Clinician Experiences with Adolescents with Comorbid Chronic Pain and Eating Disorders
Emily A. Beckmann, Claire M. Aarnio-Peterson, Kendra J. Homan, Cathleen Odar Stough, Kristen E. Jastrowski Mano

TL;DR
This study explores how clinicians in the U.S. handle adolescents with both chronic pain and eating disorders, highlighting a need for better tools and training.
Contribution
The paper provides insights into clinician experiences and identifies gaps in diagnosis and collaboration for adolescents with comorbid chronic pain and eating disorders.
Findings
Clinicians often encounter adolescents with both chronic pain and eating disorders.
Clinicians report low confidence in diagnosing these comorbid conditions due to limited screening tools and training.
Collaboration and consultation among clinicians are common practices for managing these complex cases.
Abstract
Background/Objectives: Chronic pain and eating disorders are two prevalent and disabling pediatric health concerns, with serious, life-threatening consequences. These conditions can co-occur, yet little is known about best practices addressing comorbid pain and eating disorders. Delayed intervention for eating disorders may have grave implications, as eating disorders have one of the highest mortality rates among psychological disorders. Moreover, chronic pain not only persists but worsens into adulthood when left untreated. This study aimed to understand pediatric clinicians’ experiences with adolescents with chronic pain and eating disorders. Methods: Semi-structured interviews were conducted with hospital-based physicians (N = 10; 70% female; M years of experience = 15.3) and psychologists (N = 10; 80% female; M years of experience = 10.2) specializing in anesthesiology/pain,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
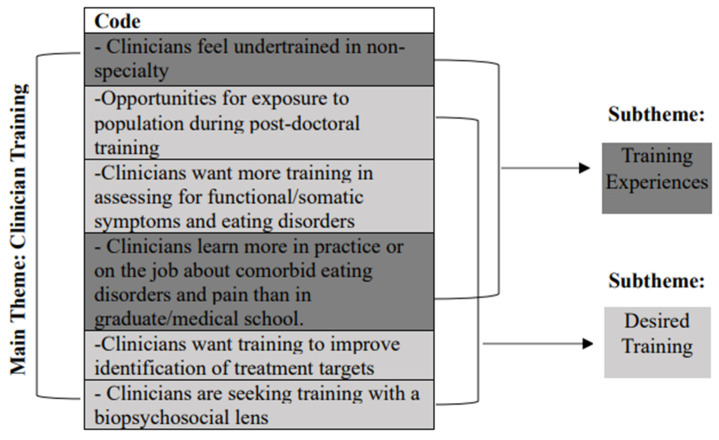 Figure 1
Figure 1- —Seeman Dissertation Fund at the University of Cincinnati
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Pain Management Techniques · Eating Disorders and Behaviors · Infant Health and Development
1. Introduction
Chronic pain and eating disorders are two highly prevalent conditions affecting adolescents. According to national estimates, 6% to 26% of children and adolescents between the ages of 6 and 17 experience chronic pain [1,2]. Eating disorders (EDs) are diagnosed in approximately 3.8% of adolescent females and 1.5% of males in the United States [3]. Moreover, approximately 13% of adolescents will develop an eating disorder upon transitioning to young adulthood [4]. Chronic pain, especially chronic functional abdominal pain, might put an individual at risk for the development of an eating disorder. A variety of pain-related symptoms, such as reduced appetite, dietary changes, nausea, and avoidance of movement can impact nutrition and weight, which in turn could trigger the development of an eating disorder [5,6]. Not only has it been demonstrated that adolescents with chronic pain are at risk for eating disorders, but the reverse pattern has also been noted. Specifically, adolescents with eating disorders can develop chronic pain [7]. Gastrointestinal distress is common among children and adolescents with eating disorders [7,8,9,10]. Research cites that as much as 25% of children and adolescents with restrictive eating also experience ongoing gastrointestinal distress, discomfort, and pain [11].
There are many shared risk factors that likely contribute to the co-occurrence of chronic pain and eating disorders in adolescents. It is possible that as a result of shared risk factors, adolescents with chronic pain are at increased risk for developing restrictive eating, and vice versa. Individuals with chronic pain and eating disorders possess shared temperamental risk factors, such as tendencies toward perfectionism [12] and harm avoidance [13]. Social factors also increase the likelihood of developing eating disorder pathology in adolescents with chronic pain [11,12]. Social reinforcement of weight loss is linked to increased frequency of restrictive eating behaviors to maintain low weight [6].
Despite the association between chronic pain and eating disorders, the identification, assessment, diagnosis, and treatment of comorbid chronic pain and eating disorders is challenging for clinicians. Sim and colleagues [6] found a significant delay in identification of eating disorders in adolescents with chronic pain compared to adolescents with an eating disorder without chronic pain. Hampered diagnosis is particularly problematic, as early detection is critical in both pediatric chronic pain [14] and eating disorder treatment effectiveness [15]. Postponed treatment has been linked to increased likelihood of pain and eating disorder symptoms becoming persistent, higher health care costs, and lower quality of life [15,16,17]. Moreover, eating disorders, particularly anorexia nervosa, have one of the highest mortality rates of any psychiatric disorder [18,19]. These statistics become incredibly salient in the context of comorbid eating disorders and chronic pain, as these individuals are diagnosed significantly later than those without the comorbidity [6].
Although no research has examined methods for identifying and assessing for co-occurring chronic pain and EDs, it is common practice for clinicians to conduct a physical exam and psychological assessment for patients with chronic pain or eating difficulties [20]. Comorbid chronic pain and eating disorders are likely difficult to diagnose, as many physical symptoms overlap [6]. Both conditions can involve weight fluctuation, food refusal, fasting, fatigue, orthostatic intolerance, early satiety, reflux, and/or constipation [21]. Despite such similarities, certain symptoms could serve as differentiators between the two conditions.
Sim and colleagues [6] highlighted behavioral signs of eating disorders for medical professionals to consider when seeing a patient with chronic pain who may also have an eating disorder. Behaviors such as tracking calories, having a calorie “goal” without input from a medical professional, excessive exercise, and body checking are often present in the context of an eating disorder, but are unlikely to be present in adolescents with chronic pain alone. Similarly, an intense fear of weight gain and significant body dissatisfaction are often reported by adolescents with anorexia nervosa [21] but would not likely be experienced by adolescents who have chronic pain without anorexia nervosa. A different eating disorder diagnosis also characterized by restrictive eating is avoidant restrictive food intake disorder (ARFID), which does not require body dissatisfaction or desire for weight loss for diagnosis. Indeed, identifying comorbid chronic pain and eating disorders is not a straightforward process. Despite the challenges associated with this complex presentation, no studies have explored clinician experiences in identifying, assessing, and treating comorbid chronic pain and eating disorders. Given the prevalence of eating disorders and chronic pain among adolescents, it is imperative to understand clinician experiences across specialties and care settings to improve the efficiency, accuracy, and ease with which clinicians assess, diagnose, and treat adolescents with comorbid chronic pain and eating disorders. Quickly addressing these concurrent, dangerous, and complex conditions could prevent mortality as well as unnecessary health care costs and low quality of life.
Present Study
Despite knowledge of the co-occurrence of chronic pain and eating disorders [11,22] and the danger of delayed diagnosis [6], there remains a lack of research on factors impacting identification, assessment, and treatment of comorbid chronic pain and eating disorders. Moreover, chronic pain and eating disorder patients present to several different pediatric clinics, yet no studies have considered cross-discipline clinician experiences with this population. Improved understanding of clinician perspectives on their work with adolescents with chronic pain and eating disorder symptoms is imperative for the rapid identification of symptoms, prevention of disease progression, and the advancement of treatment approaches. Additionally, determining clinician-identified strengths and weaknesses in professional education, training, and collaborative experiences could inform program development and refinement to support providers in building competence and confidence with this population.
The aim of the current study was to describe cross-disciplinary clinician experiences with adolescents who present with chronic pain and eating disorder symptoms in interdisciplinary academic medical center settings across the United States. The current study employed a cross-sectional phenomenological qualitative study design and utilized multi-disciplinary sources of reporting.
2. Materials and Methods
2.1. Study Questions, Design, and Setting
Consistent with phenomenological design, questions informed by emerging research were posed instead of hypotheses so that exploration of the phenomenon was not limited [23]. The exemplar study involved three primary research questions: (1) What are clinician experiences with adolescents with chronic pain and eating disorders? (2) What educational and training experiences in chronic pain and eating disorders have clinicians obtained throughout their careers? and (3) What experiences do clinicians have in consultation and collaboration with other providers when working with adolescents with chronic pain and eating disorders?
2.2. Participants
Participants were hospital-based clinicians at several academic medical centers across the United States. Participants were practicing physicians and psychologists with experience in identification, assessment, diagnosis, and/or treatment of adolescents with comorbid chronic pain and eating disorders. Inclusion criteria for the current study included the following: (1) participants were practicing physicians or psychologists in an academic medical center in the United States at the time of participation, (2) participants were required to have previous clinical experience with adolescents with chronic pain and eating disorders (the population of interest for the interview), (3) participants were English-speaking (language of the interview), (4) participants had required access to a device with video conferencing capabilities (participation took place over Zoom).
2.3. Participant Sampling and Recruitment
Participants were recruited using convenience, purposive, and snowball sampling techniques. Convenience sampling was the first techniques used to identify potential study participants in the selected pediatric academic medical centers. Pediatric academic medical centers were selected based on the presence of specialty clinics for eating disorders, gastroenterology, and/or pediatric pain as well as the presence of physicians and psychologists in the clinics. Study flyers were distributed to division directors in adolescent medicine, gastroenterology, and anesthesiology at several pediatric academic medical centers across the United States. Directors distributed flyers to physicians and psychologists working in the divisions and specialty clinics.
Purposive sampling and snowball sampling techniques were used to recruit participants following the distribution of study flyers. Purposive sampling allows researchers to identify and select participants who have direct experience with a phenomenon of interest, in this case, adolescents with eating disorders and chronic pain [24,25]. Snowball sampling allows for participants to recommend other contacts who might be interested in participating in the study using their own networks [26]. Interested clinicians were encouraged to contact the principal investigator briefly describing their experience with the population of interest. Consistent with previous research studies utilizing interview techniques within a phenomenological approach and a narrow scope, a sample size of 20 clinicians-physicians and psychologists was decided upon for the current study [27].
Prior to participation, the research team informed each participating clinician via email that they would be asked questions about their clinical experiences with adolescents with chronic pain and eating disorders. It was also explained that the interview audio would be recorded for transcription purposes and that the interview recordings would be de-identified and stored on a private server.
2.4. Semi-Structured Interview Guide
A semi-structured interview guide (see Table 1) was formulated by the research team based on the research questions. The guide was field tested with a physician and a psychologist with clinical experience with adolescents with chronic pain and eating disorders. The physician and psychologist completed field testing independently so as not to influence one another’s feedback. Feedback supported clarity and comprehensibility of the semi-structured interview guide. No amendments or modifications were made following field testing.
2.5. Interview and Data Acquisition
Interviews were open-ended, semi-structured interviews and conducted one-on-one with the PI and each participant. Interviews took place over the course of a 3-month period (January 2023–March 2023). The semi-structured interview guide allowed for the exploration of specific topics using pre-written interview questions, while also allowing for flexibility throughout the interview process to explore connected themes and spontaneous follow-up questions [28]. Interviews took place for approximately one hour with each clinician and the PI. The Zoom interview method was used for ease of recording and to afford each clinician the opportunity to participate at a time most convenient for them. In addition to the interview data, the PI gathered demographic information (e.g., gender identity, number of years of experience). Participants were compensated for their time with a $25 Amazon gift card.
2.6. Data Analysis
All audio recordings were transcribed verbatim using NVivo transcription software (V.13). Three researchers were involved in the data analytic process, including the PI and two undergraduate research assistants trained in qualitative data analysis and coding techniques. Consistent with the Braun and Clarke [29] approach to thematic content analysis, analysis was conducted in four phases. The four phases of thematic content analysis included the following: (1) reviewing of transcripts for errors and saturation, (2) initial coding, (3) code grouping and theme identification, (4) reviewing of themes [29].
The first phase involved reviewing the auto-transcription of de-identified interviews to correct any errors in transcription (e.g., “are feed” instead of ARFID). This step also involved the reading and re-reading of transcripts to evaluate thematic saturation and data quality. Researchers highlighted quotes of significance and key terms related to the research questions. Phase two involved initial coding using a hybrid method of deductive and inductive coding approaches. Each member of the research team independently coded each transcript to allow for the evaluation of intercoder reliability. The research team also met together at three separate times to assess intercoder agreement. Phase three focused on code grouping and theme identification. The research team collaboratively sorted through codes and grouped overlapping codes. Codes were grouped if a recurring pattern was observed across transcript data around a particular topic. The PI independently assigned the grouped overlapping codes into main themes and subthemes (see Figure 1 for an example). All identified themes were organized into a table with relevant codes and participant quotes (see Appendix A). The goal of phase four was to review identified main themes and subthemes. The research team collaboratively reviewed each main theme and subtheme in the table for agreement and finalization.
3. Results
3.1. Participants
Demographic information and participant characteristics for the study sample are summarized in Table 2. The final sample consisted of physicians (n = 10; M years of experience = 15.3) and psychologists (n = 10; M years of experience = 10.2) at several academic medical centers across the United States.
3.2. Themes
3.2.1. Main Theme 1: Clinical Practice
Codes falling under the main theme of clinical practice included statements from clinicians regarding where and how patients and their families presented for screening, assessment, and treatment. Moreover, clinicians described approaches to screening, assessment, and treatment and proposed approaches that might be effective to address comorbid chronic pain and eating disorders in the future.
Subtheme 1: Patient Presentation
Clinicians stated that the most common pain condition among patients they encounter when they see adolescents with comorbid chronic pain and eating disorders is chronic functional abdominal pain (CFAP). The majority of participating clinicians also noted that the most common eating disorder experienced by patients with comorbid chronic pain and eating disorders is avoidant restrictive food intake disorder (ARFID). Clinicians also spoke to the types of symptoms endorsed by patients when they presented to clinic. Specifically, clinicians shared that patients who sought care for chronic pain also endorsed eating disorder symptoms. Alternatively, some patients who sought care for an eating disorder were also found to have chronic pain symptoms. Clinicians commented on caregiver reports and perceptions at the time of patient presentation. Moreover, clinicians noted that caregivers often expressed fatigue and frustration related to their child’s symptoms. Caregivers also disclosed feelings of guilt and fear to clinicians in the context of treatment efforts and symptom management.
“By the time these patients get to me, the ones with functional pain, they’ve had the ultrasounds, the scopes, the colonoscopies… and they still don’t have answers as to what’s causing the pain. Then you have to tell them that there might not be an organic cause. That’s really tough.” (Physician, Anesthesiology)
Subtheme 2: Screening and Assessment
The subtheme of screening and assessment captures clinician experiences in the evaluation of adolescents with comorbid chronic pain and eating disorders. Codes categorized under this subtheme also highlight clinicians’ thoughts on what might be helpful in terms of improving screening and assessment of adolescents with chronic pain and eating disorders. Clinicians emphasized the importance of asking questions beyond the diagnosis(es) in their medical chart, especially if there are suspicions of a comorbid disorder. No participants reported the use of formal measures during the screening and assessment of adolescents with chronic pain and eating disorders. Despite the lack of validated screening and assessment measures, the majority of clinicians emphasized the importance of taking a careful and thorough history of symptoms.
“I’m looking at the behavior. If the kid is saying pain is impacting eating and daily activity yet is exercising a ton and eating foods that tend to cause gas and bloating, like cauliflower rice and sugar free stuff, I’m paying attention… alarm bells are going off.” (Psychologist, Pain)
Other notable topics addressed by clinicians regarding screening and assessment included determining what is driving food avoidance, challenges associated with teasing apart symptoms of pain and eating disorders, as well as the need for caregiver involvement in the screening and assessment process.
Subtheme 3: Intervention
Clinicians spoke to relevant treatment targets and factors impacting treatment in comorbid chronic pain and eating disorders. Transdiagnostic approaches were also proposed. Several clinicians spoke to challenges related to effective intervention in adolescents with chronic pain and eating disorders. Patients’ ability to participate in treatment was discussed by clinicians with an emphasis on medical stability. For example, if a patient is severely malnourished, they might not be able to engage in the physical demands associated with pain rehabilitation. The impact of caregiver buy-in to patient diagnosis(es) on intervention was also addressed. Clinicians proposed Family Based Treatment (FBT), a combination of Acceptance and Commitment Therapy and Cognitive Behavioral Therapy (CBT), as well as exposure therapy as potential intervention approaches to address both chronic pain and eating disorders. Lastly, clinicians spoke to the use of tube feeding and medications as other treatment options for patients.
“FBT is the gold standard as you know for eating disorder treatment. I still think it’s relevant for these kids who also have pain issues. These kids need to be eating and having parents take control is the best way to ensure that, because if we leave it up to the eating disorder or pain the kid isn’t going to eat.” (Physician, Adolescent Medicine)
3.2.2. Main Theme 2: Clinician Training
Clinician training represents clinician training experiences in graduate school, medical school, residency, and post-doctoral training, as well as peri-career training. The theme of clinician training also reflects desired training opportunities expressed by clinicians.
Subtheme 1: Training Experiences
In terms of training experiences, clinicians expressed feeling undertrained in their non-specialty. Physicians specifically noted that they felt undertrained in functional pain disorders and somatic symptoms. Psychologists expressed minimal training in graduate school for eating disorders. Additionally, clinicians shared that they learned more in practice and in their work than they learned in medical school or graduate school on complex presentations of chronic pain or eating disorders. Clinicians described previous discussions with colleagues about non-specialty cases, shadowing other clinicians at work. Many clinicians sought consultation and supervision to train in non-specialty areas.
“I have career long experience with eating disorders. In regard to pain, I don’t have any training. Of course, I have attended some workshops. I’ve talked with colleagues at the hospital.” (Physician, Adolescent Medicine)
Subtheme 2: Desired Training
Many clinicians spoke to training experiences that they desired or wished that they could have received earlier than post-doctoral training. Specifically, opportunities for exposure to their non-specialty in medical school and graduate school were endorsed. Clinicians shared that they wanted more training to assess for functional/somatic symptoms and eating disorders. Additional training experiences sought by clinicians included training to improve treatment targets and training with a biopsychosocial lens.
“It’s unfortunate, because the pain these kids have is real and we don’t always do a great job of validating functional stuff in the medical world. I’m not confident that I have the best language to respond when kids come in with functional pain or somatic symptoms. I would love more training on that.” (Physician, Adolescent Medicine)
3.2.3. Main Theme 3: Collaboration and Consultation
The main theme of collaboration and consultation entails clinician comments addressing referring patients to different specialty clinics and providers, the setting(s) in which they see patients, and collaboration with other providers.
Subtheme 1: Referrals
Clinicians reported referring cases to other providers and clinics when they did not feel like they had the expertise to diagnose and treat the patient. Clinicians described awareness of their competency. They also shared their preference to refer patients out when they felt that they might be practicing out of their scope.
“If ever I felt like someone needed true treatment for an eating disorder, I’m going to refer because I’m not, you know, I don’t have the expertise for that. So I don’t typically do the weight focus. I just say we have to stop the weight loss. How do we do that? Let’s come up with some strategies and go from there.” (Psychologist, Gastroenterology)
Subtheme 2: Care Setting
Communication with other providers in different care settings was addressed by participating clinicians. Physicians discussed communication with mental health professionals in the community and within the academic medical center setting. Psychologists also discussed communicating with community providers on complex cases where the patient was also seen at an academic medical center. Moreover, clinicians highlighted the strengths associated with working with adolescents with comorbid chronic pain and eating disorders in an interdisciplinary setting. Clinicians expressed the difficulty in finding a higher level of care options for adolescents with comorbid chronic pain and eating disorders, as many inpatient pain rehabilitation programs do not accept adolescents with eating disorders, and inpatient eating disorder programs often do not accept adolescents with a co-occurring chronic pain diagnosis.
“In the inpatient intensive rehab program for kids who have been affected by chronic pain, you can’t walk, is in a wheelchair, can’t attend school, they manage everything except for eating. You must be able to eat. Otherwise, they’re not able to participate, which makes no sense to me. They have to be strong enough nutritionally to do physical therapy, but they can’t restore nutritionally because of chronic pain. Our eating disorder program doesn’t accept kids with chronic pain either.” (Physician, Adolescent Medicine)
Subtheme 3: Collaboration
Collaboration was addressed by participating clinicians. They described feeling confident in knowing who to ask or consult within an interdisciplinary team if they felt uncertain or wanted advice on a patient with comorbid chronic pain and eating disorders. They also spoke extensively about defining roles within the treatment team. Clinicians collaborated with the patient’s treatment team and saw the benefit in allowing each team member to address patients’ needs in their domain. For example, psychologists described referring to adolescent medicine for questions related to medical stability and to dietitians for caregiver questions about calorie requirements and meal plans.
“It’s so important to collaborate on our teams. I don’t know how many calories a patient should be consuming. I don’t have that expertise, so I loop in their dietitian if there are questions. I also don’t know if they’re orthostatic by heart rate or blood pressure unless they’re following with a pediatrician. We need to work together.” (Psychologist, Eating Disorders)
4. Discussion
The present study was the first to explore physician and psychologist experiences working with adolescents with comorbid chronic pain and eating disorders. A qualitative design was used with deductive and inductive approaches to thematic analysis to characterize cross-disciplinary clinician experiences with this population. Results support existing research suggesting that patients can develop pain symptoms prior to and after the onset of eating disorder symptoms [6]. Findings not only demonstrate how patients present with comorbid chronic pain and eating disorders, but also how their caregivers present. Specifically, clinicians reported awareness of caregiver emotions and wellbeing. Per clinician report, caregivers presented with treatment fatigue and frustration, as well as fear and guilt. Research has demonstrated a relationship between caregiver expressed emotion and treatment outcomes in adolescents [30,31]. Taken together, these findings emphasize the salience of family-centered care for adolescents with comorbid chronic pain and eating disorders.
Clinicians noted their desire for screening tools [32] and described their rationale for examining behavioral signs of pain and eating disorders as a critical component of the assessment process. This is consistent with guidelines provided by Sim and colleagues for individuals working with adolescents with chronic pain and eating disorders [6], which encouraged the use of screening tools in the assessment process and included a list of behavioral signs of eating disorders. Clinicians who participated in the present study also commented on the challenges associated with teasing apart symptoms of pain and eating disorders. Consistent with anticipated diagnostic features, clinicians spoke to weight loss, avoidance, functional disability, food restriction, constipation, and body dissatisfaction. Moreover, clinicians did not endorse using specific assessment approaches.
Regarding intervention, clinicians emphasized the effectiveness and utility associated with FBT, CBT, and exposure therapy for comorbid chronic pain and eating disorders. Previous research demonstrated the use of these interventions for pediatric chronic pain, with the exception of FBT [33,34]. Evidence has also been shown for the effectiveness of CBT and exposure therapy for the treatment of eating disorders [35,36,37], but research has not examined the effectiveness of these treatment modalities for co-occurring pain and eating disorders. Many clinicians hypothesized that adapted versions of these interventions could be effective at treating chronic pain and eating disorders simultaneously if the adolescent is medically stable.
Clinicians described feeling undertrained in their non-specialty. For example, physicians and psychologists who worked in adolescent medicine and eating disorders noted that they did not receive much training in functional pain or somatic symptom disorder during medical or graduate school. Indeed, existing research supports that clinicians do not receive significant graduate level training in somatic symptoms [38,39]. The present study builds upon this literature, as the majority of clinicians desired more training in complex presentations of functional pain and eating disorders at the medical school and graduate level.
Clinicians reported a preference to refer cases to other providers and clinics when they did not feel like they had the expertise to diagnose and treat the patient. Regarding the care setting subtheme, communication with other providers in different care settings was addressed by participating clinicians. Physicians and psychologists shared that they communicate with community providers and within the academic medical center setting on complex cases. An important finding related to the referral and care setting subtheme is that low perceived competence and confidence in working with patients with complex presentations increased the likelihood of clinicians referring patients to clinicians in other disciplines and specialties. Clinicians also shared that they felt confident in knowing who to ask or to consult within an interdisciplinary team if they felt uncertain or wanted advice on a patient with comorbid chronic pain and eating disorders. Together, these findings suggest that collaboration was helpful to increase clinician confidence. However, training is what clinicians linked to increasing their competence in addressing adolescents with this comorbid chronic pain and eating disorders.
4.1. Clinical Implications
Findings from the present study demonstrate the complexity of patient presentation as well as variability in approaches to screening, assessment, diagnosis, and treatment of adolescents with comorbid chronic pain and eating disorders. Clinicians could benefit from increased development and use of practical and simple screening and assessment tools, such as the recently validated Eating Attitudes Test–16–Chronic Pain [32]. Moreover, results highlight the impact that previous health care (e.g., medical testing, treatment fatigue, medicalization of patient) can have on patient and family presentation.
Results also highlight the lack of training at the medical school and graduate level and that training at this level is desired by clinicians. Future program development efforts might aim to build in education for functional pain and somatic symptoms as well as diversity in eating disorder presentations for physicians and psychologists at the graduate level. Additionally, internship/residency and post-doctoral programs could increase training opportunities on rotations to increase exposure and consequently confidence in working with complex presentations of medical and psychiatric conditions.
Several themes captured the importance of an interdisciplinary setting for the care of adolescents with comorbid chronic pain and eating disorders. Research should determine barriers to the development of outpatient, partial hospitalization, and inpatient interdisciplinary pain and eating disorder programs in order to provide adolescents with comprehensive care at a level that is most appropriate for the acuity of their condition and to meet the needs of the patient and their family.
4.2. Limitations and Future Directions
It is imperative to understand the limitations of the present study. Although we reached thematic saturation with 20 participants, the sample of physicians and psychologists was small. Thus, we were unable to examine, for example, differences in responses based on when clinicians completed their medical and subspecialty training. Further, all anesthesiologists interviewed in our study practiced within integrated pediatric pain clinics that were structured around interdisciplinary models of care, involving collaboration among physicians, psychologists, and other specialists. Though this recruitment approach was deliberate given that interdisciplinary approaches are essential when treating youth with complex conditions, the perspectives of clinicians working in family medicine, community clinics, and private practice may differ from those of clinicians working with adolescents with chronic pain (and/or eating disorders) in interdisciplinary clinics in academic medical centers. Future research might also aim to obtain a wider sample of providers, including pain medicine physicians, psychiatrists, nurses, physiotherapists, and dietitians.
An additional limitation related to the study design is that the interviews were conducted virtually. Although the Zoom method increases accessibility, as participants do not have to travel to a research lab, virtual interviews could impact participant comfort and also require that participants have specific technology [40]. Participants were required to have access to the internet, a device with video conferencing capability, and a secure space. Therefore, consideration of the impact on available office space and/or devices for potential participants was important. Also, important to note, all interviews took place with an interviewer who is in the psychology field, which could have impacted physician willingness to share negative experiences associated with psychology colleagues. Future studies may consider matching interviewer and participant on this domain, or perhaps conduct group interviews or focus groups with participants representing varied training backgrounds and areas of expertise.
5. Conclusions
The current study contributes to the existing literature by providing insight into clinicians’ experiences with adolescents with comorbid chronic pain and eating disorders. Results also indicate clinicians’ desire for more graduate and post-doctoral training in somatic symptoms, functional pain, and eating disorders. Participants emphasized the importance of working collaboratively with other specialties and disciplines to increase clinician confidence and competence in the identification, assessment, and treatment of adolescents with chronic pain and eating disorders.
Results highlight future directions for the development of specific screening questions, assessment tools, and intervention strategies for adolescents with comorbid chronic pain and eating disorders. Moreover, this study presents targets for improved education and training in pediatric functional pain and eating disorders as well as opportunities to optimize collaboration and consultation across medical and psychiatric settings, disciplines, and specialties.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Groenewald C.B. Beals-Erickson S.E. Ralston-Wilson J. Rabbitts J.A. Palermo T.M. Complementary and alternative medicine use by children with pain in the United States Acad. Pediatr.20171778579310.1016/j.acap.2017.02.00828232257 PMC 5598558 · doi ↗ · pubmed ↗
- 2Tumin D. Miller R. Hakim M. Shafy S.Z. Drees D. Wrona S. Smith T. Tobias J.D. Bhalla T. Predictors of referral to a pediatric outpatient chronic pain clinic Clin. J. Pain 20193520521110.1097/AJP.000000000000066430303827 · doi ↗ · pubmed ↗
- 3American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders (DSM-5®)American Psychiatric Publisher Washington, DC, USA 2013
- 4Austin A. Flynn M. Shearer J. Long M. Allen K. Mountford V.A. Glennon D. Grant N. Brown A. Franklin-Smith M. The First Episode Rapid Early Intervention for Eating Disorders—Upscaled study: Clinical outcomes Early Interv. Psychiatry 2022169710510.1111/eip.1313933781000 PMC 9291113 · doi ↗ · pubmed ↗
- 5Hilbert A. Pike K.M. Goldschmidt A.B. Wilfley D.E. Fairburn C.G. Dohm F.A. Walsh B.T. Weissman R.S. Risk factors across the eating disorders Psychiatry Res.201422050050610.1016/j.psychres.2014.05.05425103674 PMC 4785871 · doi ↗ · pubmed ↗
- 6Sim L.A. Lebow J. Weiss K. Harrison T. Bruce B. Eating disorders in adolescents with chronic pain J. Pediatr. Health Care 201731677410.1016/j.pedhc.2016.03.00127021242 · doi ↗ · pubmed ↗
- 7Sato Y. Fukudo S. Gastrointestinal symptoms and disorders in patients with eating disorders Clin. J. Gastroenterol.2015825526310.1007/s 12328-015-0611-x 26499370 · doi ↗ · pubmed ↗
- 8Boyd C. Abraham S. Kellow J. Psychological features are important predictors of functional gastrointestinal disorders in patients with eating disorders Gastroenterology 20054092993510.1080/0036552051001583616170899 · doi ↗ · pubmed ↗