Ultrasound-guided pulsed radiofrequency versus perineural platelet rich plasma injection for the treatment of idiopathic carpal tunnel syndrome: a prospective randomized controlled study
Engi Yousry Hashem, Faten Saeed Shamandy, Ahmed Fawzy Elmulla, Magdy AbdelAziz Mansour

TL;DR
This study compares ultrasound-guided treatments for carpal tunnel syndrome, finding that pulsed radiofrequency and steroids work better than platelet-rich plasma.
Contribution
A novel prospective randomized controlled trial comparing pulsed radiofrequency, steroids, and platelet-rich plasma for carpal tunnel syndrome.
Findings
PRF and steroid groups showed greater pain and function improvement than PRP.
All groups improved significantly in pain, function, and nerve measurements.
PRP had the least improvement compared to other treatments.
Abstract
Carpal tunnel syndrome (CTS) is the most common focal mononeuropathy caused by the compression of the median nerve within the carpal tunnel. Ultrasound-guided hydrodissection with corticosteroids, platelet-rich plasma injection, and median nerve pulsed radiofrequency are all potential treatments for relieving symptoms of CTS in mild and moderate cases, comparison between their clinical outcomes is yet to be studied.The primary outcome was pain measured by Visual Analog Scale (VAS). The secondary outcomes included functional outcome evaluated by the Boston Carpal Tunnel Questionnaire (BCTQ), Nerve Conduction Velocity (NCV) and median nerve cross-sectional area (CSA). This prospective, double-blinded, randomized controlled study was conducted on Seventy-five patients diagnosed with mild to moderate CTS, they were randomly allocated into three equal groups. The control group received a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
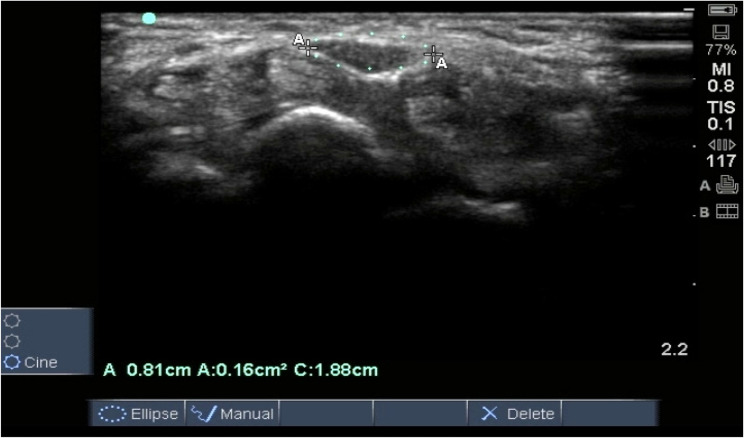 Figure 1
Figure 1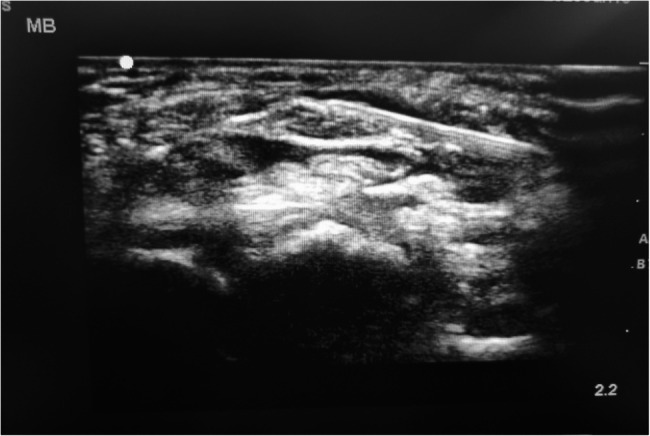 Figure 2
Figure 2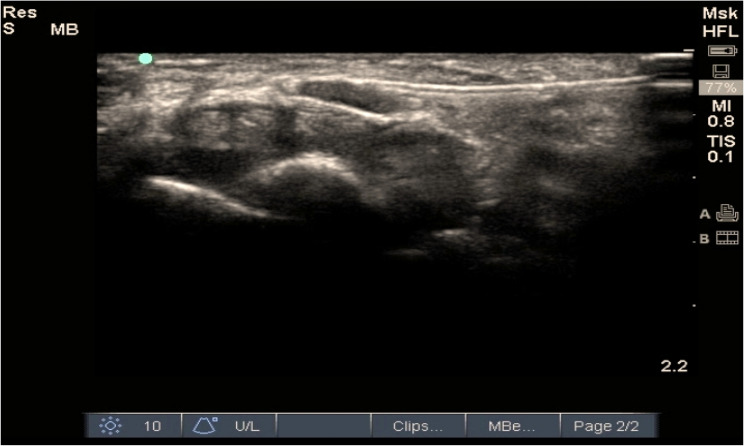 Figure 3
Figure 3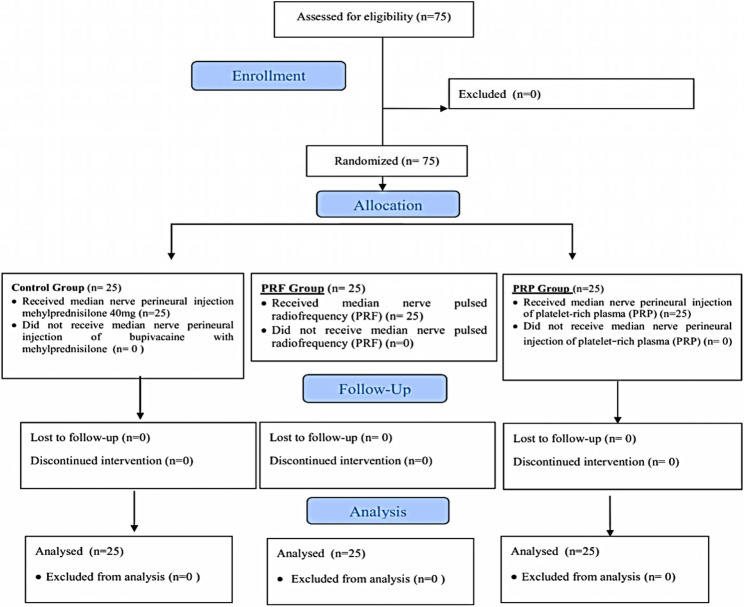 Figure 4
Figure 4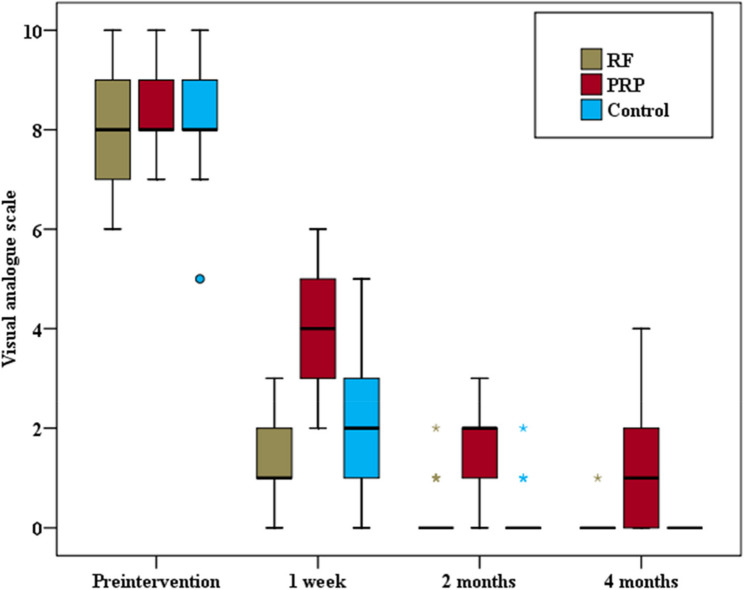 Figure 5
Figure 5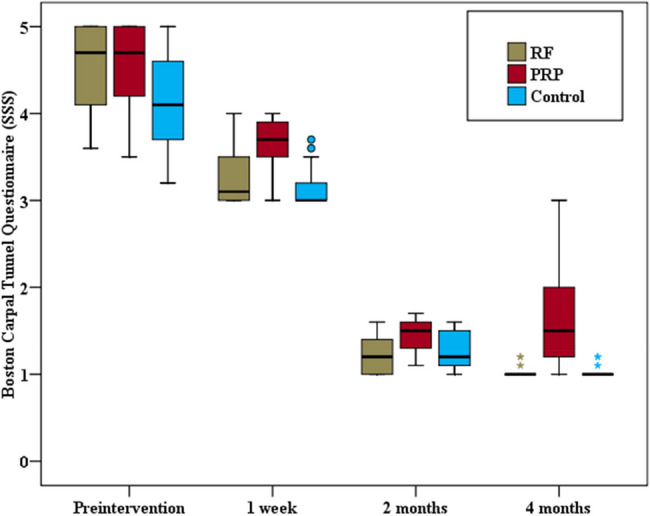 Figure 6
Figure 6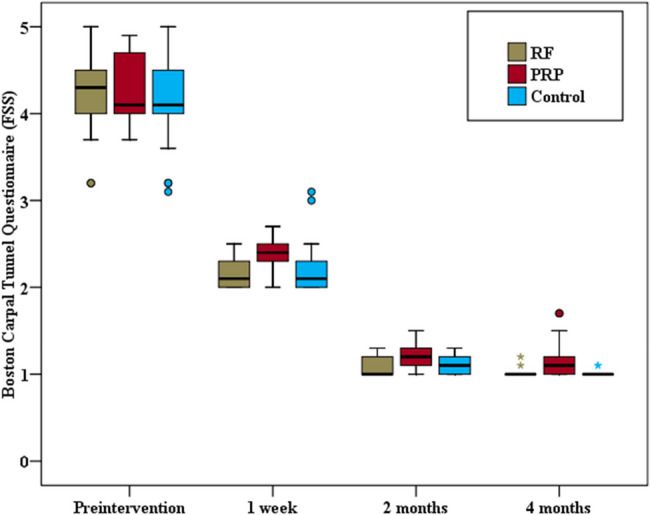 Figure 7
Figure 7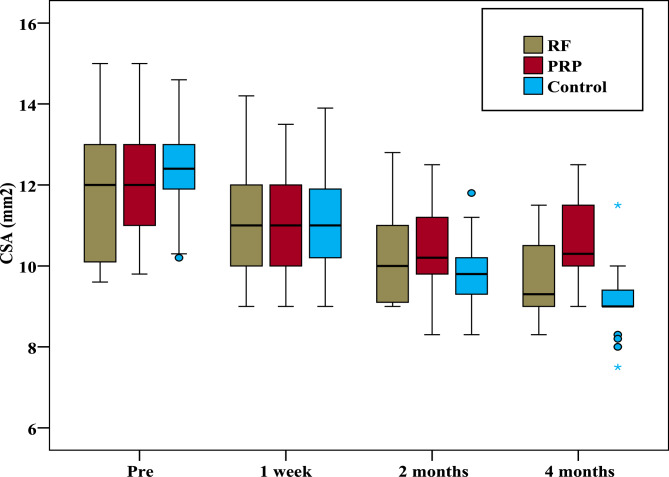 Figure 8
Figure 8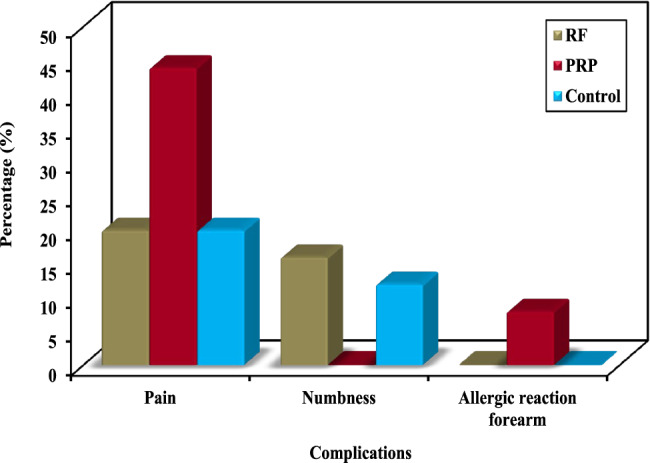 Figure 9
Figure 9- —Alexandria University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Nerve Disorders · Shoulder Injury and Treatment · Orthopedic Surgery and Rehabilitation
Introduction
Carpal tunnel syndrome (CTS) is a compression neuropathy affecting the median nerve at the wrist. The pathophysiology of CTS involves increased endoneurial pressure, reduced neuronal microcirculation, neural ischemia, edema, and fibrosis [1]. Nonsurgical treatments such as splints and physical therapy are recommended for mild-to-moderate CTS but have limited therapeutic effects [2].
Ultrasound-guided hydrodissection, corticosteroids, platelet-rich plasma (PRP) injections, and pulsed radiofrequency (PRF) treatment are all potential therapies. The precise mechanisms underlying the therapeutic benefits of such treatments remain incompletely understood. Hydrodissection can reduce gliding resistance in patients with CTS, as it creates a fluid plane around the nerve and dislodges perineural adhesions [3]. Corticosteroids alleviate inflammation by modifying vascular wall permeability [4]; nonetheless, the mechanism through which they confer analgesic benefits is likely attributable to their antifibrotic properties [5].
Platelet-rich plasma (PRP) therapies aim to increase self-healing by using autologous growth factors to stimulate wound healing, angiogenesis, and axonal regeneration [4].PRP products exhibit significant therapeutic potential as neuroprotective, neurogenic, and neuroinflammatory modulators. They are employed in the management of peripheral nerve injuries and neuropathies. Plasma rich in growth factors encompasses a diverse array of growth factors, microparticles, and bioactive mediators. Upon the infiltration of PRP, cell signaling molecules, such as neurotrophic factors—including nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), platelet-derived growth factor (PDGF), and insulin-like growth factor 1 (IGF-1)—as well as neurotropic factors (fibrin, fibronectin, and vitronectin) are released. These elements facilitate the modulation of early inflammation, the activation of stem cells, macrophage polarization, the resolution of inflammation, angiogenesis, and fibrogenesis. Consequently, they are indispensable for the functional recovery of nerve tissue(6).
Pulsed radiofrequency (PRF) treatment alleviates pain by delivering electric impulses and heat bursts at a temperature of less than 42 °C [5]. PRF selectively regulates small-diameter Aδ and C-type fibers through modifications to mitochondria, microfilaments, and microtubules within these fibers [7].PRF techniques are routinely employed for their neuromodulatory effects on resting baseline pain perception, while concurrently mitigating the risks associated with thermodestructive lesioning. Despite a limited understanding of the underlying mechanisms, the application of electrical fields has demonstrated the capacity to exert reversible effects on impulse transmission along small unmyelinated fibers. This phenomenon can induce alterations in the excitatory C and Aδ fibers, which are pivotal for the transmission of nociceptive and neuropathic pain. Several mechanisms have been postulated, including modifications at nerve synapses and alterations in nerve permeability induced by the electrical field. Furthermore, changes in c-Fos signaling pathways may augment descending noradrenergic and serotonergic inhibitory pathways [8].
The aim of the study is to evaluate the role of pulsed radiofrequency versus platelet rich plasma injection in treatment of idiopathic mild to moderate carpal tunnel syndrome.
Study registration
The study was retrospectively registered in the “Clinical Trials Library for Protocol Registration and Results System” under NCT05053477 0n September 11, 2021. This investigation strictly followed CONSORT requirements as outlined in their statement published in 2010 [9].
Methods
This double-blind, randomized controlled trial was conducted on 75 patients recruited from the pain clinic at the Medical Research Institute, Alexandria University, who were diagnosed with mild to moderate idiopathic carpal tunnel syndrome (CTS) for more than 3 months and who had not responded positively to conservative treatment methods.
After declaring the research benefits and potential side effects, a comprehensive Informed written consent form was obtained from all participants for their involvement in the study. Additionally, written informed consent was acquired from the patients for the publication of the ultrasound images from the study.
Assessment and preparation
Patients were thoroughly assessed by:
-
Detailed medical and surgical history taking.
-
Clinical examination for median nerve by Reverse Phalen’s test, Tinel’s tests and Boston Carpal Tunnel Syndrome Questionnaire (BCTQ).
-
Ultrasound examination:
-
Cross-sectional area (CSA): The median nerve was identified using a 38 mm, L25x,13 − 6 MHz, linear array transducer with a portable, bedside Ultrasound unit (Sonosite S-Nerve, Sonosite Inc.,USA). The participants’ wrists were maintained in neutral positions, scanning was done in short axis, as the probe was parallel to proximal crease of hand where the CSA was measured. The greatest lateral measurements in anteroposterior and lateral dimensions were recorded (mm^2^) and then calculated into an elliptical shape for subsequent calculation of its surface area (mm^2^)and the cross sectional area of the nerve was measured in mm2. (Fig. 1).Fig. 1CSA of median nerve measurement at level of pisiform bone
-
Any secondary causes for carpal tunnel syndrome were identified including and not restricted to (tenosynovitis. Ganglion cyst, tumor or space occupying lesions, bifid nerve median or a patent median artery, ect).
-
Nerve conduction velocity study (SNCV) were conducted by the same physiotherapist within the same laboratory for all the patients pre and post procedural.
-
Laboratory investigations via venous blood sample:
-
Complete blood picture.
-
Platelet count.
-
Random blood sugar.
-
Prothrombin activity (PT, INR).
Inclusion criteria
- Patients aged (20–60) years of both gender.
- Patients with mild to moderate idiopathic CTS The grading of CTS was based on Padua’s study as (1) Mild: abnormal, sensory nerve conduction velocity (SNCV) with a normal distal motor latency (DML), (2) Moderate: abnormal SNCV and DML, and (3) Severe: absence of SNCV and abnormal DML [10, 11].
- Patient who are failed to respond to conservative treatment (such as splint, medications, physical therapy) for at least three months.
Exclusion criteria
- Severe CTS severe CTS (distal latency to abductor pollicis brevis muscle > 6.5 ms or with absent sensory potentials of the median nerve by electrophysiological study [7], cross-sectional area [CSA] of median nerve > 15.0 mm2 by ultrasonography [12].
- Secondary CTS due to systemic disease including thyroid disease, diabetes mellitus, or acromegaly or due to local causes as identified by the pre-procedural Ultrasound including tenosynovitis. Ganglion cyst, tumor or space occupying lesions, bifid nerve median or a patent median artery.
- Other neuropathies overlapping with CTS.
- Previous release surgery for the median nerve or wrist surgery.
- Pregnancy.
- Known allergies to any of the medications or who were on concurrent steroids.
- Previous injections to CTS upto 6 months.
Patients were randomly assigned to one of the three studied groups. The allocation was performed via a computer-generated randomization program (www.randomizer.org) in which patients were equally assigned to the three studied groups.Each patient’s randomization number was concealed until the end of the study from both the patients and the outcome assessor who was blinded to the procedure used.The procedure used for treatment was not revealed to the patients until study completion.
Intervention
All the procedures were conducted under ultrasound guidance (Sonosite^®^ S-Nerve™ ultrasound machine, FUJIFILM SonoSite, USA) with a 38 mm, L25x, 13–6 MHz, linear array probe. Patients were in a supine position while their forearm was extended with the palm facing up and slightly extended with a small pillow. This position was used during the ultrasound assessment and injection.
- The control group (n = 25) received a perineural injection of bupivacaine (0.25%) with methylprednisolone (40 mg) in a total volume of 2 ml. Injection was done to circumstantially Hydro dissecting the nerve from the underlying structures and the retinaculum above. (Fig. 2).Fig. 2. Hydodisection of the median nerve using a 22-gauge needle
The PRF group (n = 25): After the identification of the median nerve using ultrasound, a 5-cm radiofrequency curved cannula with a 10-mm active tip was meticulously advanced towards the median nerve employing the in-plane technique. Utilizing the Neurotherm (NT1000 (NeuroTherm® NT2000Ix, Abbott Medical, USA),), both sensory and motor stimulations were assessed. Sensory responses were elicited at 50 Hz and upto 0.5 V, while motor responses were evaluated at 2 Hz and up to 1 V, respectively. Pulsed radiofrequency (PRF) lesions were applied for a duration of 120 s at a frequency of 2 Hz and a pulse width of 20 ms, voltage 45 v, maintained at a temperature of 42 °C. Subsequently, 2 ml of 0.25% bupivacaine was administered perineurally. (Fig. 3).Fig. 322-gauge, 50-mm radiofrequency cannula inserted above median nerve
Finally, the PRP group (n = 25) received a perineural injection of 2 ml of PRP. PRP was prepared by withdrawing 15 ml of fresh whole blood from each patient in citrate tubes. The tubes were initially centrifuged at 3000 rpm for 10 min. The resulting supernatant plasma and buffy coat were then transferred to another sterile plain tube and subjected to hard spin at 4000 rpm for 15 min. The sediment comprising 2 ml of PRP was suspended by gently shaking it, then it was injected perineurally under real-time ultrasound guidance using the inplane technique.
Post procedure care for three groups
- Patients were advised to apply ice on the injection site at day of intervention and modify activity as tolerated to alleviate any post injection discomfort or pain.
- Pain medication in the form of paracetamol (500 mg) only was allowed for the next 4 months if needed. The patients were instructed to stop analgesics 48 h before visit of follow up to allow proper symptoms assessment.
- Physical therapy, splinting, or exercise were not allowed.
Study endpoints
The primary outcome measure among the groups was the visual analog scale (VAS). The secondary outcomes included cross-sectional area (CSA), functional outcome as evaluated by the Boston Carpal Tunnel Questionnaire (BCTQ), and an electrophysiological study via nerve conduction velocity (NCV).
Measurements
Baseline measurements assessing demographic data, CSA (mm^2^), baseline pain and disability through the VAS and BCTQ [13] were obtained before the intervention, followed by subsequent assessments at one week, two months, and four months after the procedure. An Arabic version of the BCTQ was handed to the patients at each visit. NCV testing was carried out by the same physiotherapist in the same laboratory and machine configurations to validate the standardization both initially and at four months. Any complications that occurred during or after any interventions were reported and managed accordingly.
Statistical analysis
The required sample size of the study was calculated via the PASS Version 20 program. To ascertain the proportional difference in pain relief assessed by the visual analog scale (VAS) compared with the control group, a minimum hypothesized total sample size of 75 adults (25 per group) is necessary. This computation incorporates a 95% confidence interval and 80% statistical power, utilizing the chi-square test [9]. The data were analyzed via the IBM SPSS software package version 20.0 (Armonk, NY: IBM Corp). Qualitative data are expressed in terms of numbers and percentages. The normality of the distribution was confirmed by the Shapiro‒Wilk test. Quantitative data are presented as the means, standard deviations, medians, and interquartile ranges (IQRs). Statistical significance was considered at the 5% level. For categorical variables, a chi-square or Monte Carlo test was conducted to compare various groups. To compare normally distributed quantitative variables among more than two groups, an F test (ANOVA) was performed, while pairwise comparisons were performed through post hoc testing. The Kruskal‒Wallis test was used for non normally distributed quantitative variables with multiple studied groups, where pairwise comparisons took place via Dunn’s multiple comparisons test under post hoc analysis.
Results
Seventy-five patients were recruited, and none of them were excluded. The 75 patients who fulfilled the inclusion criteria were randomized into 3 equal groups of 25 patients each. The attrition rate was 0% (Fig. 4).Fig. 4CONSORT flow diagram of the studied participants
Demographic data were comparable across the three study groups, with no statistically significant differences among the three groups (Table 1).Table 1. Comparison between the three studied groups regarding the demographic dataPRF(n = 25)PRP(n = 25)Control(n = 25)pSex (females)25 (100%)25 (100%)25 (100%)–Age (years)33.36 ± 7.7834.08 ± 7.535.36 ± 8.780.674Data were expressed using Mean ± SDPRF pulsed radiofrequency, PRP platelet rich plasmaStandard deviation. P < 0.05 is considered significant
There was no statistically significant difference among the three groups prior to the intervention concerning the various clinical criteria, including VAS, CSA, both components of the BCTQ and the different parameters of the nerve conduction tests (Table 2).Table 2. Comparison between the three studied groups regarding clinical criteria before the interventionPreinterventionRFPRPControl(p)(n = 25)(n = 25)(n = 25)VAS0.762Min. – Max.6–107–105–10Median (IQR)8 (7–9)8 (8–9)8 (8–9)CSA (mm2)0.577Min. – Max.10.20–14.609.60–15.09.80–15.0Median12.41212BCTQ (SSS)0.072Min. – Max.3.60–5.03.50–5.03.20–5.0Median (IQR)4.7(4.10–5.0)4.7(4.20–5.0)4.1(3.70–4.60)BCTQ (FSS)Min. – Max.3.20–5.03.70–4.903.10–5.00.569Median(IQR)4.3(4.0–4.50)4.1(4.0–4.70)4.1(4.0–4.50)Distal motor latency (msec)Min. – Max.4.30–5.204.30–5.204.30–5.20(0.956)Median4.704.704.70Sensory conduction velocity (m/s)Min. – Max.35.10–37.8035.10–37.3035.10–38.40(0.195)Median36.4035.8036.30Distal CMAP amplitude (mV)Min. – Max.6.80–10.107.10–10.406.80–10.0(0.491)Median8.808.708.50Data were expressed using Mean ± SDPRF pulsed radiofrequency, PRP platelet rich plasmaStandard deviation. P < 0.05 is considered significant
The group analysis unveiled a significant reduction in all groups in the Visual Analog Scale (VAS) score pre and post-intervention at one week, two months, and four months.
The VAS score was significantly different among the three groups at different follow-up times: one week (p < 0.001), two months (p < 0.001), and four months (p < 0.001). Pairwise comparisons between the two groups in terms of the VAS score at different study times revealed statistically significant differences between the PRF group and the PRP group after one week (p < 0.001), after two months (p < 0.001), and after four months of intervention (p < 0.001), where lower scores were recorded in the PRF group. Additionally, there was a statistically significant difference in the VAS score at different study times between the steroid group and the PRP group after one week (p < 0.001), after two months (p < 0.001), and after four months of intervention (p < 0.001), where lower VAS scores were recorded in the steroid groups. However, there was no statistically significant difference in the VAS score at different study times between the PRF group and the control group after one week (p = 0.079), after two months, (p = 0.838), and after four months of intervention (p = 0.768) (Fig. 5).Fig. 5. Comparison between the three studied groups as regards Visual Analogue scale
The same group comparison revealed statistically significant improvements in both components of the BCTQ at all follow-up time points compared with the preintervention readings. A statistically significant difference in BCTQ (SSS) and BCTQ (FSS) scores was detected among the three groups at various follow-up times (p < 0.001). Pairwise comparisons between each group revealed significant differences in BCTQ (SSS) and BCTQ (FSS) scores between the PRF and PRP groups at all studied time points (p = 0.001). Similarly, significant differences in BCTQ (SSS) and BCTQ (FSS) scores were found between the PRP group and the steroid group at all the studied follow-up times (p < 0.001, p = 0.002, p < 0.001 for the BCTQ (SSS) and p < 0.001, p_3_ = 0.001, p < 0.001 for the BCTQ (FSS) respectively). Conversely, no statistically significant difference in BCTQ was detected between the PRF group and the control group at any of the studied times. (Figs. 6 and 7).Fig. 6. Comparison between the three study groups as regard Boston Carpal Tunnel Questionnaire (SSS)Fig. 7. Comparison between the three study groups as regard Boston Carpal Tunnel Questionnaire (FSS)
With respect to the CSA, the same group comparison revealed a statistically significant decrease in the median nerve CSA in all the groups at all the studied times compared with the preintervention values. A significant difference among all the groups was recorded only after four months (p < 0.001). Pairwise comparisons revealed no significant difference in the CSA between the PRF and steroid groups after four months (p = 0.147), but a significant difference was recorded between the steroid and PRP groups (p = 0.002) and between the PRF and PRP groups (p < 0.001) (Fig. 8).Fig. 8. Comparison between the three studied groups regarding median nerve cross sectional area (mm2)
After four months of intervention, all the groups showed significant improvements in different NCS parameters, including distal motor latency (msec), CMAP amplitude (mV), and sensory conduction velocity (SCV) (m/s). Compared with the PRP group, the steroid group and PRF group demonstrated a significantly greater improvement in all NCSs. The data regarding all the parameters and the degree of significance are presented in (Table 3)Table 3. Comparison between the three study groups regarding NCV (distal motor latency (msec), distal CMAP amplitude (mV) and sensory conduction velocity (m/s)RF(n = 25)PRP(n = 25)Control(n = 25)(p)Sig. bet. grps.Distal motor latency (msec)Before(0.956)–Min. – Max.4.30–5.204.30–5.204.30–5.20Median4.704.704.704 monthsMin. – Max.3.40–4.503.40–4.803.60–4.50(< 0.001^^)p_1_ < 0.001^^,p_2_ = 0.284,p_3_ = 0.014^^Median3.704.203.90(p_0_)(< 0.001^^)(< 0.001^^)(< 0.001^^)Distal CMAP amplitude (mV)BeforeMin. – Max.6.80–10.107.10–10.406.80–10.0(0.491)–Median8.808.708.504 monthsMin. – Max.9.20–15.508.30–14.09.10–15.20(< 0.001^^)p_1_ < 0.001^^,p_2_ = 0.624,p_3_ < 0.001^^Median13.909.8013.60(p_0_)(< 0.001^^)(< 0.001^^)(< 0.001^^)Sensory conduction velocity (m/s)BeforeMin. – Max.35.10–37.8035.10–37.3035.10–38.40(0.195)–Median36.4035.8036.304 monthsMin. – Max.42.30–55.3036.80–54.2041.20–53.20(< 0.001^^)p_1_ < 0.001^^,p_2_ = 0.444,p_3_ = 0.001^^Median50.9043.2049.50t(p_0_)(< 0.001^^)(< 0.001^^)(< 0.001^^)Pairwise comparison bet. each 2 groups was done using Post Hoc Test (Tukey)PRF pulsed radiofrequency, PRP platelet rich plasma, Min minimum, Max maximum, n numbersStatistically significant at p ≤ 0.05 p: p value for comparing between the three studied groupsp_0_: p value for comparing between before and 4 months in each group p_1_: p value for comparing between RF and PRPp_2_: p value for comparing between RF and Control p_3_: p value for comparing between PRP and Control
Notably, PRP was associated with a greater incidence of complications (48%) than RF (24%) and steroids (28%) in terms of procedural pain, numbness, and allergic reactions in the forearm. However, these differences did not reach statistical significance, as indicated by p values of 0.092, 0.151, and 0.331, respectively (Fig. 9).Fig. 9. Comparison between the three studied groups according to complications
The percentage of reduction in different parameters among the three groups is illustared in (Table 4).Table 4. Descriptive analysis of the percent of reduction in different parameters in each groupPercent of reduction (%)PRF(n = 25)PRP(n = 25)Control(n = 25)VASMin. – Max.85.71–100.042.86–100.0100.0–100.0Median (IQR)100.0 (100–100)88.89 (75–100)100.0 (100–100)CSAMin. – Max.6.25–33.330.0–25.011.76–37.50Median (IQR)17.0 (14.0–22.50)9.73 (5.45–14.17)25.45 (22.33–29.23)BCTQ (SSS)Min. – Max.70.73–80.028.57–80.065.63–80.0Median (IQR)76.60 (74.36–80.0)67.39 (48.72–76.0)75.61 (72.97–78.26)BCTQ (FSS)Min. – Max.68.75–80.063.83–79.5967.74–80.0Median (IQR)75.61 (73.33–77.78)72.50 (70.0–75.61)75.0 (72.97–77.78)PRF pulsed radiofrequency, *PRP *platelet rich plasma
Discussion
In the current study, US-guided median nerve PRP injection, steroid injection and PRF yielded significant improvements in the VAS score, BCTQ score, and NCV at all follow-ups compared with those at baseline, with comparable improvements between the PRF group and the steroid group after four months and significantly less improvement in the PRP group.
Consistent findings underscore the short-term efficacy of perineural steroid injection treatment [14],it is postulated to attenuate inflammation via the reducion of the expression of acute inflammatory factors such as CRP and IL-6 and edema affecting the nerve and surrounding tissues within the carpal tunnel, thereby diminishing the pressure exerted on the median nerve [15] though recent molecular genetic analyses have challenged this traditional view and have focused on the anti-fibrinolytic properties as reported on the downregulation of fibrosis related genes Col1A1 (collagen type 1 alpha 1 chin), Col1A2, and Col3A1 in ten patients who underwent ultrasound-guided injection with triamcinolone acetonide [16].
However, divergent reports persist regarding long-term outcomes. Enhanced results are anticipated in cases of milder symptoms, those persisting for less than one year, and less severe electrophysiological findings. A dosage of 40 mg of triamcinolone acetonide is frequently utilized, or its equivalent steroid dosages, with an average injection volume of 3.54 mL recommended for median nerve mobilization, ensuring adequate hydrodisection and superior distribution of the steroid dosage around the nerve. A dosage of 10 mg of triamcinolone acetonide may prove more advantageous in mitigating adverse effects. Ultrasound-guided injection for carpal tunnel syndrome enhances precision, minimizes the risk of intraneural injection, alleviates pain, and augments both efficacy and outcomes in comparison to the traditional landmark technique [17, 18].
The current study posits enhanced short-term to mid term clinical outcomes following PRP injections upto 4 months. There exists a compelling body of evidence supporting the potential of PRP in fostering nerve regeneration, including: neuroprotection and the prevention of neuronal apoptosis, stimulation of vascular regeneration, facilitation of axonal regeneration, modulation of the inflammatory response within the microenvironment, mitigation of nerve-related muscle atrophy, and enhancement of parameters associated with the human nervous system [6].
Similar finding were published by Benny et al. [19], where they compared perineural PRP injection compared to the steroids, they confirmed the short term improvement up to 12 weeks in all clinical outcomes including functional status (BCTQ FSS), symptom severity (BCTQ SSS) and CSA of the median nerve at carpal tunnel inlet.
Perineural injection of PRP has been extensively documented as a viable treatment option for CTS, demonstrating that PRP more effective than other conservative methods including steroid injection, night splinting and saline injection [20] in terms of pain reduction, improved function, and distal sensory latency improvement.Another meta-analysis demonstrated that platelet-rich plasma (PRP) injection surpasses other conservative management strategies, including wrist splinting and local injections with steroids, hyaluronidase, dextrose, and normal saline, in alleviating pain, enhancing wrist functionality and symptoms, diminishing median nerve swelling, and partially ameliorating electrophysiological parameters [21]. Others demonstrated PRP as promising therapy in short and midterm outcomes [22, 23].However, the long-term adverse side and consensus on standardization of PRP in CTS patients still need further large-scale trials.
The disparity between the results of the PRP is attributed to variations in PRP preparation techniques, which currently lack uniformity, including the volume of blood withdrawn, centrifugation duration and speed, and preactivation of platelets prior to injection [24], and the volume of PRP used, as the reported volume in different studies varied between 1 and 3 ml. It was reported that the concentration of formed elements, growth factors and cytokines in samples of PRP varied according to the centrifugation method utilized [25].
The observed improvement in the PRP group in the current study may be attributed to the swift relief of compression resulting from hydrodissection of the median nerve. However, the decreased efficacy could be explained by the the expected delayed effect of the PRP or one of the predictor factors as proposed by Shen et al., who elucidated the predictive factors contributing to the efficacy of a single PRP injection in patients with moderate carpal tunnel syndrome (CTS), specifically in terms of achieving a 50% reduction in the (VAS). Notably, lower body weight (BW), superior (SNCV), and diminished (CSA) of the median nerve (MN) were correlated with favorable outcomes during the third and sixth month follow-up visits post-PRP injection. Among these variables, BW, distal motor latency (DML), and CSA emerged as significant predictive factors of the treatment outcome.DML was identified as the most robust predictor of potential outcomes, exhibiting the strongest association (odds ratio: 0.383 at three months and 0.530 at six months). They also noted that the number of good outcomers increase from 28 patients at 3 months to 43 at six months consistent with the prolonged effect of neural regeneration [26].
Enhancements in NCV parameters were observed across all three groups throughout the four-month evaluation period. However, the PRP group demonstrated a relatively diminished degree of advancement. This observation prompted a revisit to Hakan Uzun’s study conclusion, which posits that PRP provides only transitory symptomatic relief, lacking any significant differentiations in NCV studies conducted on mild cases, thereby corroborating prior findings [27]. Indeed, several researchers have reported discrepancies between clinical symptoms and electrophysiological outcomes, as the large myelinated fibers assessed during electrophysiological examinations do not adequately reflect the small sensory fibers associated with the symptoms of CTS. Furthermore, previous investigations have indicated that electrodiagnostic measurements possess inherent limitations in forecasting the therapeutic efficacy of conservative treatments, as nerve recovery is typically a protracted process that may extend up to 18 months [20].
In the present study, notable progressive enhancements in all clinical parameters were documented at various follow-up intervals in the PRF group.The mechanism of therapeutic effect of PRF in CTS is unclear.PRF exerts its therapeutic influence through potentially multifactorial, mechanisms, such as the modulation of nociceptive Aδ and C fibers, alongside alterations in the expression of mediators implicated in neuropathic pain. Further investigation is imperative to elucidate the mechanisms by which PRF exerts its effects in CTS [8, 28].
The body of literature remains limited regarding the comparative analysis of PRF in the context of CTS. To date, this represents the inaugural research to compare (PRP) with (PRF).However, a limited number of studies have been published that compare these treatments with other conservative measures and corticosteroid injections. Gupta et al. elucidate findings from investigations on (PRF) for CTS, demonstrating notable analgesic and functional advantages, evidenced by short-term pain alleviation and enhanced functionality. However, uncertainty persists regarding long-term benefits. PRF may represent a viable alternative, particularly considering the inherent side effects associated with local steroid injections, which include adverse local reactions such as atrophy and hypopigmentation, alongside a plethora of potential systemic complications. Their review was constrained by the variability in technical parameters, encompassing probe length, active tip, needle gauge, and treatment duration. Although the output voltage has infrequently been documented in the studies reviewed, it consistently adheres to a standard output of 45 V. Ultimately, the absence of standardization in PRF parameters complicates the comparison of outcomes across diverse studies [7].
Eren Celenlioglu and colleagues [28] reported comparable enhancements in NRS and BCTQ scores with both PRF and steroid injection for a period of up to three months. Individuals who underwent PRF treatment reported significantly quicker onset of pain relief than those who received steroid injections exclusively probably due late onset of the anti-inflammatory effects of the steroid injection. The results of their study is congruent to the current study despite using mixture containing dexamethasone 8 mg and 0.5 cc of bupivacaine 0.5% targeting the hydrodissection only under the median nerve.
Similarly, Chen et al. [5]conducted a prospective, randomized, controlled, single-blinded study comparing pulsed radiofrequency (PRF) treatment of the median nerve to nocturnal splinting. The ultrasound-guided PRF cohort exhibited a more rapid onset of therapeutic effects, with a median onset time of 2 days compared to 14 days, and demonstrated a more pronounced reduction in pain at each follow-up assessment up to the 12-week. Furthermore, there was a significant enhancement in scores on the BCTQ, a reduction in the CSA of the median nerve, and improved finger pinch strength relative to the control group. The side effects associated with PRF were minimal, primarily manifesting as transient tingling at the puncture site. However, the absence of significant differences in sensory nerve conduction velocity (SNCV) engenders ongoing debate regarding the correlation between electrophysiological evaluations and the severity of symptoms or functional status scores. Despite the similarities in results, notable distinctions exist between the current study, which employed the injection of local anesthetic following PRF to standardize the integral effect of volume injection hydrodissection across all groups,. Additionally, their study did not delineate the severity of CTS in the enrolled patients. The inclusion and exclusion criteria suggest that the study likely encompassed a spectrum of CTS severity, provided that the diagnosis was substantiated by clinical symptoms and electrophysiological assessments.
In the current study hydrodissection was done in all the groups below and under the nerve to separate the nerve from the underlying tendons and overlying retinaculum. This adjustment was implemented to mitigate the hydrodissection effects across all groups uniformly.However, existing literature indicates that the inclusion of bupivacaine in conjunction with PRP may diminish the therapeutic efficacy of PRP; thus, it was excluded from the formulation and relayed on the liquid nature of PRP for hydrodissection.Indeed lack of bupivacaine might have skewed the results of PRP especially in the complication of pain during injection and was added to the limitations [29].
In the present study, only minor complications were documented across all groups, underscoring the safety of all procedures conducted over a short-term duration of up to four months but still concerns about potential side effects of steroids like skin pigmentation, tendon atrophy, hyperglycaemia and others will always be compelling to pursue other therapeutic modalities with similar efficacy [30].
Limitations
Several limitations are evident within the study, including a brief follow-up duration; an extended follow-up period of six months is essential to thoroughly assess the long-term outcomes and complications associated with the study. Additionally, as a single-center investigation, the findings underscore the necessity for broader multicenter studies. The absence of a universally standardized protocol for the preparation of (PRP), along with the lack of platelet count measurement for each PRP sample. Furthermore, bupivacaine was excluded from the PRP in accordance with reports suggesting its potential to diminish therapeutic efficacy.
Conclusion
The present investigation proposes that utilizing ultrasound to guide hydrodissection of the median nerve, in conjunction with local anesthetics/steroids or PRP and PRF, can be deemed efficacious modalities for addressing mild to moderate cases of carpal tunnel syndrome. Notably, short-term functional outcomes upto 4 month duration of the study were improved through the use of PRF and steroid injections; these treatments also proved superior in relieving pain compared with PRP injections.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.