Osteomyelitis Complicating Sickle Cell Disease
Furgan Özcan, Filip Vanhoenacker, Frederick Catry

TL;DR
This paper highlights the difficulty in distinguishing between two bone conditions in sickle cell disease patients and emphasizes the need for careful imaging and clinical evaluation.
Contribution
The paper emphasizes the importance of integrating imaging and clinical data for accurate diagnosis in sickle cell disease patients.
Findings
Diaphyseal osteomyelitis and bone infarction are hard to differentiate in sickle cell disease.
Accurate diagnosis requires careful correlation of imaging and clinical findings.
Abstract
Teaching point: Differentiating diaphyseal osteomyelitis and bone infarction in patients with sickle cell disease is challenging and requires meticulous correlation of imaging and clinical findings.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
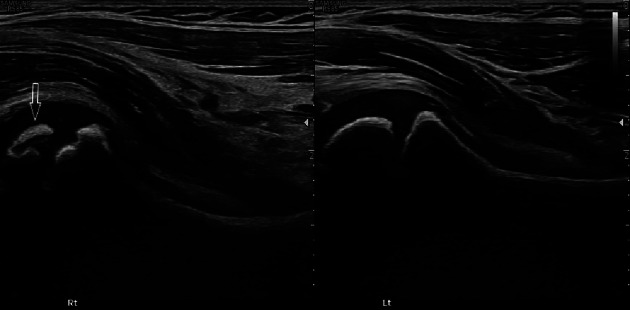 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Hemoglobinopathies and Related Disorders · Tuberculosis Research and Epidemiology
Case History
A 3‑year‑old child of African descent presented with high fever, limping, and refusal to bear weight. There was no history of trauma.
Abdominal ultrasound was unremarkable.
Ultrasound of the hips demonstrated irregular delineation of the right proximal femoral epiphysis and adjacent growth plate (Figure 1, arrow).
Ultrasound. Irregular delineation of the right proximal femur (arrow).
Conventional radiography (CR) of the pelvis showed flattening, heterogeneous sclerosis of the right femoral head, and widening of the femoral neck (Figure 2), in keeping with Legg–Calvé–Perthes disease.
Conventional radiography. Flattening, sclerosis of femoral head; widening of femoral neck.
Laboratory examination revealed leukocytosis with a left shift, anemia, and elevated CRP (116 mg/L). Hemoglobin electrophoresis revealed sickle cell disease (SCD) by demonstrating an elevated HbS fraction.
Because of clinical suspicion of osteomyelitis, an MRI was performed. Fat suppressed (FS) proton density (PD) image (Figure 3A) revealed diffuse increased signal intensity in both femoral diaphysis, indicating red bone marrow hyperplasia.
A Fat‑saturated PD‑WI MRI. Increased signal in the femoral diaphyses. B–C Fat‑saturated T1‑WI MRI with contrast. Subperiosteal collection with peripheral rim enhancement (arrow).
A subtle subperiosteal collection along the right femoral diaphysis, with peripheral rim enhancement (Figure 3B‑C, arrow) was seen on contrast‑enhanced FS‑T1‑weighted images.
The diagnosis of SCD complicated by osteomyelitis was suggested, based on the combination of clinical, laboratory, and imaging findings. Blood cultures remained negative. The patient showed uneventful recovery within two weeks following the start of antibiotic therapy, supporting empirically the diagnosis of osteomyelitis.
Comments
SCD is an autosomal recessive disorder of the hemoglobin molecule in red blood cells, causing chronic hemolytic anemia and chronic hypoxemia that may result in compensatory red bone marrow hyperplasia.
The most common musculoskeletal (MSK) complications include avascular necrosis or bone infarct due to microvascular vaso‑occlusion, osteomyelitis (typically caused by Salmonella), septic arthritis, and growth retardation [1]. Legg–Calvé–Perthes disease—as in our patient—is the pediatric equivalent of avascular necrosis of the hip in adults.
Acute infarction and acute osteomyelitis of the diaphysis of the long bones may present with similar features on MRI [1], rendering the differential diagnosis difficult, particularly if pre‑existing bone marrow hyperplasia is present. Clinical presentation is often nonspecific, as bone tenderness, swelling, fever, and leukocytosis may occur in both acute infarction and acute osteomyelitis. Blood cultures do not always yield a microbiological diagnosis, further hampering a precise diagnosis.
In this case, based on the presence of a subperiosteal collection, adjacent soft tissue extension, and the rapid recovery following antibiotic therapy, the final diagnosis of osteomyelitis was made.
Osteomyelitis in SCD arises from hematogenous spread of bacteria, facilitated by impaired splenic function, vascular stasis, and bone infarction, creating a nidus for infection [1].
CR rarely contributes to the diagnosis of acute complications of SCD, and MRI is recommended in any case of suspected acute MSK complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.