Comparative Outcomes of Intra-Aortic Balloon Pump Versus Percutaneous Left Ventricular Assist Device in High-Risk Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis
Dhiran Sivasubramanian, Virushnee Senthilkumar, Nithish Nanda Palanisamy, Rashi Bilgaiyan, Smrti Aravind, Sri Drishaal Kumar, Aishwarya Balasubramanian, Sathwik Sanil, Karthick Balasubramanian, Dharssini Kamaladasan, Hashwin Pilathodan, Kiruba Shankar

TL;DR
This study compares two heart support devices during high-risk heart procedures and finds one device is better at reducing early death and heart failure risks.
Contribution
The study provides a meta-analysis comparing IABP and PLVAD outcomes in HR-PCI without cardiogenic shock.
Findings
PLVAD use was associated with lower early mortality compared to IABP.
PLVAD reduced the risk of cardiogenic shock compared to IABP.
No significant differences were found in bleeding, kidney injury, or stroke rates between the devices.
Abstract
Background/Objectives: High-risk percutaneous coronary interventions (HR-PCIs) often require mechanical circulatory support (MCS) to maintain hemodynamic stability. Intra-aortic balloon pump (IABP) and percutaneous left ventricular assist device (PLVAD) are two commonly used MCS devices that differ in their mechanisms. We aimed to evaluate and compare the clinical outcomes associated with IABP and PLVAD use in HR-PCIs without cardiogenic shock. Methods: We conducted a search of PubMed, Scopus, Cochrane, Mendeley, Web of Science, and Embase to identify relevant randomized controlled trials and cohort studies, and we included 13 studies for the systematic review and meta-analysis. The primary goal was to define the difference in early mortality (in-hospital and 30-day mortality), major bleeding, and major adverse cardiovascular event (MACE) components (cardiogenic shock, acute kidney…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
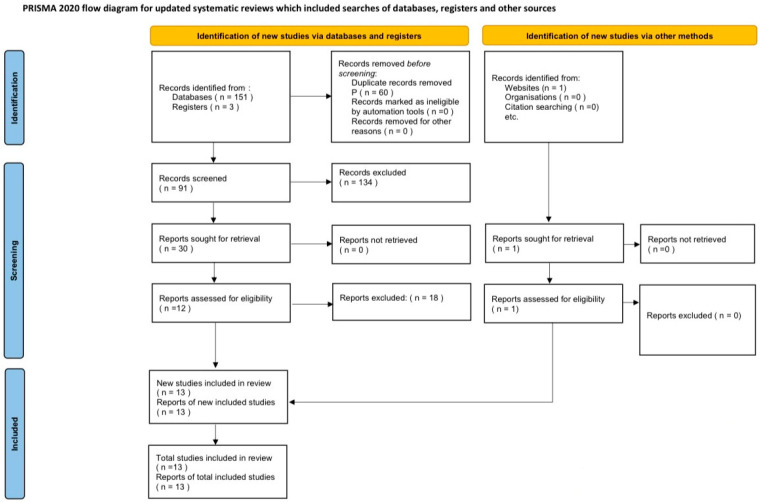 Figure 1
Figure 1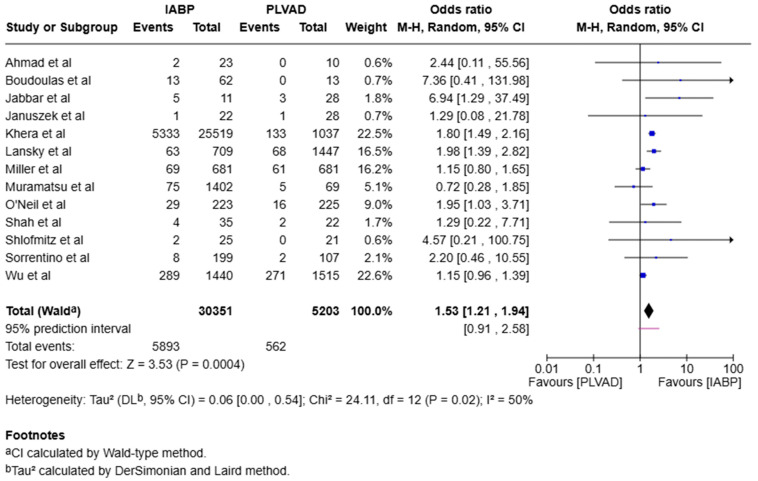 Figure 2
Figure 2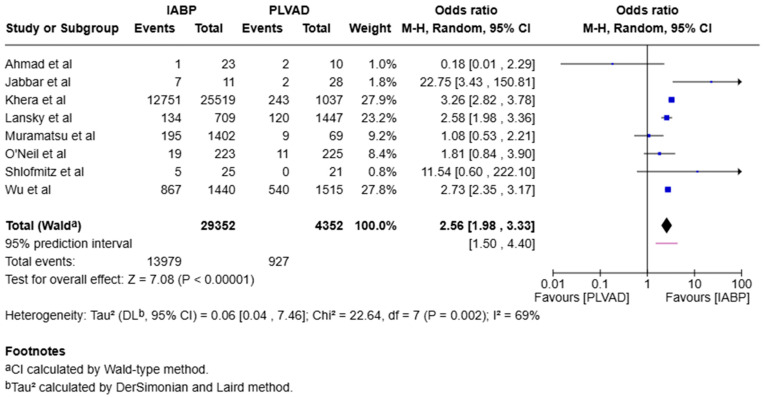 Figure 3
Figure 3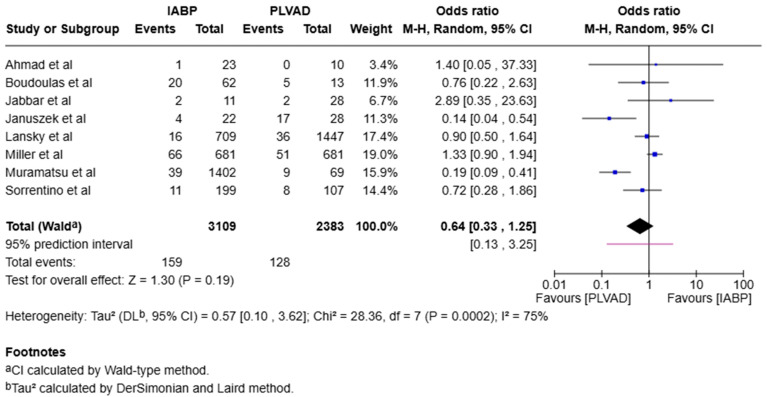 Figure 4
Figure 4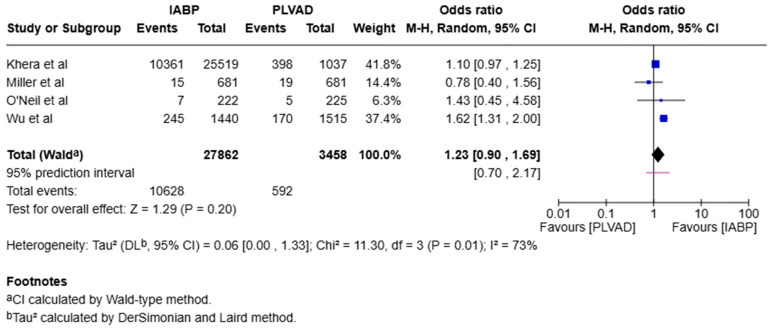 Figure 5
Figure 5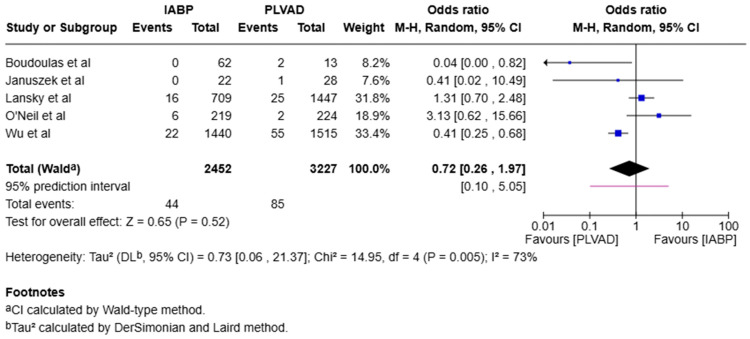 Figure 6
Figure 6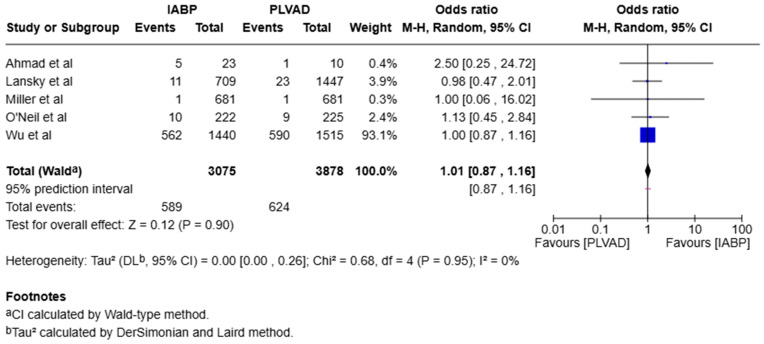 Figure 7
Figure 7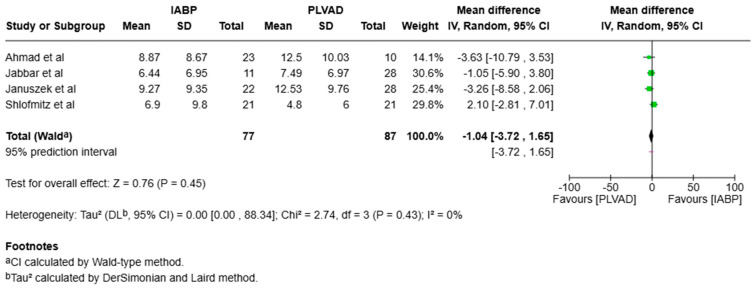 Figure 8
Figure 8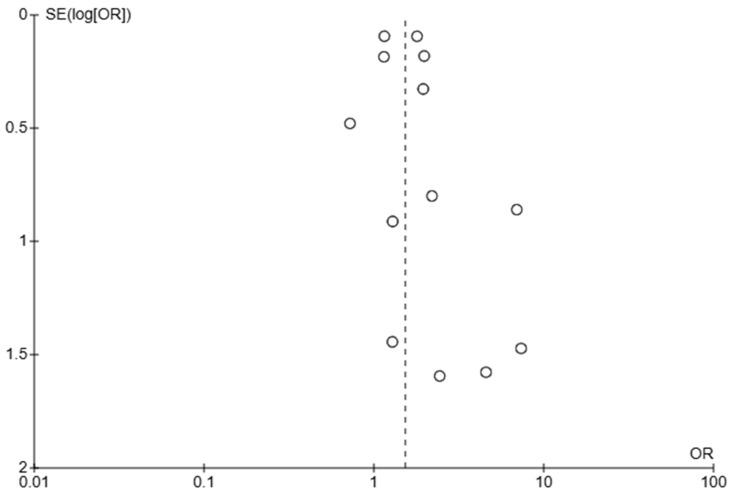 Figure 9
Figure 9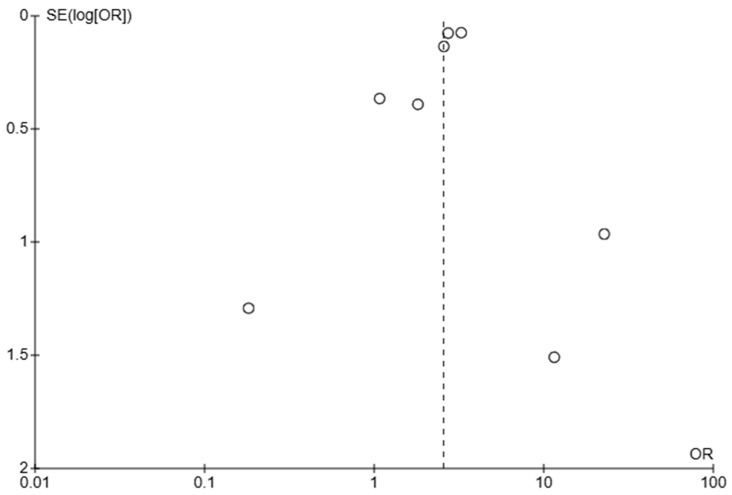 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair
1. Introduction
High-risk percutaneous coronary interventions (HR-PCIs) are performed in patients who present with significant clinical challenges like advanced age, diabetes mellitus, multivessel disease, unprotected left main coronary artery involvement, complex coronary anatomy, and severely impaired left ventricular function, which increase their periprocedural risk. These procedures are complicated by transient interruptions of coronary blood flow caused by balloon inflation, contrast dye injections, guidewire passage, and stent manipulation, which can result in the acute impairment of cardiac function [1,2]. Mechanical circulatory support (MCS) devices, such as percutaneous left ventricular assist devices (PLVADs) and intra-aortic balloon pump (IABP), are employed to enhance hemodynamic stability by ensuring adequate systemic and coronary perfusion during these procedures [2,3].
Intra-aortic balloon pump (IABP) has been a mainstay device in providing such support; however, in recent times, IABP’s limited augmentation of cardiac output has promoted the growth of the use of PLVAD, which includes Impella and Tandem Heart [1,4].
Several studies and a randomized controlled trial (RCT) have compared IABP and PLVAD use in HR-PCI, but the findings remain inconsistent. Previous meta-analyses comparing IABP and PLVAD included both HR-PCIs and shock populations, which may confound the interpretation of outcomes specific to elective HR-PCIs [4,5,6]. Although there is only one RCT to date [7], several cohort studies have emerged in recent years. In this systematic review and meta-analysis, we aimed to strictly compare the outcomes of IABP and PLVAD in HR-PCIs without cardiogenic shock to provide more targeted clinical insights.
2. Methods
2.1. Search Strategy
We conducted a systematic search of the PubMed, Scopus, Cochrane, Mendeley, Web of Science, and Embase databases to identify relevant RCTs and cohort studies with patients undergoing HR-PCI under MCS with IABP or PLVAD up to June 2025. The search was limited to English-language articles. The following search terms were included in various combinations: “intra-aortic balloon pump”, “percutaneous left ventricular assist device”, “Impella”, “Tandem Heart”, “high-risk percutaneous coronary intervention”, “protected percutaneous coronary intervention”, “randomized”, and “studies”. The search strategy was performed with adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Figure 1) [8,9]. Studies using the same patient databases were carefully excluded to prevent data overlap. Two independent authors (DS and VS) reviewed the search results separately to select the studies based on inclusion and exclusion criteria. Reference lists of the included studies were reviewed for any missing relevant studies. Disagreements were resolved by a third and fourth reviewer (NNP and RB). This review was not registered in any registry.
2.2. Inclusion Criteria
The inclusion criteria were cohort studies or RCTs with at least 10 patients undergoing HR-PCI with hemodynamic support that compared the differences based on whether the patients had PLVAD or IABP and reported one or all of the following outcomes: early mortality (in-hospital and 30-day mortality) and major cardiovascular adverse event (MACE) components such as cardiogenic shock, major bleeding, acute kidney injury (AKI), arrhythmia, and stroke/transient ischemic attack (TIA). Only adult patients >18 years old were included. Abstracts from major journals were included if they provided the desired results.
2.3. Exclusion Criteria
Non-English literature, systematic reviews, meta-analysis, narrative reviews, case reports/series, editorials, study protocols, commentaries, editorial letters, and studies that report the outcomes for only one intervention without the other were excluded. Studies with patients aged < 18 years were also excluded.
2.4. Data Extraction and Quality Assessment
Six independent investigators were tasked with data extraction from the included studies, and a thorough review of the data was performed. For each study, the data on the number of events and the total number were abstracted.
The extracted data included primary outcomes of interest, early mortality (including 30-day mortality and in-hospital mortality), peri- and post-procedural cardiogenic shock, major bleeding events, new arrhythmias, the occurrence of AKI and stroke/TIA, along with mean length of stay in the hospital.
Using the Newcastle–Ottawa scale (NOS) risk-of-bias assessment instrument, a total of 13 studies from the initial 155 records that met the inclusion criteria were assessed. After two impartial assessors evaluated the potential for bias, a final table was created based on their consensus (Table 1 and Table 2).
2.5. Statistical Analysis
The Cochrane Collaboration and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines were fully adhered to in this meta-analysis [22]. We used the Cochrane Collaboration’s “Review Manager” software version 5.4.1 (The Cochrane Collaboration, London, UK) for data analysis. We employed the Mantel–Haenszel random-effects model to estimate the odds ratios (ORs) and the associated 95% confidence intervals (CIs) for binary outcomes. The inverse variance method was also utilized to determine the weighted mean difference (MD) for continuous outcomes.
Forest plots were created for the graphical representation of the clinical outcomes. Heterogeneity between studies, defined as variation among the results of individual studies beyond that expected from chance, was evaluated with the I^2^ statistic. Interpretation for I^2^: 50%, low heterogeneity; 50–75%, moderate heterogeneity; and >75%, high heterogeneity. Publication bias was evaluated through visual inspection of funnel plots for asymmetry in Review Manager.
3. Results
A total of 13 studies (1 RCT and 12 cohort studies) met our criteria and were included in this study from a total of 155 records that were initially identified from the databases (Figure 1). A total of 35,554 patients were included in this analysis conducted between 2014 and 2025, with 30,351 patients receiving IABP and 5203 receiving PLVAD. The study characteristics are presented in Table 3. The study by Al-Khadra et al. [23] using the National Inpatient Sampling (NIS) database met the inclusion criteria but was carefully excluded because there was a potential overlap of patients as they used the same database as Khera et al. [14].
3.1. Mortality
Early mortality (in-hospital and 30-day mortality) was significantly higher in the IABP group when compared to the PLVAD group (OR = 1.53, 95% CI [1.21, 1.94], p < 0.001, I^2^ = 50%) (Figure 2).
3.2. Subgroup Analysis
We observed a significantly higher incidence of cardiogenic shock in the IABP group compared to the PLVAD group (OR = 2.56, 95% CI [1.98, 3.33], p < 0.00001, I^2^ = 69%) (Figure 3). We also observed no significant difference in major bleeding (OR = 0.64, 95% CI [0.33, 1.25], p = 0.19, I^2^ = 75%) (Figure 4), stroke/TIA (OR = 1.23, 95% CI [0.90, 1.69], p = 0.20, I^2^ = 73%) (Figure 5), arrhythmia (OR = 0.72, 95% CI [0.26, 1.97], p = 0.52, I^2^ = 73%) (Figure 6), AKI (OR = 1.01, 95% CI [0.87, 1.16], p = 0.90, I^2^ = 0%) (Figure 7), or length of stay (MD = −1.04, 95% CI [−3.72, 1.65], p = 0.45, I^2^ = 0%) (Figure 8) between both of the groups.
3.3. Heterogeneity
Early mortality demonstrated low heterogeneity across the studies (I^2^ = 50%), indicating relatively consistent findings. The cardiogenic shock, major bleeding, arrhythmia, and stroke/TIA outcomes showed moderate heterogeneity (I^2^ = 69%, 75%, 73%, and 73%, respectively), suggesting some variability in the effect estimates. AKI and length of hospital stay had no heterogeneity (I^2^ = 0%), reflecting highly consistent results among the studies.
3.4. Assessment of Publication Bias
The funnel plot (Figure 9) evaluating early mortality suggests some degree of publication bias, evidenced by the asymmetry. Larger studies appear more consistent and tend to cluster at OR = 1–2, suggesting less extreme estimates and higher reliability, while smaller studies vary widely, which is expected due to higher random error in smaller studies.
The funnel plot (Figure 10) evaluating cardiogenic shock suggests high heterogeneity, as seen from the wide range of ORs (from <0.1 to >10). The asymmetry also suggests the potential for publication bias, especially against small studies showing a benefit (OR < 1).
4. Discussion
During HR-PCI, patients are subject to increased risk of hemodynamic collapse; to mitigate these risks, MCS devices are used to maintain adequate systemic and coronary perfusion during the procedure [1].
As of now, there are no clear criteria to identify high-risk PCI candidates. The Society for Cardiovascular Angiography & Interventions (SCAI) specifically highlights that those patients with severely impaired ejection fraction (≤35%), unprotected left main coronary artery, or complex multivessel disease undergoing PCI are considered to be at high risk of hemodynamic compromise and may benefit from MCS. The SCAI also notes that additional factors, such as comorbidities, advanced age, anticipated procedural complexity (e.g., atherectomy), and extent of myocardium at risk, should be integrated into the risk assessment for MCS use [24].
The commonly used MCS devices in HR-PCI are IABP and PLVAD. PLVAD comprises two main devices, Impella 2.5 and Tandem Heart [2]. Both groups of devices have distinct mechanisms of action, and a comparison of their effectiveness in HR-PCI is much needed.
4.1. Outcomes
4.1.1. Early Mortality
Our analysis reported lower early mortality with PLVAD when compared to IABP. This is in alignment with the findings of a large propensity-adjusted analysis conducted by Lansky et al. [15] of 2156 patients undergoing HR-PCI, which showed that Impella was associated with improved in-hospital survival, lower myocardial infarction, and cardiogenic shock events compared to IABP, while other MACEs were similar in both groups. The only RCT that compared Impella and IABP in HR-PCI is the PROTECT II trial [7], which enrolled 448 patients based on anatomical and clinical criteria, and they showed no significant difference in 30-day mortality between the groups. However, Impella showed a potential benefit over IABP in terms of 90-day mortality. Additionally, there was a non-significant trend towards fewer MACEs with Impella.
4.1.2. Cardiogenic Shock
A significant increase in the incidence of cardiogenic shock was noted in our study while using IABP compared to PLVAD. This can perhaps be attributed to the difference in the mechanism of the two devices. The IABP works by inflating during diastole to augment coronary perfusion and deflating just before systole to reduce afterload and thereby moderately increasing the cardiac output and improving coronary perfusion. Impella actively unloads the left ventricle (LV) by aspirating blood from the LV and expelling it into the aorta, while Tandem Heart withdraws blood from the left atrium and returns it to the femoral artery, bypassing the LV, thereby increasing the cardiac output and lowering the myocardial oxygen demand [25].
4.1.3. Stroke
Our analysis showed that the occurrence of stroke was similar in the Impella and PLVAD groups. Stroke incidence is generally higher with PLVAD, including Impella and Tandem Heart, compared to IABP in high-risk percutaneous procedures, according to previous studies. In cardiogenic shock, stroke rates range from 4 to 8% with PLVAD versus 3 to 4% with IABP [26,27,28]. In HR-PCI without shock, the absolute stroke rates are low, with no significant difference between the devices [15,29]. These trends are consistent across large observational studies and meta-analyses [15,26,29].
4.1.4. Major Bleeding
Our analysis showed that the occurrence of major bleeding was similar in the Impella and PLVAD groups. According to previous studies, major bleeding is significantly more common with PLVAD than with IABP in HR-PCI. Other meta-analyses report a 2- to 3-fold increased risk with PLVAD (RR 2.35–2.85) [26,30]. During MCS use in cardiogenic shock, the in-hospital major bleeding rates are 31.3% with PLVAD versus 16.0% with IABP [31], with similar trends in real-world data showing higher hematologic and overall complications with PLVADs [26,28]. The bleeding rates generally range from 11 to 19% for IABP and 19 to 31% for PLVAD in HR-PCI or shock [26,32,33,34].
4.1.5. Acute Kidney Injury
AKI is a major risk after high-risk PCI, especially in patients with low LVEF or chronic kidney disease (CKD). Our study does not show a significant difference in the occurrence of AKI between the two groups. This, however, is in contrast to Flaherty MP et al., who found that the use of PLVAD (Impella) significantly reduces AKI risk and lowers dialysis rates, likely by improving renal perfusion [35]. In contrast, IABP use increases AKI risk, likely due to insufficient hemodynamic support [31,36].
4.1.6. Arrhythmia
We found no significant difference in the incidence of arrhythmia between the two groups. A previous meta-analysis pooled from RCTs comparing IABP and PLVADs in high-risk PCI showed similar results [29]; these findings are consistent across all of the available randomized data and observational studies, such as the large propensity-weighted retrospective analysis of 2879 patients by Miller et al. [21].
4.1.7. Length of Stay and Cost Effectiveness
The length of hospital stay is similar between the two groups. Multicenter retrospective and prospective studies have not shown any significant differences [10,12,13,18].
PLVADs are significantly less cost-effective than IABP in this setting. Contemporary claims-based analyses by Miller et al. showed that the mean total costs for the index admission are substantially higher with PLVADs (e.g., Impella) compared to IABP (approximately USD 96,700 vs. USD 71,900; p < 0.001), and this cost difference persists at 30 days post-procedure [21].
4.2. Strengths and Limitations
Our study results are different from previous meta-analyses [4,5,6]; the exclusive focus on high-risk PCI without cardiogenic shock addresses a critical gap. Previous meta-analyses have pooled these distinct populations, despite their pathophysiology, risk profiles, and expected outcomes. By deliberately excluding studies involving cardiogenic shock, the current work provides a more precise estimate of the comparative effectiveness and safety of IABP vs. PLVAD specifically in high-risk PCI settings, where the risk–benefit calculus may differ substantially from that in shock. It offers a focused, up-to-date synthesis of evidence for device selection in high-risk PCI, unconfounded by the inclusion of cardiogenic shock populations. This meta-analysis further incorporates the more recent registry data up to 2025, which enhances the relevance of the findings compared to earlier meta-analyses that relied on older or less comprehensive datasets. We showed a significantly higher early mortality and cardiogenic shock in IABP compared to PLVAD. We also included the largest sample size of 35,554 patients compared to other analyses. Although one of the meta-analyses that reported PLVAD could be associated with a higher occurrence of adverse events such as bleeding and AKI [6], we did not find any significant difference in MACEs other than cardiogenic shock between the groups.
This systematic review and meta-analysis has several limitations.
First, there was significant heterogeneity among the included studies, particularly in secondary outcomes such as major bleeding, stroke/TIA, cardiogenic shock, and arrhythmia, which may reflect differences in the study design, including randomized controlled trials versus observational studies, sample size, and follow-up duration, resulting in variable risk of bias and event ascertainment, directly impacting the outcome estimates and their variability across studies.
The patient selection criteria are inconsistent, with studies enrolling populations that differ in age, comorbidities, baseline left ventricular function, and procedural risk, all of which influence complication rates. For example, some studies include patients with more advanced coronary disease or higher bleeding risk, leading to divergent rates of major bleeding and arrhythmia [26,29].
Procedural techniques and operator skill also vary widely. Device selection (e.g., Impella vs. Tandem Heart), the vascular access approach, anticoagulation protocols, and periprocedural management are not standardized, and operator and center experience with newer devices can affect complication rates, particularly for bleeding and vascular events [6,29,37].
Definitions of adverse events such as major bleeding, stroke, and arrhythmia are not uniform across studies, with some using clinical criteria and others relying on administrative or registry data, further increasing heterogeneity [29,37]. Furthermore, the funnel plots show asymmetry towards IABP, suggesting that studies favoring PLVAD or higher mortality or cardiogenic shock in IABP may be more likely to be published.
Second, the included studies also varied in their reporting of mortality outcomes; some reported in-hospital mortality, while others reported 30-day mortality. To account for this inconsistency, we grouped these endpoints under the broader category of early mortality, which may obscure important differences. In-hospital mortality is more likely to reflect procedural and immediate post-procedural complications, whereas 30-day mortality includes later events such as subacute heart failure or non-cardiac causes. Prior studies have shown that the risk of death is highest in the first week following PCI and declines thereafter, with cardiac causes predominating early and non-cardiac causes increasing over time [38,39]. As a result, combining these endpoints may dilute the impact of device-related procedural complications on the observed outcomes.
Third, the majority of included studies were observational cohort studies rather than randomized controlled trials. As a result, the findings may be subject to inherent biases, including confounding by indication. For example, clinicians may preferentially select PLVADs, particularly Impella, for patients perceived to be at lower risk or with specific anatomical considerations, while IABP is reserved for sicker patients due to easier insertion and familiarity. This selection bias can skew outcome comparisons. While few observational studies have statistical adjustments, such as propensity score matching and multivariate regression to address baseline imbalances [15,21,23], residual confounding from unmeasured or unknown variables cannot be excluded. The analysis by Agoritas et al. explicitly notes that even with advanced adjustment methods, non-randomized studies are inherently susceptible to selection and referral bias, and only randomization can fully balance both known and unknown confounders. This limitation should temper the interpretation of any observed associations, particularly regarding device selection and outcomes [40].
Fourth, the studies do not specify the exact distinction between intra-procedural and post-procedural cardiogenic shock, so we could not analyze these separately. Additionally, there are no large-scale studies or randomized controlled trials that specifically differentiate between intra-procedural and post-procedural cardiogenic shock in patients undergoing HR-PCI when comparing IABP and PLVAD. The guidelines from the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography & Interventions also do not address this distinction, reflecting the lack of granular data in the literature [41,42]. This limitation affects the interpretation of device efficacy and safety, as intra-procedural shock may be more directly related to procedural complications and device performance, whereas post-procedural shock may reflect broader patient comorbidities or delayed complications. Without this distinction, attributing outcomes to device choice versus patient or procedural factors remains challenging.
Fifth, the lack of granular data regarding device type and procedural details limited our ability to perform device-specific subgroup analyses. While most PLVAD usage likely involved Impella 2.5, the exact distribution between Impella 2.5, Impella 5.0, and Tandem Heart devices were not uniformly reported. The Tandem Heart requires transseptal puncture, increasing procedural complexity and risk, but offers greater support than the Impella 2.5. The Impella 5.0 is comparable to Tandem Heart in terms of support. Differences in the flow capacity, mechanism, complication profiles, and access requirements between these devices could impact the outcomes, and these could not be analyzed separately in our study. This limitation is particularly relevant because prior analyses have shown that Impella and Tandem Heart may have different rates of major bleeding and short-term mortality in the HR-PCI population. Therefore, the results should be interpreted with caution, and the generalizability of the findings to specific devices or clinical scenarios is limited [6,29,43].
Lastly, the protocol was not prospectively registered in any registry (e.g., PROSPERO), which may introduce concerns regarding transparency and the potential for selective reporting.
4.3. Future Directions
It is important to note that Impella 2.5 is the most used form of commercially available PLVAD, which has a flow rate of 2.5 L/min, which was the device used in the PROTECT II trial. In contrast, Impella 5 provides more robust support with a flow rate of 5 L/min but requires a surgical cutdown of the femoral or axillary artery, similar to Tandem Heart, which limits its practicality in the clinical setting [41]. A study by Kovacic et al. [25] compared Tandem Heart and Impella 2.5 in 68 patients who underwent HR-PCI using either device, and they found that there was no difference in the short- or long-term clinical outcomes between the two groups. Large-scale multicenter RCTs are needed to clarify whether there is a difference between Impella 2.5 and Impella 5 or between these and Tandem Heart.
Additionally, the findings from the PRAISE registry show that the 1-year outcomes between STEMI (ST-elevated myocardial infarction) and NSTEMI (non-ST-elevated myocardial infarction) are comparable once adjusted for comorbidities and revascularization completeness [44]. This underscores the need to individualize MCS decisions based on patient profiles rather than MI type alone.
Our analysis exclusively focuses on short-term outcomes, such as in-hospital and 30-day mortality. While these endpoints provide valuable insights into early procedural risk, they do not capture the full clinical trajectory following HR-PCI. Future studies should incorporate long-term outcomes such as 6- or 12-month mortality and rehospitalization to better assess the sustained effectiveness of PLVADs over IABP in HR- PCI. Current evidence is limited to short-term endpoints, and standardized long-term follow-up is needed to guide clinical decision-making.
5. Conclusions
PLVAD use in HR-PCI was associated with lower early mortality and cardiogenic shock compared to IABP, with no significant difference in other adverse events and length of stay. While these findings suggest a potential clinical benefit of PLVADs, this must be weighed against their significantly higher cost. Moreover, as these results are derived predominantly from observational data, they should be interpreted with caution due to the potential for confounding by indication. Further, randomized controlled trials are needed to confirm these results and guide device selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bass T.A. High-Risk Percutaneous Coronary Interventions in Modern Day Clinical Practice: Current Concepts and Challenges Circ. Cardiovasc. Interv.20158 e 00340510.1161/CIRCINTERVENTIONS.115.00340526628592 · doi ↗ · pubmed ↗
- 2Simonton C. Thompson C. Wollmuth J.R. Morris D.L. Dahle T.G. The Role of Hemodynamic Support in High-risk Percutaneous Coronary Intervention US Cardiol. Rev.202014 e 1310.15420/usc.2020.18PMC 1166476039720455 · doi ↗ · pubmed ↗
- 3Kahaly O. Boudoulas K.D. Percutaneous left ventricular assist device in high risk percutaneous coronary intervention J. Thorac. Dis.2016829810.21037/jtd.2016.01.7727076921 PMC 4805787 · doi ↗ · pubmed ↗
- 4Kuno T. Takagi H. Ando T. Kodaira M. Numasawa Y. Fox J. Bangalore S. Safety and efficacy of mechanical circulatory support with Impella or intra-aortic balloon pump for high-risk percutaneous coronary intervention and/or cardiogenic shock: Insights from a network meta-analysis of randomized trials Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv.202197 E 636E 64510.1002/ccd.2923632894797 · doi ↗ · pubmed ↗
- 5Hu F.B. Cui L.Q. Percutaneous left ventricular assist device vs. intra-aortic balloon pump in patients with severe left ventricular dysfunction undergoing cardiovascular intervention: A meta-analysis Chronic Dis. Transl. Med.2018426026710.1016/j.cdtm.2017.11.00230603744 PMC 6308918 · doi ↗ · pubmed ↗
- 6Rios S.A. Bravo C.A. Weinreich M. Olmedo W. Villablanca P. Villela M.A. Ramakrishna H. Hirji S. Robles O.A. Mahato P. Meta-Analysis and Trial Sequential Analysis Comparing Percutaneous Ventricular Assist Devices Versus Intra-Aortic Balloon Pump During High-Risk Percutaneous Coronary Intervention or Cardiogenic Shock Am. J. Cardiol.20181221330133810.1016/j.amjcard.2018.07.01130146099 · doi ↗ · pubmed ↗
- 7O’Neill W.W. Kleiman N.S. Moses J. Henriques J.P. Dixon S. Massaro J. Palacios I. Maini B. Mulukutla S. Dzavík V. A prospective, randomized clinical trial of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoing high-risk percutaneous coronary intervention: The PROTECT II study Circulation 20121261717172710.1161/CIRCULATIONAHA.112.09819422935569 · doi ↗ · pubmed ↗
- 8Liberati A. Altman D.G. Tetzlaff J. Mulrow C. Gøtzsche P.C. Ioannidis J.P. Clarke M. Devereaux P.J. Kleijnen J. Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration Ann. Intern. Med.2009151 W 65W 9410.7326/0003-4819-151-4-200908180-0013619622512 · doi ↗ · pubmed ↗