Scrotal Migration of the Ventriculoperitoneal Shunt in a 1-Year-Old Pediatric Patient: A Case Report and Systematic Literature Review
Zenon Pogorelić, Stipe Ninčević, Vlade Babić, Miro Jukić, Stipe Vidović

TL;DR
A 1-year-old child's ventriculoperitoneal shunt migrated to the scrotum, and laparoscopic surgery successfully treated it.
Contribution
This case report and systematic review provide insights into the treatment of rare scrotal migration of VPS in pediatric patients.
Findings
Laparoscopic repositioning of the VPS catheter and closure of the processus vaginalis was effective in 90.4% of cases.
Scrotal/inguinoscrotal swelling was the most common symptom among 52 pediatric patients analyzed.
The median age at presentation for scrotal VPS migration was 24 months.
Abstract
Background: Migration of the peritoneal end of the ventriculoperitoneal shunt (VPS) into the scrotum is a rare but recognized complication. Inguinoscrotal migration typically occurs as a result of increased intra-abdominal pressure combined with a patent processus vaginalis. A 14-month-old pediatric patient presented to the emergency department with abdominal pain, vomiting, and swelling of the right scrotum that had persisted for two days. The patient had a history of a head injury that had resulted in a large secondary arachnoid cyst for which a VPS had been placed at eight months of age. Examination of the inguinoscrotal region revealed a swollen and painful right side of the scrotum with a hydrocele and a palpable distal portion of the ventriculoperitoneal catheter in the right groin extending to the scrotum. After a brief preoperative preparation, the patient underwent laparoscopic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
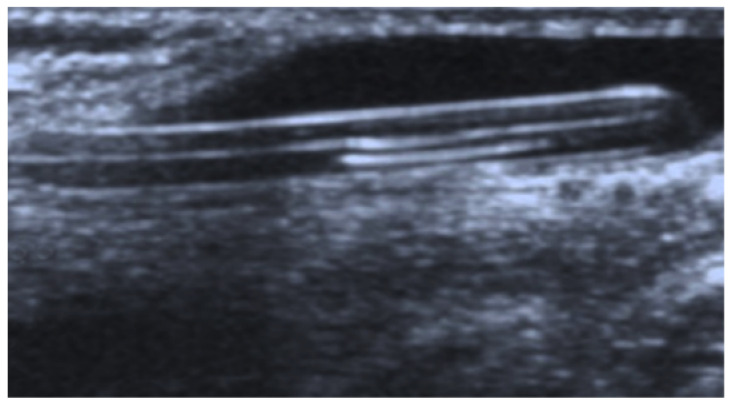 Figure 1
Figure 1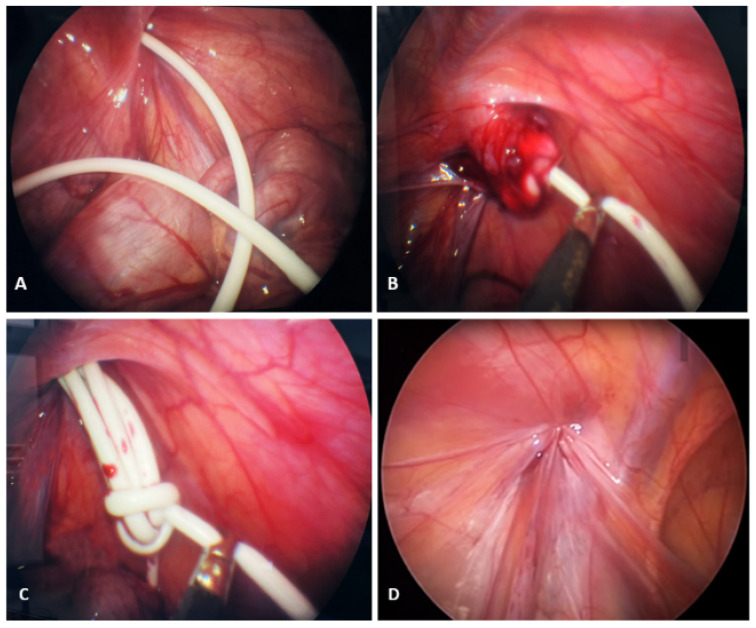 Figure 2
Figure 2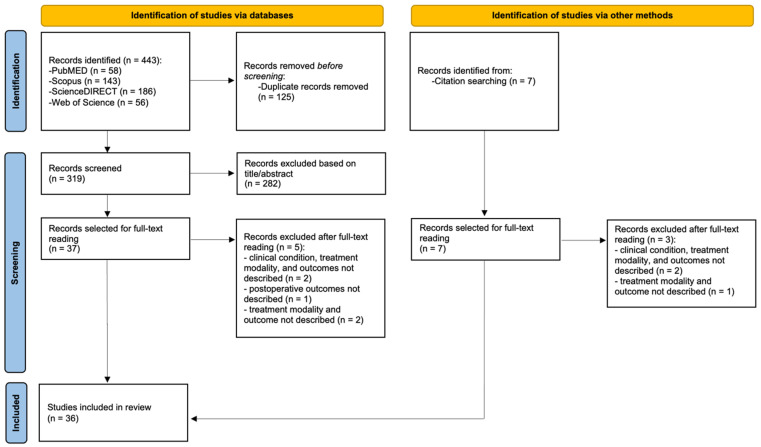 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Spinal Dysraphism and Malformations · Fetal and Pediatric Neurological Disorders
1. Introduction
Hydrocephalus is defined as the accumulation of cerebrospinal fluid (CSF) within the cerebral ventricles, resulting from either primary (congenital, developmental, or genetic) or secondary causes, such as central nervous system (CNS) infections, meningitis, brain tumors, head trauma, or spontaneous intracranial hemorrhage [1]. Based on the underlying mechanism, hydrocephalus can be classified into communicating, non-communicating (obstructive), ex-vacuo hydrocephalus, and normal pressure hydrocephalus [2].
The ventriculoperitoneal shunt (VPS) remains the most commonly performed surgical treatment for hydrocephalus in the pediatric population and is currently the most frequent procedure in pediatric neurosurgery [3,4]. A typical VPS system consists of two components: a proximal catheter that diverts CSF from the ventricles, and a distal catheter that typically terminates in the peritoneal cavity. Other alternative distal sites include the right atrium (ventriculoatrial shunt), pleural space (ventriculopleural shunt), and the lumbar subarachnoid space connected to the peritoneum (lumboperitoneal shunt) [5]. It is estimated that approximately 30,000 shunt procedures are performed annually in the United States. VPS-related complications may be classified as mechanical, infectious, or functional [6]. Functional complications include CSF overdrainage, valve malfunction, catheter breakage, obstruction, coiling, or spontaneous knot formation [7,8].
The most common causes of shunt failure in both children and adults are obstruction and infection, with infection typically leading to early shunt failure, while catheter obstruction is more often associated with late failure [8,9]. Studies have identified several risk factors for shunt malfunction, including patient age, prior surgeries before shunt placement, the underlying etiology of hydrocephalus, and the specific type of hydrocephalus [10]. Patients with congenital hydrocephalus or spinal dysraphism have been shown to have a significantly higher incidence of shunt malfunction compared to those with other etiologies. In contrast, patients with normal pressure hydrocephalus (NPH) exhibit the lowest rates of shunt revision [11].
Mechanical complications of the VPS include migration of the catheter into the thoracic cavity, heart, bladder, hernia sacs, anus, and distal part of the scrotum, which can lead to infection and/or inadequate CSF drainage, which, in turn, can cause obstructive hydrocephalus [12]. Although cases of scrotal migration of the distal catheter have been reported in adults, they are rare due to obliteration of the processus vaginalis [7]. Consequently, this complication is more commonly observed in pediatric patients, where the processus vaginalis often remains patent. Scrotal migration may lead to more serious clinical manifestations, including scrotal edema, acute scrotum, abdominal pain, and even shunt extrusion [13].
In the past, the open surgical approach was considered the gold standard for the treatment of inguinal hernia or a patent processus vaginalis. The most commonly employed technique involved high ligation of the hernia sac [14]. However, with significant advancements in minimally invasive pediatric surgery, instruments have been developed that enable these procedures to be performed even in neonates and small children. As a result, virtually all pediatric abdominal surgeries can now be carried out laparoscopically [15]. In recent years, the percutaneous internal ring suturing (PIRS) technique has gained particular popularity among pediatric surgeons for the treatment of indirect inguinal hernias, offering excellent outcomes and very low recurrence rates [16].
In this report, we present a rare case of a VPS catheter loop within the right scrotum of a 14-month-old pediatric patient, which resulted in a painful hydrocele and was successfully managed using a laparoscopic approach. In addition, we present the findings of a systematic review of the literature.
2. Case Presentation
A 14-month-old pediatric patient presented to the emergency department of our hospital with abdominal pain, vomiting, and swelling of the right scrotum that had persisted for two days. The patient had a history of head injury resulting in a large secondary arachnoid cyst, for which a VPS had been placed at 8 months of age. Until two days before admission, the patient was in good general condition, growing and developing normally, and the VPS was functioning normally.
On physical examination, the patient was anxious and irritable, but hemodynamically stable and afebrile. The abdomen was soft, with no signs of peritoneal guarding. Examination of the inguinoscrotal region revealed a swollen and painful right side of the scrotum with a hydrocele and a palpable distal portion of the VP (ventriculoperitoneal) catheter in the right groin extending towards the scrotum. The scrotal ultrasound revealed a normal testicle, with no signs of inflammation, swelling, or torsion.
A scrotal ultrasound was performed, which showed a moderate hydrocele on the right side and the individualization of tubular echogenic material therein, which was consistent with the distal end of the VP catheter (Figure 1).
After a brief preoperative preparation, the patient underwent an emergency laparoscopic abdominal exploration. A supraumbilical incision was made, a 5 mm trocar was inserted, and an 8-mmHg pneumoperitoneum was established. Exploration of the abdominal cavity revealed a VP catheter in the abdomen, the end of which entered the inguinal canal and scrotum through an open processus vaginalis (Figure 2A). After the insertion of two additional lateral 3.5 mm trocars, an attempt was made to reposition the VP catheter in the abdominal cavity using gentle movements, but this was met with resistance. Even after stronger traction, it was not possible to pull the catheter into the abdominal cavity (Figure 2B), which is why the laparoscopic incision of the hernia sac was performed using laparoscopic scissors, and the catheter was pulled out of the scrotum into the abdominal cavity, after the adhesions had been dissected. After the catheter had been pulled out completely, it was found that the long part of the catheter was lying in the scrotum and was buried around its axis (Figure 2C). The catheter was repositioned in the pelvis. The internal opening of the inguinal canal was then closed using the percutaneous internal ring suturing (PIRS) method [17], as shown in Figure 2D. At the end of the procedure, the VP catheter was checked and found to be functioning normally. The skin incisions were closed with Steri-Strip adhesive bands (3M^TM^ Steri-StripTM, Neuss, Germany).
After surgery, the patient was observed in the pediatric surgery department. Oral intake was initiated two hours after surgery. Ibuprofen at a dose of 10 mg/kg was used for analgesia. The patient was discharged from the hospital after 24 h in good general condition, pain-free, and afebrile. At the follow-up examination seven days later, the Steri-Strip adhesive bands were removed, and the surgical incisions had healed well. At six-month follow-up, the patient is in good general condition, pain-free, the VP catheter is functioning properly, and there are no signs of recurrent inguinal hernia.
3. Methods
The following paragraphs relate to the methodology of the systematic review on scrotal migration of the VPS in the pediatric population.
3.1. Inclusion and Exclusion Criteria
The inclusion and exclusion criteria for the systematic review are presented in Table 1.
3.2. Data Sources and Search Strategy
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A literature search was performed by reviewers S.V. and Z.P. on 10 April 2025, across four electronic databases: PubMed, ScienceDirect, Scopus, and Web of Science. Boolean logic expressions were used for the search without applying any filters, as follows: PubMed: ((ventriculoperitoneal shunt) AND (scrotal migration)); Scopus: ((ventriculoperitoneal shunt) AND (scrotal migration)); ScienceDirect: ((ventriculoperitoneal shunt) AND (scrotal migration)); and Web of Science: TS = ((ventriculoperitoneal shunt) AND (scrotal migration)). In addition to the electronic search, a manual screening of the reference lists from the selected articles was conducted by reviewers S.V. and Z.P. to identify any further relevant studies.
3.3. Study Selection and Data Collection Process
Following the removal of duplicate records, reviewers S.V. and Z.P. collaboratively screened the titles and abstracts of all articles retrieved through the electronic database search. Studies selected for full-text review were identified according to the predefined inclusion and exclusion criteria (Table 1). After evaluating the full texts, articles that did not meet the eligibility criteria were excluded, with reasons for exclusion recorded. Additionally, S.V. and Z.P. manually reviewed the reference lists of the included studies to identify and incorporate any further eligible articles.
For each study included in the systematic review, data extraction was carried out by reviewers S.V. and Z.P. The following information was collected when available: author(s), year of publication, country of origin, study design, and sample size. Patient-related data were also extracted, including age, indication for VPS placement, presenting symptoms, time to clinical presentation following VPS insertion, imaging and laboratory findings, presence of inguinal hernia, type of treatment administered, intraoperative and postoperative complications, length of hospital stay, mortality, and duration of follow-up for patients with scrotal migration of the VPS.
3.4. Risk of Bias Assessment of Included Studies
To evaluate the methodological quality and potential bias of the studies included in the review, the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports and the JBI Critical Appraisal Checklist for Case Series were utilized [18]. Two reviewers (S.V. and Z.P.) independently assessed each item on the relevant checklist, assigning one of four possible responses: ‘Yes’, ‘No’, ‘Unclear’, or ‘Not applicable’. Discrepancies between the reviewers were addressed and resolved through discussion. For scoring, each ‘Yes’ response was awarded one point, while ‘No’, ‘Unclear’, and ‘Not applicable’ responses received zero points. The total score was determined by summing the points from all ‘Yes’ responses and was then converted into a percentage by dividing by the maximum possible score. Based on this percentage, the methodological quality of each study was classified as low (<50%), moderate (50–74%), or high (>75%).
3.5. Statistical Analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS, Version 28.0; IBM Corp., Armonk, NY, USA). The normality of numerical data was assessed using the Shapiro–Wilk test. As the distributions were non-normal, numerical variables were expressed as medians and interquartile ranges (IQRs), while categorical variables were summarized using absolute numbers and relative frequencies (percentages). Missing data were not imputed; analyses were based on available data only. For each variable analyzed, percentages were calculated using only the total number of participants from studies that reported data for that specific variable. Studies that did not provide data for a given variable were excluded from the denominator in those calculations.
4. Results
4.1. Study Selection
The database search initially identified 443 studies, of which 125 were duplicates. Based on the screening of titles and abstracts according to the predefined inclusion and exclusion criteria (Table 1), 282 records were excluded. Subsequently, 37 articles were selected for full-text review, after which 5 were excluded due to the absence of a described clinical condition, treatment modality, or reported outcomes. In addition, a manual search of reference lists identified seven more studies, of which three were excluded after full-text assessment for the same reasons. Ultimately, 36 studies were included in the systematic review. The literature search flow diagram is presented in Figure 3.
4.2. Study Characteristics
Ultimately, the review incorporated 30 case reports and six case series, and the key characteristics of these studies are presented in Table 2.
4.3. Risk of Bias in Studies
Upon assessing the methodological quality and risk of bias using the JBI Critical Appraisal Checklist for Case Series (Table 3) and the JBI Critical Appraisal Checklist for Case Reports (Table 4), 18 studies were classified as high quality, 16 as medium quality, and 2 as low quality based on the overall quality assessment score.
4.4. Summary of the Included Studies
A review and analysis of the 36 studies included in this article identified a total of 52 pediatric patients with VPS scrotal migration. The median age was 24 months (range: 1–169 months). For 51 patients, the indication for VPS placement was described, and all of them had hydrocephalus, of which 11 (21.6%) cases were congenital. Furthermore, the hydrocephalus was secondary to various underlying conditions, including myelomeningocele (n = 5, 9.8%), meningitis (n = 3, 5.9%), aqueductal stenosis (n = 3, 5.9%), tumor (n = 3, 5.9%), hemorrhage (n = 3, 5.9%), and Chiari malformation (n = 3, 5.9%). For 49 patients, the side of VPS migration was reported; of these, 34 (69.4%) occurred on the right side and 15 (30.6%) on the left side. The time from VPS placement to the onset of symptoms was available for 47 patients, with a median of 9.0 months (range: 1 day–72 months). The most commonly reported symptoms were scrotal/inguinoscrotal swelling (n = 50, 96.2%), vomiting (n = 7, 13.5%), and fever (n = 3, 5.8%). Diagnostic methods were reported for 49 patients and included abdominal X-ray (n = 43, 87.8%), ultrasound (n = 5, 10.2%), scrotal transillumination test (n = 5, 10.2%), and computed tomography (CT) (n = 1, 2.0%). An inguinal hernia was reported in 19 patients. Key characteristics and clinical findings of patients with VPS scrotal migration are summarized in Table 5.
Regarding treatment, surgical repositioning of the VPS into the peritoneal cavity was performed in 47 patients (90.4%). A laparoscopic approach was described in two patients (3.8%). Non-operative manual repositioning was reported in two cases (3.8%), and spontaneous resolution of VPS migration from the scrotum occurred in three patients (5.8%). The length of the hospital stay was reported in 15 patients, with a median duration of 3.2 days (range: 1–10 days). No intraoperative or postoperative complications were observed. Follow-up data were available for 12 patients, with a median follow-up period of 19.1 months (range: 1–120 months). Treatment approaches, intraoperative and postoperative complications, length of hospital stay, and mortality outcomes for patients with VPS scrotal migration are summarized in Table 6.
5. Discussion
This paper presents a relatively rare case of scrotal migration of the peritoneal end of a VPS in a one-year-old child. To our knowledge, it also represents the first systematic review of the literature focusing on scrotal migration of VPS in the pediatric population.
Several theories have been proposed to explain the scrotal migration of ventriculoperitoneal shunts (VPS), with the most widely accepted attributing it to increased intra-abdominal pressure [10,19]. This pressure can impede the natural obliteration of the processus vaginalis (PV), providing a potential pathway for distal catheter migration into the scrotum. This condition is especially prevalent in neonates and young children, in whom the PV remains open in up to 90% of cases at birth and gradually closes with age [52]. Furthermore, the combination of a smaller peritoneal cavity, the vertical orientation of the inguinal canal in early life, and the “funnel effect” created by a patent PV further facilitates this type of migration [30]. Collectively, these anatomical and physiological factors contribute to the increased risk of scrotal migration of the distal end of the VPS.
Studies indicate that the primary indication for VPS placement in children is hydrocephalus, which is often secondary to a variety of underlying conditions, including myelomeningocele, aqueductal stenosis, meningitis, brain tumors, intraventricular hemorrhage, and Chiari malformation [3,10,13,19,20,21]. In our case, the patient had a history of head trauma that led to the development of a large secondary arachnoid cyst, which necessitated VPS placement.
Findings from previous studies suggest that scrotal migration of VPS may occur more frequently on the right side, as was also observed in our case [3,10,13,19,20,21]. This pattern can be attributed to several anatomical and developmental factors. The processus vaginalis is known to remain patent longer on the right, increasing the likelihood of it serving as a pathway for shunt migration [52]. Additionally, right-sided inguinal hernias may be more common in the pediatric population, likely due to asymmetries in testicular descent and differences in the timing of processus vaginalis closure between the two sides [53,54,55]. The anatomical configuration of the peritoneal cavity may further contribute, as the spleen on the left side can act as a physical barrier, limiting catheter mobility in that direction [51]. Collectively, these factors may explain the observed predominance of right-sided VPS migration in children.
Furthermore, studies indicate that the most commonly reported symptoms associated with scrotal migration of VPS are scrotal swelling, vomiting, and fever (Table 5), which aligns with the clinical presentation observed in our patient. In addition to physical examination, ultrasound was used in our case to establish the diagnosis. According to the literature, the most frequently employed confirmatory diagnostic modality is abdominal X-ray, followed by ultrasound of the inguinoscrotal region, a positive transillumination test, and computed tomography (Table 4).
Regarding the treatment of VPS scrotal migration, studies indicate that the most common approach is surgical repositioning of the catheter into the peritoneal cavity (Table 6). In cases where an inguinal hernia is present, hernia repair is typically performed concurrently, as was performed in our case. No intraoperative or postoperative complications have been reported in the reviewed literature (Table 6). In our case, a laparoscopic approach was used, and to the best of our knowledge, this approach has been previously described only by Ezzat et al., who reported successful laparoscopic repositioning of the VPS into the peritoneal cavity in two patients, also without complications [18]. Given that only one other study, in addition to ours, has described a laparoscopic approach, a comparison with the open surgical technique is not feasible. Additionally, two studies reported manual (non-operative) repositioning of the catheter [23,40], while spontaneous resolution of scrotal migration was documented in three patients [3,37,49]. Additionally, two studies reported manual (non-operative) repositioning of the catheter [23,40], while spontaneous resolution of scrotal migration was documented in three patients [3,37,49]. The precise mechanism underlying the spontaneous resolution of scrotal migration remains unclear; however, it has been hypothesized that factors such as gravitational repositioning, fluctuations in intra-abdominal pressure, and progressive fibrotic encapsulation may contribute to the gradual return of the distal catheter to its intended anatomical position [3]. These findings suggest that conservative management may be a viable option in carefully selected asymptomatic patients, particularly within the pediatric population, where increased tissue elasticity and ongoing anatomical development may promote spontaneous correction [56]. In particular, conservative management might be justified in cases without clinical signs of shunt malfunction, infection, or hydrocele formation, and where the catheter remains functionally positioned despite scrotal descent. The absence of progressive symptoms and stable neuroimaging findings during follow-up may further support a watchful waiting approach [57]. Nonetheless, such an approach would require vigilant clinical monitoring to ensure early detection of potential shunt dysfunction or other complications. Given the rarity of these occurrences, further studies are warranted to elucidate predictive factors for spontaneous regression and to establish evidence-based guidelines for non-operative management [23].
Limitations
One of the main limitations of this review is the relatively small number of included studies, the majority of which were case reports or single-center case series with limited sample sizes. This restricted the depth of analysis, introduced potential sources of bias, and significantly limited the generalizability of the findings. A meta-analysis was not performed, thereby reducing the ability to conduct a quantitative synthesis. As a result, interpretation of the findings relied more heavily on subjective judgment, the identification of consistent patterns across studies was hindered, and assessment of between-study heterogeneity was not feasible.
In addition, one case report [25] and one case series [24] were assessed as having low methodological quality according to the JBI Critical Appraisal Tools. Although these studies contributed relevant clinical observations, their methodological limitations may have introduced additional bias.
To address these limitations, future research should prioritize the design and implementation of high-quality retrospective cohort studies, randomized controlled trials, and prospective observational studies. Ideally, such studies should be conducted across multiple centers to improve the representativeness and robustness of the data. Furthermore, the adoption of standardized research protocols and consistent reporting of key clinical and demographic variables would facilitate more accurate cross-study comparisons and enable future meta-analyses.
6. Conclusions
This case report presents laparoscopic repositioning of the VPS into the peritoneal cavity, combined with closure of the processus vaginalis, as a safe and effective treatment strategy for managing scrotal migration of the VPS in pediatric patients. Further well-designed, multicenter studies are necessary to provide more comprehensive, generalizable, and unbiased evidence regarding this rare but clinically significant complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anwar F. Zhang K. Sun C. Pang M. Zhou W. Li H. He R. Liu X. Ming D. Hydrocephalus: An Update on Latest Progress in Pathophysiological and Therapeutic Research Biomed. Pharmacother.202418111770210.1016/j.biopha.2024.11770239581146 · doi ↗ · pubmed ↗
- 2Kahle K.T. Klinge P.M. Koschnitzky J.E. Kulkarni A.V. Mac Aulay N. Robinson S. Schiff S.J. Strahle J.M. Paediatric Hydrocephalus Nat. Rev. Dis. Primer 2024103510.1038/s 41572-024-00519-9PMC 1209126938755194 · doi ↗ · pubmed ↗
- 3Alkhudari A. Galal M. Wagley Z. Sabbah B.N. Houdane A. Aljabr A. A Case of Spontaneous Resolution of a Scrotal Ventriculoperitoneal Shunt Migration Radiol. Case Rep.2022173620362310.1016/j.radcr.2022.07.03935923335 PMC 9340143 · doi ↗ · pubmed ↗
- 4Ferras M. Mc Cauley N. Stead T. Ganti L. Desai B. Ventriculoperitoneal Shunts in the Emergency Department: A Review Cureus 202012 e 685710.7759/cureus.685732181092 PMC 7053664 · doi ↗ · pubmed ↗
- 5Dowlati E. Shashaty M. Carroll A.H. Pivazyan G. Briscoe J. Patel N. Shahjouie S. Anaizi A.N. Jackson P.G. Nair M.N. General Surgery Involvement with Ventriculoperitoneal Shunt Insertions Reduces Revision Rates Clin. Neurol. Neurosurg.202019910626310.1016/j.clineuro.2020.10626333059316 · doi ↗ · pubmed ↗
- 6BakalÜ. Poyraz A.K. Tartar T. Akdenizİ. Sürme M.B. Çelik S. SaraçM. A Rare Complication of Ventriculoperitoneal Shunt: Asymptomatic Small Bowel Perforation Istanb. Med. J.20192057157310.4274/imj.galenos.2019.65391 · doi ↗
- 7Lee B.S. Vadera S. Gonzalez-Martinez J.A. Rare Complication of Ventriculoperitoneal Shunt. Early Onset of Distal Catheter Migration into Scrotum in an Adult Male: Case Report and Literature Review Int. J. Surg. Case Rep.2015619820210.1016/j.ijscr.2014.09.032PMC 433495125553524 · doi ↗ · pubmed ↗
- 8Khoudir M. Harris L. Toescu S.M. Vaqas B. Scrotal Migration of a Ventriculoperitoneal Shunt in an Adult. A Case Report and Literature Review Brain Spine 2022210089810.1016/j.bas.2022.10089836248102 PMC 9562235 · doi ↗ · pubmed ↗