis showed a white blood cell count of 6900 cells/µL, a low level of serum CRP (11 mg/L), and a normal HCG level (2 IU/L) (Table 1).
Ultrasonography (US) revealed a minimal hypoechoic effusion in the right iliac fossa. The spleen was normally located. An abdominal CT scan showed a heterogeneous mass in the right iliac fossa, which slightly enhanced (Figure 1).
CT scan of the pelvic region showing a right laterocystic mass with a wall slightly enhanced by the contrast product (red arrow).
Based on the radiological findings, laparoscopic surgery was performed, revealing a 3 cm twisted mass on its pedicle (Figure 2), which was resected after clipping the pedicle (Figure 3).
Laparoscopic view of the mass.
Necrotic accessory spleen
Anatomopathological examination confirmed the diagnosis of an accessory spleen torsion. The postoperative course was uneventful. The patient got discharged four days after.
Discussion
Accessory splenic torsion is a rare and often under-recognized cause of acute abdominal pain. Due to its non-specific clinical, biological, and radiological presentations, as well as its rarity, the diagnosis is most often made intraoperatively [5,6] .Patients generally arrive with acute or subacute abdominal pain, which is usually focused in the left upper quadrant, left flank, or even the lower abdomen, depending on where the accessory spleen is situated, nausea, vomiting, and low-grade fever.
In most cases, accessory spleens are clinically silent and can be discovered incidentally on abdominal imaging requested in the context of other pathologies. Complications are very rare and may include torsion, infarction, bleeding, and infection [7,8,9,10].
The spleen develops from mesenchymal tissue in the dorsal mesogastrium during the fifth week of gestation. Accessory spleens likely originate from mesenchymal remnants that fail to fuse with the main splenic mass. The most common site for accessory spleens is the splenic hilum, but other locations include the splenic vessels, omentum, and retroperitoneum [7,11,12].
US findings can vary, with the accessory spleen presenting as a hypoechoic or homogeneous parenchymal mass located in any quadrant of the abdomen. On enhanced CT scan, twisted accessory spleens typically appear as well-marginated, rounded masses that enhance heterogeneously depending on blood flow in the twisted pedicle. MRI has advantages over US and CT, not only for detecting the mass but also for evaluating its nature. However, MRI is not always feasible in emergency situations [7,10]. In this case, the CT scan was crucial in identifying an abdominal mass but could not definitively diagnose the etiology, reinforcing the challenge of preoperative diagnosis. The location in the right iliac fossa is also unusual, further complicating the clinical picture.
Nonetheless, preoperative diagnosis is often hypothetical. Laparoscopy with histological examination remains the gold standard for both diagnosis and treatment [10,13,14]. Laparotomy is usually reserved for complicated cases (e.g., peritonitis or abundant hemoperitoneum) or when a large accessory spleen cannot be extracted via laparoscopic surgery.
In this case, laparoscopy was the first-line intervention, providing both diagnosis and treatment. This situation differs from the torsion of a wandering spleen, where the diagnosis is more obvious due to the absence of the splenic compartment on radiological examination [11].
The surgical removal of an accessory spleen does not result in the immune deficiency seen in splenectomized patients with a single spleen, so postoperative vaccination is not indicated.
Conclusions
While accessory spleens are common, torsion of an accessory spleen is a rare cause of acute abdominal pain in the emergency room. It is helpful for radiologists to be aware of the possibility of accessory spleen torsion so that the diagnosis can be suggested early, especially when an avascular mass is seen on the CT scan, and the normal spleen remains in place.
The definitive diagnosis is obtained in the operating room after anatomopathological examination.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Differential diagnosis of splenic lesions EPOS Pozuelo Segura C Pozuelo O Mones L 2010
- 2The accessory spleen : prevalence and imaging findings in 1,735 consecutive patients examined by multidetector computed tomography J Belg Soc Radiol Romer T Wiesner W 616595201222764656 · pubmed ↗
- 3Torsion of an accessory spleen: case report and review of the literature Radiol Case Rep Sadro CT Lehnert BE 802820132733061810.2484/rcr.v 8i 1.802PMC 4900206 · doi ↗ · pubmed ↗
- 4Identification of accessory spleens during laparoscopic splenectomy is superior to preoperative computed tomography for detection of accessory spleens JSLS Koshenkov VP Pahuja AK Németh ZH Abkin A Carter MS 3873911620122331806310.4293/108680812 X 13427982377102 PMC 3535795 · doi ↗ · pubmed ↗
- 5Infarction of an accessory spleen causing an acute abdomen Am J Surg Badcok TL Coker DD Haynes JL Conklin HB 3363371271974481224210.1016/0002-9610(74)90044-0 · doi ↗ · pubmed ↗
- 6Lesions observed in accessory spleens of 311 patients Am J Clin Pathol HAB GYF 1651683219591367014010.1093/ajcp/32.2.165 · doi ↗ · pubmed ↗
- 7Paratesticular accessory spleen Mayo Clin Proc Wick MR Rife CC 455456561981 https://pubmed.ncbi.nlm.nih.gov/7253706/7253706 · pubmed ↗
- 8Abscess of an accessory spleen Am Surg Habib FA Kolachalam RB Swason K 215218662000 https://pubmed.ncbi.nlm.nih.gov/10695757/10695757 · pubmed ↗