A Rare Twist in the Tale: Midgut Volvulus From Intestinal Non-rotation in an Adult
Ram Kumar, Alexander Mecheri Antony, Ganesh Guru, V Ramlakshmi, Gowthaam Ramesh

TL;DR
This paper discusses a rare case of intestinal malrotation in an adult causing midgut volvulus and highlights the importance of early diagnosis and surgical intervention.
Contribution
The paper emphasizes the need for increased awareness of intestinal malrotation in adults to improve timely diagnosis and treatment.
Findings
Intestinal malrotation can present in adulthood with symptoms like abdominal pain and vomiting.
Imaging techniques like contrast-enhanced upper gastrointestinal series and CT scans are crucial for diagnosis.
Prompt surgical intervention is necessary to prevent complications like bowel ischemia and short bowel syndrome.
Abstract
Intestinal malrotation is an inherited condition where the midgut is not properly rotated, and it tends to be noticed in infancy. It becomes evident in later life with unusual abdominal pain and vomiting, which happen due to occasional blockages. Consequently, there is a risk of midgut volvulus and damage to the blood supply of the bowel. For diagnosis, the best method is imaging, especially using a contrast-enhanced upper gastrointestinal series that reveals characteristic signs such as a corkscrew shape and a misplaced duodenojejunal junction. Using ultrasonography and computed tomography (CT) scans, visualization of an unusual relationship between the superior mesenteric vessel and whirlpool sign, as well as abnormal location of the jejunal artery, can be confirmed. Most surgeons use the elective Ladd's procedure for the surgery. When bowel ischemia is found, surgery must be done,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
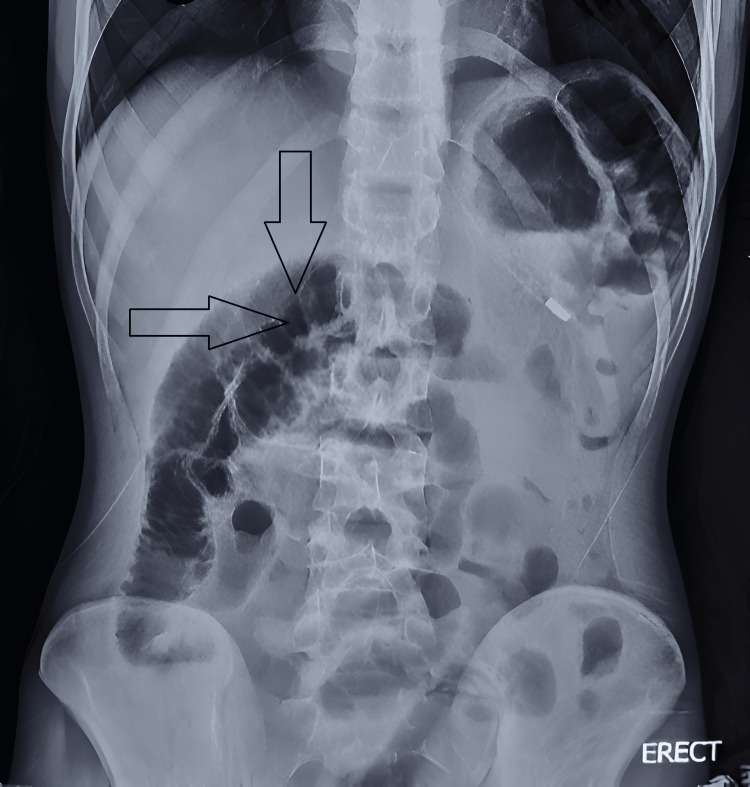 Figure 1
Figure 1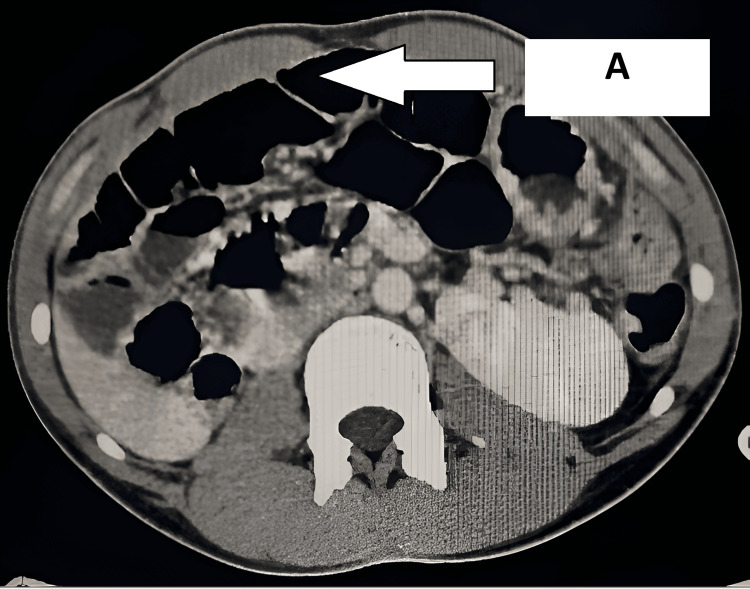 Figure 2
Figure 2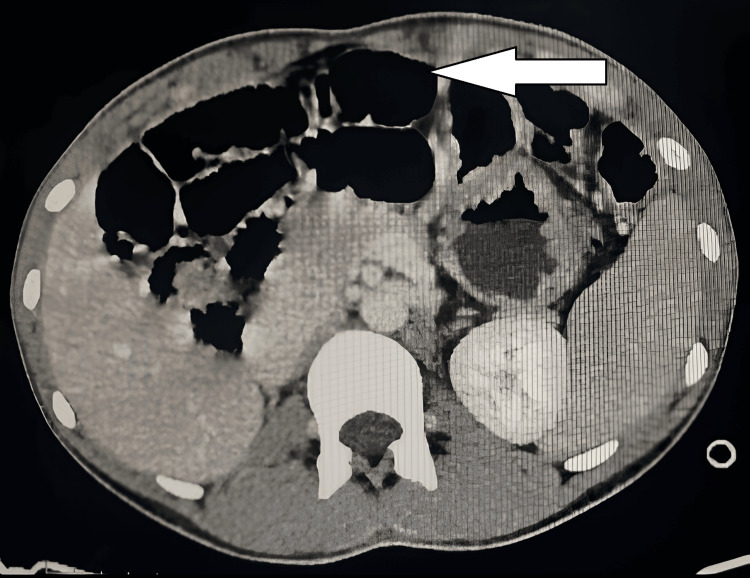 Figure 3
Figure 3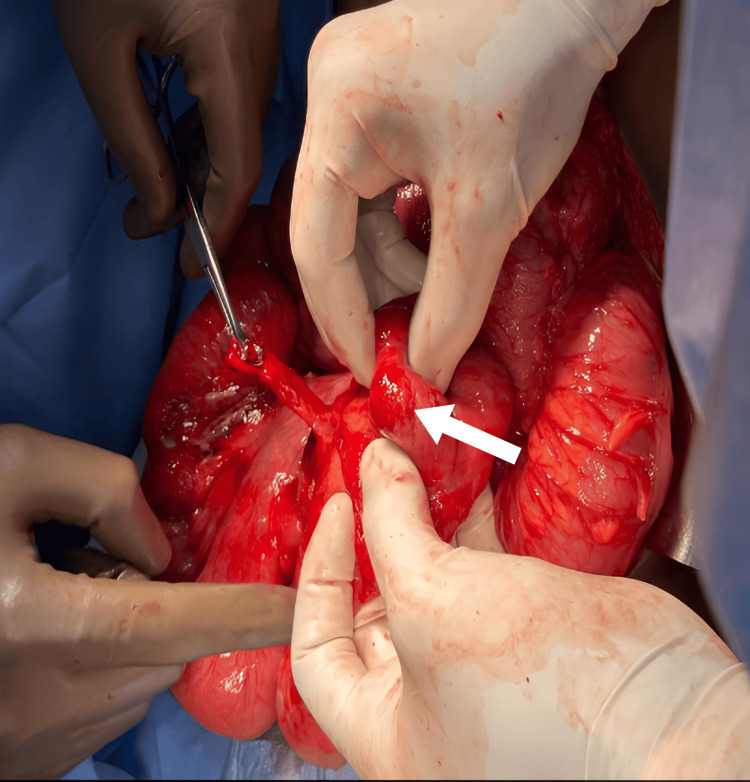 Figure 4
Figure 4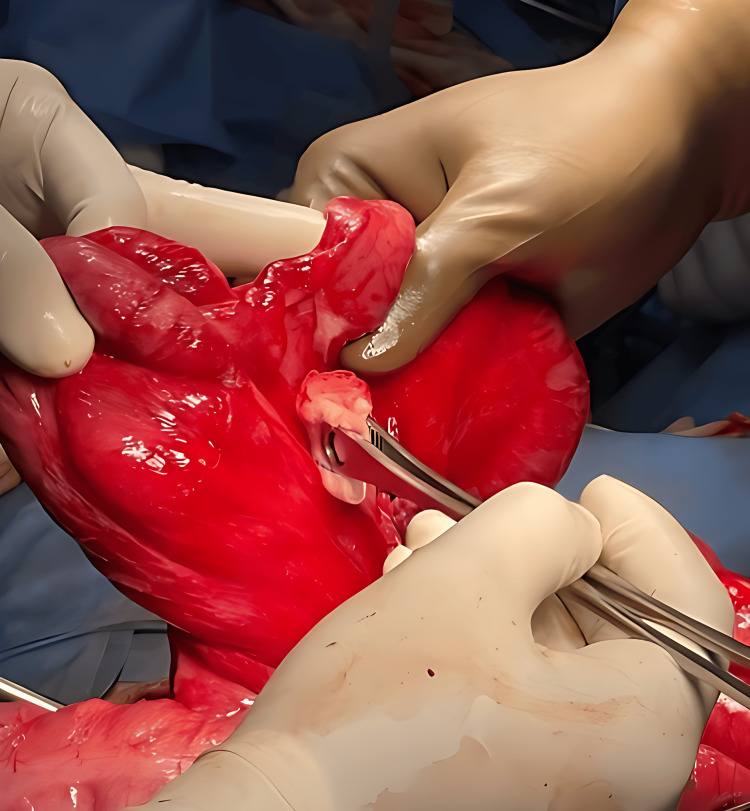 Figure 5
Figure 5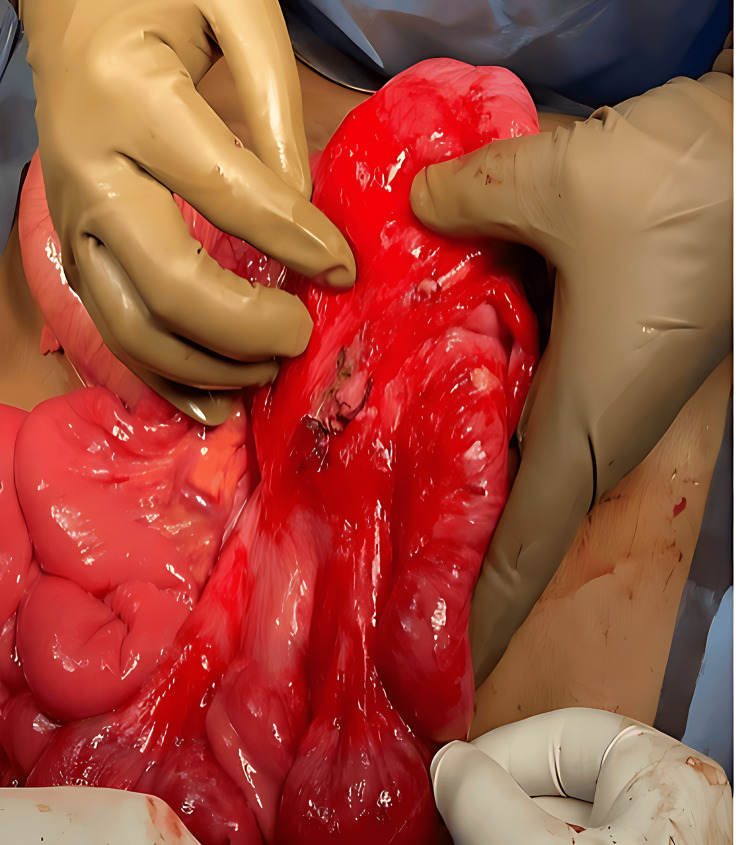 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Esophageal and GI Pathology · Pediatric Hepatobiliary Diseases and Treatments
Introduction
Intestinal malrotation represents a spectrum of congenital conditions resulting from the failure of the midgut to complete its physiological rotation and subsequent fixation within the abdominal cavity. The absence or partial completion of a 270-degree counterclockwise rotation around the superior mesenteric vessels leads to an abnormal spatial relationship between the intestinal segments [1]. In patients with intestinal malrotation, the typical anatomical landmark of the ligament of Treitz is absent due to the aberrant positioning of the bowel. Consequently, the distal duodenum and jejunum are characteristically situated on the right side of the vertebral column, deviating from their normal left-sided location [2]. The pathophysiology of intestinal malrotation, characterized by an incomplete midgut rotation and a resultant narrow mesenteric attachment, predisposes individuals to midgut volvulus. This twisting of the bowel can lead to vascular compromise, intestinal obstruction, and ultimately, tissue necrosis. Although the clinical presentation is most common in the neonatal period, with most cases diagnosed within the first month of life, a smaller subset of patients (0.2%-0.5%) are identified in adulthood [3]. The occurrence of intestinal malrotation does not exhibit a significant gender predilection, with similar rates observed in both male and female populations [4]. In adults, intestinal malrotation commonly presents with a clinical picture of intermittent, crampy abdominal pain accompanied by bile-containing vomitus. It represents the predominant predisposing factor for midgut volvulus in this age group, and subsequent obstructive complications are often localized to the colon [5].
Case presentation
An 18-year-old male patient presented to the emergency department with a four-day history of acute, insidious onset, colicky lower abdominal pain radiating to the back, related to three episodes of non-projectile, non-bilious, non-blood-stained vomiting comprising food particles. He reported intermittent abdominal pain for the past year and a history of low-grade fever relieved by medication two days prior, along with one episode of loose stools and loss of appetite for four days. His past surgical history was observed to be significant for circumcision. Family history revealed a maternal history of a left ectopic kidney. On examination, the patient was oriented, conscious, and afebrile. Abdominal examination indicated diffuse tenderness, distension, guarding, and rigidity. Bowel sounds were exaggerated in the right lower quadrant. Digital rectal examination was unremarkable. X-ray of the abdomen showed multiple dilated bowel loops (Figure 1).
Erect abdominal X-ray showing multiple dilated bowel loopsArrows indicate multiple dilated bowel loops.
Contrast-enhanced computed tomography (CECT) of the abdomen demonstrated the cecum and ileocecal junction in the pelvis, reversed superior mesenteric artery (SMA) and vein axis with twisting of mesenteric vessels, and small bowel loops in the right lumbar region ("whirlpool sign"), absent retromesenteric course of the D3 segment of the duodenum, and a duodenojejunal flexure on the right side. It also confirmed a right ectopic kidney cross-fused with the left kidney (Figures 2, 3).
CECT of the abdomen (axial view)A: CECT of the abdomen showing a dilated bowel loop.CECT: contrast-enhanced computed tomography
CECT of the abdomen (axial view)The arrow indicates the dilated bowel loop.CECT: contrast-enhanced computed tomography
Based on the radiological findings of intestinal malrotation with midgut volvulus, the patient underwent emergency exploratory laparotomy. Intraoperatively, non-rotation of the midgut with volvulus and the cecum in the left pelvis was noted. A small mesenteric fold adhered to the retroperitoneum near the duodenojejunal flexure was identified. Congestion was observed in the terminal ileum, ileocecal junction, ascending colon, and cecum. The appendix appeared inflamed, and bilaterally fused kidneys were found near the midline, with an empty right renal fossa. The volvulus was untwisted, with the colon positioned in the left lateral gutter and the small bowel in the right lateral gutter (Figures 4-6).
Intraoperative imageThe arrow points to the cecum.
Intraoperative image
Intraoperative image
The postoperative period was uneventful, and the patient was discharged on postoperative day 7.
Discussion
Intestinal malrotation is most frequently identified during the initial month of life. However, it is crucial to recognize that the diagnosis can also be made in adults, indicating the potential for delayed presentation [2]. Given the frequently obscure clinical manifestations of intestinal malrotation in adults, the predominant symptoms reported by patients are vomiting and recurrent abdominal pain, likely arising from an underlying pattern of chronic intermittent bowel obstruction [6,7]. A subset of adult patients with intestinal malrotation may exhibit malabsorption secondary to both reduced oral intake and protein-losing enteropathy stemming from chronic or intermittent volvulus-induced diarrhea [1].
The diagnostic workup for suspected intestinal malrotation often involves several imaging modalities, including plain radiography, ultrasonography, and computed tomography. Nevertheless, contrast-enhanced studies of the stomach and duodenum have been shown to provide the most precise and dependable diagnostic information [8]. The "corkscrew sign," observed on imaging, is a hallmark of intestinal malrotation, arising from the uneven distension of various parts of the duodenum. Additionally, the abnormal location of the duodenojejunal junction, secondary to jejunal folding, represents another key radiological feature [9]. The superior mesenteric vein (SMV) being located in front of the SMA on ultrasound is one of the main signs of intestinal malrotation. Doppler ultrasound can show the whirlpool sign, which proves that the SMV is rotating around the SMA, a sign of pathology [10]. One of the ways computed tomography (CT) imaging is helpful is by locating the jejunal arteries on the right side of the superior mesenteric artery, which is not normal [11]. Considering that intestinal blockage due to malrotation is very common, most people with this condition are advised to have an elective laparotomy right away. Elective surgery for intestinal malrotation has usually been done using Ladd's procedure since 1936 [12]. The standard Ladd's procedure for elective intestinal malrotation entails detorsion of any midgut volvulus, division of obstructive peritoneal bands, non-rotation positioning of colon and small bowel, and prophylactic appendectomy. However, if there is bowel ischemia, removing the affected parts is crucial; therefore, Ladd's procedure cannot be used. Sometimes, resection of a large part of the small bowel can result in short bowel syndrome. Alternative treatments, including cecopexy, endoscopic reduction, and laparoscopic techniques, have been documented. Laparoscopic Ladd's procedure has shown promise for elective cases, potentially offering benefits over the traditional open approach [13]. However, surgical management of intestinal malrotation should be tailored to the individual patient.
This case highlights several key considerations regarding this infrequent condition. The clinical presentation of adult malrotation can be subtle, although the "whirlpool sign" on abdominal CT may suggest bowel torsion. Acute presentations, however, often involve extensive bowel necrosis, potentially requiring significant resection. The subsequent management of short bowel syndrome, a potential consequence of massive small bowel resection, is complex and frequently complicated by electrolyte abnormalities, malnutrition, immunodeficiency, organ failure, and sepsis. Refeeding enteroclysis can be a valuable tool among these patients, provided there is adequate residual healthy distal small bowel for nutrients, bile salt, and fluid absorption [14].
Conclusions
Given the variable clinical presentation of intestinal malrotation, ranging from asymptomatic to vaguely symptomatic, this condition should be a key consideration in differential diagnosis of acute abdomen and intestinal ischemia. Accurate diagnosis, relying on the combination of history, physical examination, and imaging, is paramount to facilitate prompt surgical intervention aimed at limiting patient morbidity and mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adult intestinal malrotation presenting as midgut volvulus; case report J Surg Arts Sahu SK Raghuvanshi S Sinha A Sachan PK 182152012 https://www.researchgate.net/publication/277041285_ADULT_INTESTINAL_MALROTATION_PRESENTING_AS_MIDGUT_VOLVULUS_CASE_REPORT_Barsak_malrotasyonuna_bagli_olarak_gelisen_incebarsak_volvulusu_Olgu_sunumu
- 2Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review World J Emerg Surg Emanuwa OF Ayantunde AA Davies TW 2262011 https://doi.org/10.1186/1749-7922-6-222180141710.1186/1749-7922-6-22PMC 3158108 · doi ↗ · pubmed ↗
- 3Intestinal malrotation discovered at the time of laparoscopic Roux-en-Y gastric bypass J Gastrointest Surg Palepu RP Harmon CM Goldberg SP Clements RH 8989021120071748753710.1007/s 11605-006-0035-5 · doi ↗ · pubmed ↗
- 4Defusing the intra-abdominal ticking bomb: intestinal malrotation in children CMAJ Kamal IM 131513171622000 https://pubmed.ncbi.nlm.nih.gov/10813015/10813015 PMC 1232416 · pubmed ↗
- 5Midgut volvulus: a rare cause of acute abdomen in an adult patient AJR Am J Roentgenol Bernstein SM Russ PD 6396411711998 https://doi.org/10.2214/ajr.171.3.9725289972528910.2214/ajr.171.3.9725289 · doi ↗ · pubmed ↗
- 6Midgut malrotation with chronic abdominal pain N Am J Med Sci Wanjari AK Deshmukh AJ Tayde PS Lonkar Y 19619842012 https://doi.org/10.4103/1947-2714.949502253656510.4103/1947-2714.94950 PMC 3334262 · doi ↗ · pubmed ↗
- 7Intestinal volvulus: aetiology, morbidity, and mortality in Nigerian children Pediatr Surg Int Ameh EA Nmadu PT 5052162000 https://doi.org/10.1007/s 0038300500131066383510.1007/s 003830050013 · doi ↗ · pubmed ↗
- 8Midgut volvulus: value of multidetector computed tomography in diagnosis Turk J Gastroenterol Duran C Oztürk E Uraz S Kocakuşak A Mutlu H Killi R 189192192008 https://pubmed.ncbi.nlm.nih.gov/19115156/19115156 · pubmed ↗