Topical Chlormethine Gel in the Treatment of Lymphomatoid Papulosis: A Case Report and Literature Review
Miriam Teoli, Martina Caviglia, Federica Rega, Luca Barbieri, Marco Ardigò, Victor Desmond Mandel

TL;DR
A 57-year-old man with a rare skin lymphoproliferative disorder achieved full recovery using chlormethine gel, suggesting it as a potential treatment option.
Contribution
Demonstrates the effectiveness of topical chlormethine gel in treating acral lymphomatoid papulosis, a rare skin condition.
Findings
The patient achieved complete remission and full joint recovery after three months of chlormethine gel treatment.
Six months post-treatment, the patient remained in remission with no recurrence.
The case suggests chlormethine gel could be a viable treatment option for acral lymphomatoid papulosis.
Abstract
Background: Lymphomatoid papulosis (LyP) is a primary cutaneous CD30-positive T-cell lymphoproliferative disorder presenting with self-healing erythematous papulonodular lesions that may ulcerate and scar. Treatment varies by lesion extent, location, and severity. Case Report: We describe a 57-year-old man with acral LyP successfully treated with chlormethine gel (CG). The patient experienced impaired second finger mobility for over 3 months due to an ulcerated nodular mass. After 3 months of CG treatment, complete remission, symptom resolution, and full joint recovery were achieved. Six months post-treatment, the patient remained in remission. Conclusions: This case underscores the effectiveness of CG in achieving sustained remission in acral LyP, suggesting its potential as a treatment option for this rare condition.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
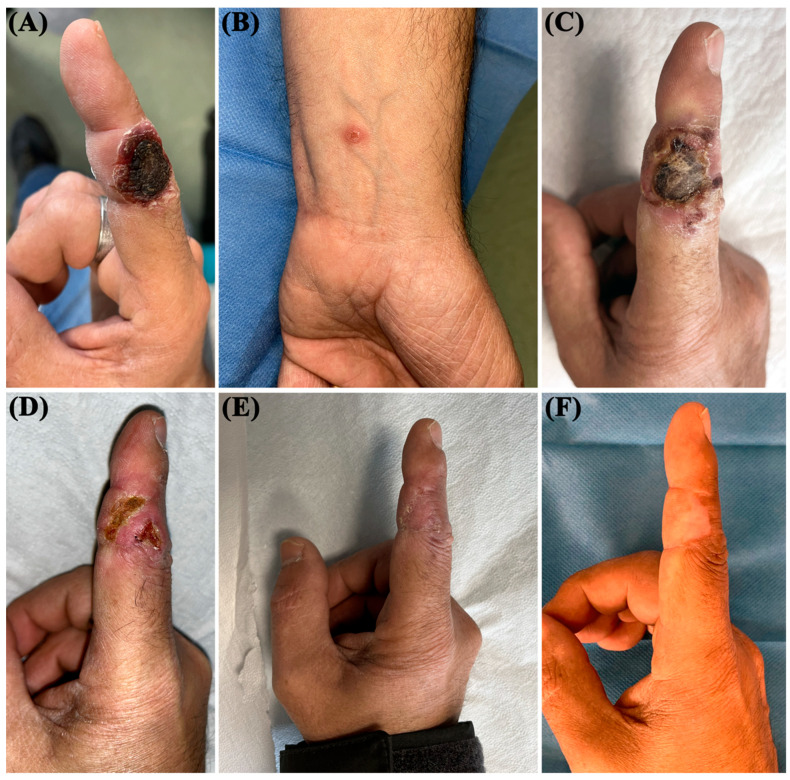 Figure 1
Figure 1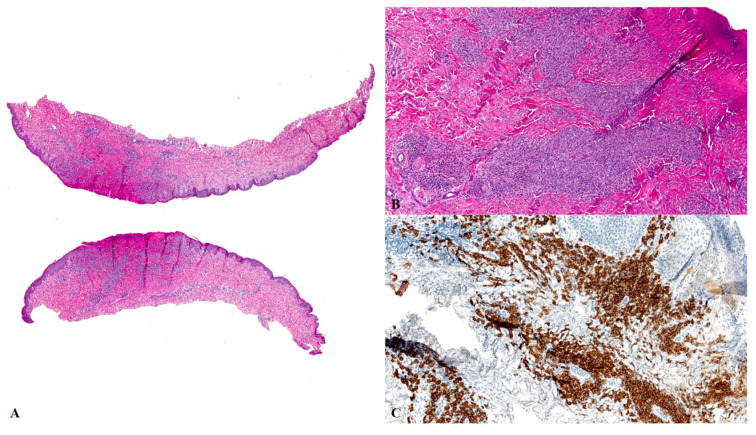 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Fungal Infections and Studies · Nail Diseases and Treatments
1. Introduction
Lymphomatoid papulosis (LyP) is a cutaneous CD30-positive T-cell lymphoproliferative disorder (CD30+ TLPD), a subcategory of cutaneous T-cell lymphoma that mostly has a non-aggressive course and accounts for about 15% of all cutaneous lymphomas [1]. Its etiology and pathogenetic mechanisms are currently unknown. The disease exhibits two peak frequencies: first, in children under 18 years of age, and second, in adults between the fourth and fifth decades of life [2]. The clinical spectrum of LyP includes self-healing erythematous papulonodular lesions that often become pustular, ulcerated, and resolve with scarring. These lesions can be single or multiple and commonly occur on the trunk and limbs [3]. Rare cases of segmental or localized presentations involving acral and facial sites have been described [4,5,6,7]. Acral LyP, in particular, is an uncommon variant that can lead to significant morbidity due to pain, ulceration, or impaired mobility. Its rarity and clinical impact underscore the importance of individualized management strategies.
LyP may be preceded, associated, or followed by other lymphatic neoplasms, with mycosis fungoides (MF) being the most commonly associated secondary lymphoma [8,9]. Treatment outcomes are unsatisfactory and may vary depending on the extent, location, and severity of the skin lesions. A ‘watchful waiting strategy’ approach can be considered for patients with a single or relatively few lesions. However, topical therapies such as corticosteroids or chlormethine gel may be preferred. In particular, chlormethine gel offers a non-steroidal, skin-directed approach with a long history of safe use in cutaneous lymphomas, and may be advantageous in acral locations where minimizing tissue atrophy and preserving function are priorities [7]. Cases with disseminated disease may benefit from phototherapy or methotrexate, which has been specifically recommended in treatment guidelines such as those by the Dutch Cutaneous Lymphoma Group [10]. Broader guidance for CD30+ lymphoproliferative disorders, including LyP, is also provided in the EORTC, ISCL, and USCLC consensus recommendations [11]. Alternative therapeutic approaches include antibiotics, antihistamines, oral steroids, or brentuximab, a monoclonal antibody targeting CD30 (Table 1) [2,3,4,5,6,7,8,9,10,11,12].
Herein, we report a rare case of LyP with exclusively acral localization treated with commercially available chlormethine gel (CG). Additionally, we provide a brief review of the related literature.
2. Case Report
A 57-year-old man, a painter by profession, was referred to our Porphyria and Rare Disease Unit in December 2022 for an evaluation of a painful lesion on the second finger of his right hand that had persisted for more than 3 months. He complained of impaired mobility of the finger joint, which prevented him from working. The patient had previously been evaluated at another center, where no specific diagnosis or treatment had been initiated. His family and medical history were unremarkable, and he was not taking any medications. A clinical examination revealed an ulcerative nodular mass measuring 2 × 1.5 cm, with well-defined and raised edges, located on the second finger of the right hand (Figure 1A). The lesion was covered by a strongly adherent eschar that was firm on palpation. A small (0.5 × 0.4 cm) erythematous papule was also observed on the left wrist (Figure 1B). We performed a complete routine laboratory investigation, including immunologic tests (immunoglobulins, rheumatoid factor, antinuclear factor, and organ-specific antibodies), and all values were within the normal range. To exclude systemic involvement, the patient also underwent an ultrasound examination of superficial lymph node sites, abdominal ultrasound, and a chest X-ray—all of which were unremarkable. After curettage (Figure 1C), an 8 mm punch biopsy was performed on the ulcerative nodular lesion of the second finger. A histopathologic analysis revealed a dense dermal lymphoid infiltrate composed of CD3+, CD4−, and CD8+ elements, along with clusters of CD30+ lymphomatoid cells (Figure 2). These features were suggestive of a type E LyP, characterized by the presence of angiotropism/angiodestruction with perivascular and intraluminal infiltrates of atypical cells, where T cells can be either CD4+ or CD8+. Additional proliferation markers such as Ki-67 were not deemed necessary, as the immunophenotype and T-cell receptor gene rearrangement analysis confirming monoclonality were sufficient to establish the diagnosis. A T-cell receptor gene rearrangement analysis showed monoclonality, and the histopathologic features were consistent with a diagnosis of LyP. Due to the painful symptoms and associated functional impairment, topical treatment with CG was prescribed. The patient applied a thin layer of CG to the lesion on the second finger every other day during the first week of treatment and then once daily in the evening, as recommended to reduce the risk of phototoxicity and enhance local tolerability. After approximately two weeks of CG application, the patient developed local irritative contact dermatitis (ICD), presenting with burning and itching sensations. Topical clobetasol propionate cream was initiated within a few days of symptom onset, and CG application was temporarily reduced. As corticosteroid treatment began shortly after the appearance of symptoms and was effective in relieving the reaction, the precise duration of the ICD could not be determined; this event did not recur. Once the irritation was resolved, the frequency of CG application was gradually increased, and the topical steroid was discontinued. One month later, a favorable response was observed (Figure 1D). A complete clinical remission of the lesions, with the resolution of painful symptoms and the fully functional recovery of the finger joint, was observed after 2 more months (Figure 1E). No serious adverse effects were reported during CG application, and the treatment was discontinued in March 2023. To maintain complete remission, methotrexate (7.5 mg per week) was prescribed in combination with folic acid (5 mg per week) following recommendations from the Dutch Cutaneous Lymphoma Group for the management of recurrent or symptomatic LyP [10]. Meanwhile, the erythematous papule observed on the left wrist resolved spontaneously. The patient has continued monthly follow-ups, including laboratory assessments of liver and kidney function as well as blood counts. At 6 months after the discontinuation of CG application, the patient remains in complete remission, maintained with methotrexate and folic acid.
3. Discussion
LyP shares many therapeutic options with other TLPDs, such as MF. However, no curative therapy is currently available. Guideline-based approaches emphasize treatment individualization according to lesion number, location, and severity. Methotrexate is supported as a first-line systemic option for widespread disease by the Dutch Cutaneous Lymphoma Group, while the EORTC/ISCL/USCLC consensus offers broader recommendations on management and clinical endpoints for CD30+ disorders [10,11]. Chlormethine gel was selected as monotherapy based on the localized nature of the lesions and the absence of systemic involvement. In line with the clinical review by Martinez-Cabriales et al. [7], topical monotherapy is an appropriate and effective first-line approach for patients with limited disease. The decision to avoid combination therapy with corticosteroids or phototherapy was guided by the desire to minimize the treatment burden, reduce potential cumulative side effects, and achieve a targeted, skin-directed intervention in a functionally sensitive area. The patient’s complete remission and functional recovery without the need for adjunctive treatments support the adequacy of monotherapy in this context [10,11]. Chlormethine, also known as mechlorethamine, is a nitrogen mustard classified as an alkylating agent. It binds to the N7 nitrogen of the base guanine in DNA, crosslinks two DNA strands, and inhibits rapidly proliferating cells, thereby preventing cell duplication [13]. CG (chlormethine 0.016% w/w, equivalent to 0.02% chlormethine hydrochloride) was approved by the US Food and Drug Administration in 2013 for treating stage IA and IB MF in patients who had previously received skin-directed therapies. In contrast, the European Medicines Agency approved its use for treating adult patients with MF in 2017 [13]. CG can be used as a monotherapy, in combination with systemic therapy, and as maintenance treatment [13,14]. Although the CG label recommends daily application, the frequency can be reduced to mitigate skin reactions.
In our case, we followed the same dosing schedule used for the MF treatment, achieving rapid and complete remission. Furthermore, the patient experienced a rapid and complete recovery of the finger joint functionality. The only side effect observed was moderate ICD, which is the most common skin reaction associated with CG therapy. However, ICD was effectively controlled with topical steroid use, improving the tolerability of CG, as reported in real-life experiences with MF treatment [14]. The long-term effects of CG have not been evaluated because of the short follow-up period available. Recently, Dege et al. described the use of CG in an 80-year-old patient with coexisting MF and LyP, observing the resolution of LyP papules after the localized application of the gel, which had been initiated primarily for MF lesions in adjacent areas [15]. Although their case provides relevant clinical insight into chlormethine use in LyP, it involved mixed disease and treatment not specifically tailored to LyP from the outset. In contrast, our report presents the first case of exclusive acral LyP successfully treated with chlormethine gel as monotherapy, initiated specifically to target LyP lesions and independent of concurrent MF. Additional cases support the use of topical alkylating agents for LyP. Shang et al. reported successful management of regional LyP with nitrogen mustard solution combined with interferon-alpha-2b [16]. Also, the association between LyP and other TLPDs is well known. Trager et al. described 10 patients with MF who developed LyP after experiencing an important inflammation during nitrogen mustard treatment [17]. The role of proliferation signals as chronic drug-induced inflammation has been hypothesized, but the triggering event leading to proliferation remains unclear [7]. Therefore, future prospective studies are warranted to evaluate the potential long-term side effects of CG and to investigate any possible correlation between CG-induced local inflammation and cutaneous T-cell lymphoma. The present case is limited by its single-patient design and a relatively short follow-up duration (6 months), which does not allow for conclusions about long-term safety or recurrence. Broader clinical experience and longer-term data are needed to confirm the durability of remission and establish the optimal role of CG in LyP management.
4. Conclusions
Our case highlights the importance of personalized treatment in minimizing the disease severity and achieving early complete remission. CG has proven to be a safe, fast-acting, easy-to-apply drug with excellent cosmetic results in LyP. Therefore, CG should be considered a viable therapeutic option for managing LyP, particularly in localized presentations. However, further studies are needed to validate these findings, assess long-term outcomes, and better define its role in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wiznia L.E. Cohen J.M. Beasley J.M. Meehan S.A. Latkowski J.M. Lymphomatoid papulosis Dermatol. Online J.20182413030/qt 4xt 046c 910.5070/D 3241204244330677799 · doi ↗ · pubmed ↗
- 2Nowicka D. Mertowska P. Mertowski S. Hymos A. Forma A. Michalski A. Morawska I. Hrynkiewicz R. Niedźwiedzka-Rystwej P. Grywalska E. Etiopathogenesis, diagnosis, and treatment strategies for lymphomatoid papulosis with particular emphasis on the role of the immune system Cells 202211369710.3390/cells 1122369736429125 PMC 9688547 · doi ↗ · pubmed ↗
- 3Fricke T. Kempf W. Schön M.P. Mitteldorf C. Histologic and immunohistochemical patterns in lymphomatoid papulosis: A systematic review of published cases Dermatopathology 202512610.3390/dermatopathology 1201000639982354 PMC 11861998 · doi ↗ · pubmed ↗
- 4Dalle S. Balme B. Thomas L. Lymphomatoid papulosis localized to the face Dermatol. Online J.200612910.5070/D 35DS 430MG 16638423 · doi ↗ · pubmed ↗
- 5Yancovitz M. Walters R.F. Kamino H. Brown L.H. Acral lymphomatoid papulosis J. Am. Acad. Dermatol.20106253053110.1016/j.jaad.2009.02.02520159331 · doi ↗ · pubmed ↗
- 6Hsu Y.J. Su L.H. Hsu Y.L. Tsai T.H. Hsiao C.H. Localized lymphomatoid papulosis J. Am. Acad. Dermatol.20106235335610.1016/j.jaad.2009.01.03420115961 · doi ↗ · pubmed ↗
- 7Martinez-Cabriales S.A. Walsh S. Sade S. Shear N.H. Lymphomatoid papulosis: An update and review J. Eur. Acad. Dermatol. Venereol.202034597310.1111/jdv.1593131494989 · doi ↗ · pubmed ↗
- 8Bekkenk M.W. Geelen F.A. van Voorst Vader P.C. Heule F. Geerts M.L. van Vloten W.A. Meijer C.J. Willemze R. Primary and secondary cutaneous CD 30+ lymphoproliferative disorders: A report from the Dutch Cutaneous Lymphoma Group on the long-term follow-up data of 219 patients and guidelines for diagnosis and treatment Blood 200095365310.1182/blood.V 95.12.365310845893 · doi ↗ · pubmed ↗