Pellucid Marginal Degeneration: A Comprehensive Review of Pathophysiology, Diagnosis, and Management Strategies
Michael Tsatsos, Konstantina Koulotsiou, Ioannis Giachos, Ioannis Tsinopoulos, Nikolaos Ziakas

TL;DR
This paper reviews Pellucid Marginal Degeneration, a rare corneal disorder, focusing on its causes, diagnosis, and treatment options to improve patient outcomes.
Contribution
The paper provides a comprehensive review of PMD, emphasizing recent advancements in diagnostic techniques and treatment strategies.
Findings
PMD is characterized by crescent-shaped corneal thinning and irregular astigmatism.
Surgical interventions like CXL, ICRS, and toric IOLs show promise for advanced PMD.
Early diagnosis using corneal tomography improves treatment outcomes.
Abstract
Purpose: Pellucid Marginal Degeneration (PMD) is a rare ectatic corneal disorder characterized by inferior peripheral thinning and significant irregular astigmatism. Despite its clinical similarities to keratoconus, PMD presents unique diagnostic and therapeutic challenges. This review aims to provide a comprehensive update on the pathophysiology, clinical features, diagnostic approaches, and management strategies for PMD, emphasizing the latest advancements in treatment options. Methods: A systematic literature search was performed in MEDLINE (via PubMed), Google Scholar, and Scopus up to February 2025 using the terms: “pellucid marginal degeneration,” “PMD,” “ectatic corneal disorders,” “keratoplasty in PMD,” “corneal cross-linking in PMD,” “ICRS in PMD,” “toric IOL PMD” and their Boolean combinations (AND/OR). The search was restricted to English-language studies involving human…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
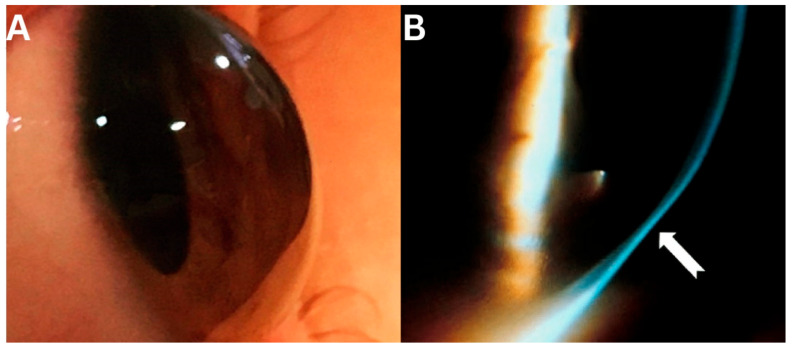 Figure 1
Figure 1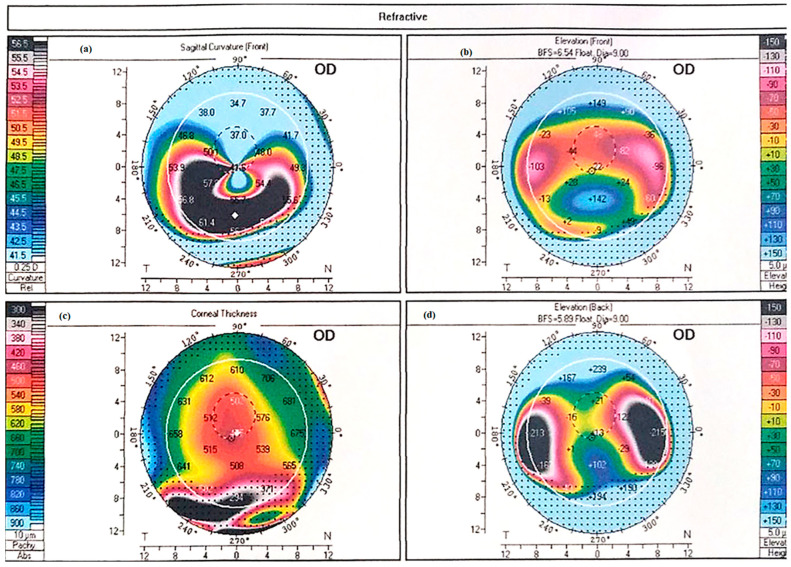 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal surgery and disorders · Ocular Surface and Contact Lens · Glaucoma and retinal disorders
1. Introduction
Pellucid marginal corneal degeneration (PMD) is a rare corneal ectatic disorder characterized by bilateral peripheral thinning of the cornea. This thinning typically presents as a crescent-shaped band, most frequently observed in the inferior quadrant, though other regions may also be affected [1,2]. The ectatic zone tends to be located more centrally, while the area of maximal thinning is usually situated 1–2 mm from the limbus [3,4].
PMD predominantly affects males in their second to fifth decades of life, often leading to reduced visual acuity due to high irregular against-the-rule astigmatism. Similar to keratoconus, PMD often demonstrates asymmetry in the extent and severity of corneal thinning between the two eyes. However, this asymmetry is less frequently emphasized in the literature, likely due to the rarity and variable clinical presentation of PMD [5]. Notably, PMD is far less common than keratoconus (KC), the most prevalent corneal ectasia [6,7]. The exact aetiology of PMD remains unclear, with several hypotheses proposed but no definitive consensus [8]. Furthermore, it is still debated whether PMD, KC, and keratoglobus represent distinct entities or phenotypic variations of the same spectrum [9,10,11]. Some researchers [2,11,12,13,14] have proposed that PMD may be a peripheral variant of KC, a notion supported by reports of concurrent PMD and KC in the same eye. For instance, Kayazawa et al. [15] documented KC features in 17 out of 20 PMD patients.
Despite available treatment options, the literature on PMD remains scarce, primarily consisting of case reports and small case series, with few large-scale studies [2]. This gap is further complicated by the frequent inclusion of mixed PMD–KC cohorts in research, making it difficult to draw conclusions specific to PMD alone.
2. Pathophysiology and Epidemiology
Similar to keratoconus, the pathophysiology of PMD remains incompletely understood. Histopathological studies have revealed structural abnormalities, including an absent or irregular Bowman’s membrane with focal breaks and occasional Descemet’s membrane folds [4]. Electron microscopy further demonstrates irregularly spaced collagen fibres, with an increased intracollagen space periodicity of 100–110 nm, compared to the normal range of 60–64 nm in healthy corneas [8]. These findings suggest an inherent biomechanical weakness in the corneal stroma, which may contribute to the disease’s progression.
Historically, PMD and other ectatic disorders were classified as non-inflammatory conditions [16]. However, emerging evidence challenges this view. For instance, McKay et al. [17] identified a link between endocrine dysfunction, pro-inflammatory metabolites, and the presence of KC. Additionally, studies have highlighted a potential association between sex hormones and KC, raising questions about similar mechanisms in PMD [18].
PMD exhibits a gender predilection (being much more prevalent in males with a 3:1 male to female ratio), though no clear ethnic predisposition has been established [8,9,19]. Given the shared pathophysiological features between PMD and other ectatic disorders, some researchers propose that these conditions may represent phenotypic variations of a single disease spectrum. Systemic factors, such as obesity and obstructive sleep apnea, have also been implicated in PMD [3]. Furthermore, ocular comorbidities, including atopic eye disease, are hypothesized to play a role in its development or progression [4,20].
Methods: A systematic literature search was performed in MEDLINE (via PubMed), Google Scholar, and Scopus up to February 2025 using the terms: “pellucid marginal degeneration,” “PMD,” “ectatic corneal disorders,” “keratoplasty in PMD,” “corneal cross-linking in PMD,” “ICRS in PMD,” “toric IOL PMD” and their Boolean combinations (AND/OR). The search was restricted to English-language studies involving human subjects, including case reports, case series, retrospective studies, clinical trials, and systematic reviews. Of the 237 initially identified articles, 98 were excluded after title/abstract screening for irrelevance or duplication, and 63 were excluded after full-text review due to insufficient PMD-specific data (e.g., mixed keratoconus/PMD cohorts without subgroup analysis). A total of 76 studies met the inclusion criteria, addressing diagnosis, pathophysiology, clinical features, and treatment outcomes in PMD. Given the heterogeneity and descriptive nature of the included studies, a narrative review framework was adopted, and no formal risk-of-bias assessment was conducted. Both conservative and surgical management options were evaluated, including contact lenses, collagen cross-linking (CXL), intrastromal corneal ring segments (ICRS), toric intraocular lenses (IOLs), and various keratoplasty techniques.
3. Clinical Signs
PMD is characterized by a linear area of corneal thinning located beneath the inferior region of corneal ectasia [10] (Figure 1). The hallmark of PMD is spatial dissociation between the zone of thinning and the ectatic zone, with maximal thinning typically located 1–2 mm from the limbus, while the area of protrusion appears more centrally (Figure 2).
On slit-lamp examination, the area of maximal ectasia, situated above the thinnest portion of the cornea, produces a distinctive “beer belly” appearance (Figure 1) [21]. This hallmark feature, combined with the characteristic “crab-claw” pattern observed on corneal tomography, aids in the clinical diagnosis of PMD. This structural configuration results in a high degree of irregular, against-the-rule astigmatism. However, in many cases, particularly in the early stages, the astigmatism remains relatively regular within the central 3 mm zone, which can contribute to better corrected visual acuity and is relevant when considering contact lens correction. In PMD, the cornea typically remains transparent, without deposits or vascularization, although Vogt’s striae may occasionally be observed [12]. The primary reason patients seek medical attention is a reduction in visual acuity due to irregular astigmatism, often accompanied by ocular discomfort or irritation [10,11,19].
Like other ectatic disorders, PMD is progressive in nature. However, unlike KC, PMD often has a delayed onset and can be more challenging to diagnose, further complicating its management [10].
4. Diagnosis
Although videokeratoscopy and corneal tomography have previously been used, corneal tomography—utilizing Scheimpflug imaging and/or a slit-scanning system—remains the gold standard for diagnosing and monitoring all forms of ectatic disease, including PMD. Additionally, anterior segment swept-source optical coherence tomography (AS-SS OCT) can provide complementary diagnostic data by generating detailed pachymetry maps and posterior elevation profiles, further aiding in the assessment and monitoring of PMD [22]. In PMD, the characteristic inferior peripheral thinning, accompanied by subsequent steepening, produces the distinctive “crab-claw” pattern—also referred to as the “kissing birds” (or historically “kissing pigeons”) appearance—on the curvature map of the tomography [13,14,15] (Figure 1). According to Krachmer, in severe cases of PMD, corneal steepness increases significantly, with the thinning area becoming progressively steeper from the centre toward the periphery [19]. This results in a curvature rise of up to 20 diopters.
Following the same principle, elevation maps reveal a heightened tomographical region within the affected area, while pachymetry measurements indicate reduced corneal thickness at the periphery and increased thickness centrally. However, it is crucial to avoid attributing this tomographic pattern exclusively to PMD. Instead, diagnosis should be made in conjunction with the patient’s medical history, slit-lamp examination, and refraction findings [10,23,24].
5. Differential Diagnosis
The differential diagnosis for PMD primarily includes other ectatic disorders such as keratoconus (KC) and keratoglobus, as well as peripheral thinning conditions like Terrien’s marginal degeneration. Inflammatory diseases, such as peripheral ulcerative keratitis and Mooren’s ulcer, should also be considered [10].
Early detection of PMD and KC can be challenging, as both conditions exhibit distinct slit-lamp and tomographic/pachymetric features only as they progress. PMD can be readily distinguished from keratoglobus based on its characteristic findings: keratoglobus is congenital and demonstrates diffuse corneal thinning and steepening, whereas PMD typically presents with an inferior “beer-belly” protrusion [16].
Mooren’s ulcer is easily identifiable due to its painful, inflammatory peripheral ulceration with an epithelial defect. Terrien’s marginal degeneration, though rarely confused with PMD, has key distinguishing features—it typically affects younger individuals and progresses slowly, with circumferential thinning often beginning superiorly [25]. Lipid deposition and pseudopterygium formation are also common [26,27].
Table 1 outlines the differential diagnoses of PMD.
6. Management
Assessment of disease severity and evaluation of the patient’s visual acuity are essential considerations in establishing the appropriate treatment method, either conservative or surgical, for PMD. Given that PMD is a relatively minor constituent of the ectasia spectrum, there is a paucity of research examining the efficacy of treatments for PMD.
7. Conservative Management
Early-stage PMD is initially managed with glasses or soft toric contact lenses (SCLs) for regular astigmatism [1,7,11,29], though their efficacy declines with disease progression. Rigid gas permeable (RGP) lenses—including corneal, limbal–miniscleral, and scleral designs—offer superior correction, with studies showing 75.5–95.4% achieving BCVA ≥ 20/40 [28,30]. Bitoric RGP designs enhance stability [31,32,33], while scleral lenses vault over irregular corneas, improving vision in advanced cases (78.7% ≥ 6/9 [34]) despite fitting challenges and tear exchange limitations [35].
Hybrid lenses (e.g., SynergEyes CooperVision, Gilbert, AZ, USA) combine RGP optics with soft lens comfort, achieving 20/30 vision but with 33% complication rates [36]. Newer designs like AirFlex, SwissLens, Prilly, Switzerland, show promise [37], though PMD-specific data remain limited.
Table 2 summarizes the findings and main takeaway messages from the conservative management options.
8. Surgical Management
Surgical management of PMD can be classified into the following types:
- (1)Alterations of corneal biomechanics
- (2)Toric intraocular lens implantation
- (3)Full-thickness surgery
- (4)Partial-thickness surgery
8.1. Alterations of Corneal Biomechanics
8.1.1. Collagen Cross Linking
Collagen Cross-Linking (CXL) is an established treatment for keratoconus and post-refractive surgery ectasia. The procedure uses UV radiation (365–370 nm) to catalyse photochemical reactions that strengthen the cornea by forming covalent bonds between collagen fibrils [38].
However, PMD presents unique challenges due to its inferior and irregular ectasia, which requires paracentral and peripheral UV application. This can lead to limbal irradiation, potentially compromising limbal stem cells and increasing the risk of limbal stem cell deficiency (LSCD). In PMD, the inferior thinning requires careful adaptation of the CXL protocol. As described by Kymionis et al. [38,39], a decentred UV irradiation zone may help target the ectatic area more effectively. While the use of UV-blocking contact lenses with central apertures to protect the limbal region has been suggested in clinical practice, this technique has not yet been formally evaluated in PMD-specific studies.
A literature review identified 13 studies evaluating CXL in PMD, including 8 case reports. Most employed the standard Dresden protocol, though some used accelerated CXL. The largest study (Iraipour et al., n = 40 eyes, 60-month follow-up [40]) found no significant change in mean BCVA post-CXL. While spherical equivalent and steep K-values remained stable in most patients, some experienced progression or improvement. In contrast, Mamoosa et al. [41] reported modest but significant gains in BCVA and reduced keratometry values. Case studies similarly noted improved BCVA and corneal flattening.
Irregular astigmatism in PMD remains difficult to manage, as CXL alone has unpredictable efficacy. A promising alternative is combined PRK and same-day CXL (CXL-plus), which may reduce irregular astigmatism and improve corneal regularity. However, it is important to note that adding PRK carries a higher long-term risk of ectasia progression compared to CXL alone.
Kymionis et al. (2009) first documented CXL in PMD, reporting stable ectasia and improved BCVA at 12 months [38,39]. The same group later observed similar success in a PMD patient with prior intracorneal ring segments (ICRS) [42].
Another study (n = 8 eyes) evaluated CXL-plus (transepithelial PTK + CXL) in PMD, showing improved UDVA (1.05 ± 0.33 to 0.41 ± 0.27 logMAR) and reduced astigmatism (−6.83 ± 2.33 D to −4.71 ± 1.89 D) at one year [43]
Cagil et al. used simultaneous transepithelial PTK + accelerated CXL, achieving reduced cylinder and spherical equivalent over 36 months—though without BCVA improvement [44].
Table 3 summarizes the key surgical interventions for PMD, comparing their mechanisms, indications, benefits, and limitations.
8.1.2. Intrastromal Corneal Rings
Intracorneal ring segments (ICRS) are medical devices composed of polymethyl methacrylate (PMMA) that are surgically implanted into the corneal stroma to modify its curvature and improve optical performance. The corneal incision for ICRS insertion can be created either manually using pocket micro-dissectors or with a femtosecond laser, typically at 50% corneal depth.
Several studies have investigated ICRS outcomes in PMD. ICRS have been shown to improve visual acuity and corneal topography in early to moderate pellucid marginal degeneration (PMD), reducing astigmatism and enhancing best-corrected visual acuity (BCVA) [45]. However, long-term complications—including regression, extrusion, and stromal melting—remain a concern. Recently, biologic alternatives such as allogenic corneal ring segments (CAIRS) have been introduced for keratoconus and may offer a promising future option for PMD [46]. These options are discussed in more detail in the Unmet Needs and Future Directions section.
The largest study by Hashemian et al. [45] utilized a femtosecond laser to implant single-segment Intacs SK rings (Addition Technology, USA) in 36 eyes of 26 patients. After six months, patients demonstrated a 2 D reduction in astigmatism, a 1.5 D decrease in mean keratometry, and improved BCVA from logMAR 0.42 to 0.16. Similarly, Kubaloglu et al. [47] reported outcomes using Keraring segments (Mediphacos, Brazil) with femtosecond laser-assisted implantation. At a mean follow-up of 30.7 months, astigmatism decreased by 2 D, maximum keratometry (Kmax) reduced by nearly 4 D, spherical equivalent improved by 3 D, and BCVA improved from logMAR 0.88 to 0.35. These findings were corroborated by Mularoni et al. [48], who observed comparable reductions in astigmatism and visual acuity gains.
Despite demonstrating efficacy in early-to-moderate PMD [10,45,49], ICRS use remains limited due to several challenges, including postoperative regression, unpredictable long-term visual outcomes, and the risk of sight-threatening complications such as corneal melting.
8.2. Toric Intraocular Lens Implantation
As with other surgical interventions for PMD, current evidence regarding toric intraocular lenses (IOLs) remains limited, underscoring the need for larger prospective studies to establish their safety and efficacy. Nevertheless, existing research—whether utilizing phakic or pseudophakic toric IOLs—demonstrates promising outcomes.
Balestrazzi et al. [50] reported improved BCVA and significant reductions in both sphere and astigmatism in 11 PMD eyes undergoing cataract surgery with pseudophakic IOLs, with no postoperative visual disturbances. Similar outcomes were observed by Matalia et al. [51], Bahar et al. [52], Han et al. [53], and Luck et al. [54], all noting enhanced BCVA and refractive stability following toric IOL implantation during cataract surgery.
For phakic toric IOLs, Camoriano et al. [55] (n = 10) documented a BCVA improvement from 20/20 to 20/18 and a reduction in spherical equivalent from −6.71 ± 0.9 D to −0.58 ± 0.1 D, while de Vries et al. [56] (n = 1) also reported satisfactory visual and refractive outcomes. Notably, one patient in Camoriano’s study required IOL explantation due to haloes and glare.
While toric IOLs demonstrate promising visual outcomes in PMD, several important limitations must be considered. First, the characteristic corneal ectasia in PMD often compromises biometry reliability, significantly complicating IOL power calculation and selection [57]. More fundamentally, while toric IOLs effectively address refractive errors, they do not correct the underlying corneal ectasia or provide biomechanical stabilization. This critical limitation means the procedure fails to halt disease progression, potentially allowing continued corneal deterioration that may require optical correction (e.g., spectacles) or additional surgical interventions in the future [51].
8.3. Full-Thickness Surgery
8.3.1. Penetrating Keratoplasty
Penetrating Keratoplasty (PK) in PMD
Penetrating keratoplasty (PK) remains a fundamental surgical intervention for advanced PMD cases, offering complete replacement of the irregular corneal tissue. The procedure presents unique challenges in PMD due to the characteristic inferior paracentral thinning, requiring large eccentric grafts that complicate both surgical execution and postoperative visual rehabilitation. Achieving optimal donor tissue centration proves particularly difficult, often resulting in challenging wound closure and significant postoperative astigmatism. Studies by Cherry et al. [58] and Tuberville et al. [59] have demonstrated that these peripherally placed grafts carry increased risks of corneal neovascularization, glaucoma, and graft rejection when positioned near the limbal vasculature.
The most comprehensive longitudinal study of PK in PMD by Tzelikis et al. [60] followed patients for nine years, documenting visual acuity improvement from 20/153 preoperatively to 20/43 at one year postoperatively. While other investigations reported acceptable postoperative astigmatism ranging from 0.75 to 2.46 diopters, they simultaneously noted concerning graft rejection rates approaching 50%. Given that PMD patients typically maintain healthy endothelial cell function, most surgeons reserve PK for cases refractory to other treatment modalities [61,62]. Even with successful graft healing, residual astigmatism frequently persists and can substantially compromise visual acuity. Consequently, many patients require supplemental optical correction—typically with rigid gas-permeable (RGP) or scleral contact lenses—to attain functional vision. This challenge is particularly relevant in PMD, where corneal irregularity often persists despite tectonic stabilization.
8.3.2. PK Surgical Alternatives
Full-Thickness Crescentic Wedge Resection
First described by Durand et al. in 1991 [62,63], full-thickness crescentic wedge resection eliminates the need for donor tissue by excising the thinned corneal stroma and approximating the remaining tissue. While offering faster recovery times compared to PK, this technique presents challenges with postoperative astigmatic drift, as documented in MacLean’s case series of 10 eyes [64]. Busin et al. [65] attempted to address this limitation by combining wedge resection with corneal relaxing incisions, achieving more stable refractive outcomes in their 10-eye series.
8.4. Partial-Thickness Procedures
Partial-thickness variations of crescentic wedge resection maintain endothelial integrity while still addressing the corneal ectasia. Genc et al. [66] reported BCVA improvement from 20/125 to 20/32 in their 10-eye series, though they observed a 10% rate of intraoperative microperforation. Technical refinements including pneumatically-assisted and femtosecond laser-assisted techniques developed by Tsatsos et al. [67,68] have enhanced the precision and safety of these procedures. Kymionis et al. [69] further advanced the technique by combining sectoral lamellar resection with corneal cross-linking, demonstrating stable visual outcomes at 14-month follow-up without disease progression.
8.4.1. Crescentic Lamellar Keratoplasty (CLK)
CLK represents a tissue-sparing alternative that replaces only the diseased anterior stroma while preserving the patient’s endothelium. This approach theoretically reduces rejection risk compared to PK but introduces new challenges, including graft–host interface opacification and significant postoperative astigmatism. The procedure demands considerable surgical expertise and currently lacks robust long-term outcome data from large prospective studies [70,71].
8.4.2. Deep Anterior Lamellar Keratoplasty (DALK)
DALK has emerged as a particularly promising alternative to PK for PMD, combining the advantages of lamellar surgery with excellent visual outcomes. The largest DALK series in PMD by Al Torbak et al. [72] demonstrated visual improvement from 0.9 to 0.4 LogMAR with a reduction in astigmatism from −8 to −4.3 diopters. The procedure carries technical challenges, with a 50% success rate for baring Descemet’s membrane and a 12.5% perforation rate in their 16-eye series. Smaller case reports by Kodavoor [73] and Millar [74] have corroborated these positive outcomes while emphasizing the technique’s steep learning curve.
8.4.3. Historical Techniques
Older surgical approaches, including lamellar thermokeratoplasty and epikeratoplasty, have largely been abandoned due to their association with high complication rates and unpredictable outcomes. These techniques have been replaced by the more refined lamellar procedures discussed above [74].
The surgical management of PMD continues to evolve, with current evidence suggesting that lamellar techniques may offer distinct advantages over traditional penetrating keratoplasty in appropriate cases. The relative rarity of PMD has limited the availability of large comparative studies, necessitating careful individualization of surgical approach based on patient-specific anatomical considerations and surgeon expertise. Future research should prioritize standardized outcome reporting and extended follow-up to better establish optimal treatment algorithms for this challenging corneal disorder.
Table 4 summarizes the benefits and limitations of full-thickness and partial-thickness surgical procedures for PMD.
9. Conclusions
Pellucid Marginal Degeneration: Diagnostic and Therapeutic Challenges
Pellucid marginal degeneration (PMD) represents a complex corneal ectatic disorder characterized by progressive inferior peripheral thinning and significant irregular astigmatism, leading to substantial visual impairment. While relatively rare, PMD presents distinct diagnostic and management challenges that often necessitate a coordinated, multidisciplinary approach to patient care.
Diagnostic Considerations and Early Intervention: Timely diagnosis remains critical in PMD management, with Scheimpflug-based corneal tomography emerging as the imaging modality of choice for detecting characteristic topographic patterns. This advanced imaging allows for early identification of the disease’s hallmark inferior “beer-belly” protrusion and peripheral thinning, enabling prompt intervention before significant visual deterioration occurs.
Therapeutic Approaches: The treatment paradigm for PMD follows a progressive approach:
Conservative Management: In mild to moderate cases, rigid gas permeable (RGP) or scleral contact lenses serve as first-line therapy, often providing excellent visual rehabilitation by neutralizing irregular astigmatism. These modalities frequently restore functional vision and significantly improve patients’ quality of life without surgical intervention.
Surgical Options: For progressive cases, collagen cross-linking (CXL) has shown promise in stabilizing corneal ectasia, while intracorneal ring segments (ICRS) can help regularize corneal topography. In patients with concurrent cataract or stable ectasia, toric intraocular lenses (IOLs) may offer effective refractive correction. However, these approaches require careful patient selection and thorough preoperative evaluation.
In advanced disease, penetrating keratoplasty (PK) or deep anterior lamellar keratoplasty (DALK) remain the definitive surgical options. While effective, these procedures carry inherent risks including graft rejection (particularly with PK), persistent astigmatism, and extended visual rehabilitation periods. Recent evidence suggests DALK may offer advantages in PMD cases due to its endothelial-sparing nature and lower rejection rates.
Unmet Needs and Future Directions: Despite these available treatment modalities, several critical limitations persist in PMD management. The field lacks standardized treatment algorithms, robust long-term outcome data for various interventions, and targeted therapies addressing the underlying disease mechanisms. These knowledge gaps highlight the need for future research focusing on multicenter studies to establish evidence-based protocols, basic science investigations to uncover novel therapeutic targets, and technological advancements in corneal imaging analytics. Additionally, refinement of lamellar surgical techniques and development of customized intracorneal ring segment designs may further improve outcomes for this challenging condition. A promising surgical approach for PMD is the use of Corneal Allogenic Intrastromal Ring Segments (CAIRS), which replaces synthetic PMMA rings with semicircular donor stromal tissue. In keratoconus, CAIRS has demonstrated improved biocompatibility, fewer complications (e.g., extrusion or stromal melting), and encouraging visual outcomes. Jacob et al. reported early safety and efficacy in keratoconus patients, with no implant-related adverse events [45]. Although CAIRS has not yet been extensively studied in PMD, its potential for better biologic integration and lower risk of foreign body rejection makes it a compelling alternative—particularly for high-risk eyes that may not tolerate synthetic implants. Future studies evaluating PMD-specific outcomes are needed to confirm its long-term efficacy.
Ultimately, optimal management of PMD requires careful staging and individualized treatment approaches guided by the specific characteristics and progression pattern in each patient. While current therapeutic options can effectively address various disease manifestations, significant opportunities remain for improving both diagnostic precision and treatment outcomes. A concerted research effort focusing on long-term outcomes, surgical innovation, and pathophysiological understanding will be essential to advance the care of patients affected by this vision-threatening disorder. Through such advancements, clinicians may one day be better equipped to preserve and restore vision in individuals with PMD, ultimately improving their quality of life and visual potential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sridhar M. Mahesh S. Bansal A.K. Nutheti R. Rao G. Pellucid marginal corneal degeneration Ophthalmology 20041111102110710.1016/j.ophtha.2003.09.03515177959 · doi ↗ · pubmed ↗
- 2Kompella V.B. Aasuri M.K. Rao G.N. Management of pellucid marginal corneal degeneration with rigid gas permeable contact lenses CLAO J.20022814014512144233 · pubmed ↗
- 3Sahu J. Raizada K. Pellucid marginal corneal degeneration Stat Pearls [Internet]Stat Pearls Publishing Treasure Island, FL, USA 202332965985 · pubmed ↗
- 4Cameron J.A. Mahmood M.A. Superior corneal thinning with pellucid marginal degeneration Am. J. Ophthalmol.199010948648710.1016/S 0002-9394(14)74624-02330956 · doi ↗ · pubmed ↗
- 5Karabatsas C.H. Cook S.D. Topographic analysis in pellucid marginal corneal degeneration and keratoglobus Eye 19961045145510.1038/eye.1996.998944096 · doi ↗ · pubmed ↗
- 6Gomes J.A.P. Rodrigues P.F. Lamazales L.L. Keratoconus epidemiology: A review Saudi J. Ophthalmol.2022363610.4103/sjopt.sjopt_204_2135971497 PMC 9375461 · doi ↗ · pubmed ↗
- 7Das A.V. Pillutla L.N. Chaurasia S. Clinical profile and demographic distribution of pellucid marginal corneal degeneration in India: A study of 559 patients Indian J. Ophthalmol.2021693488349310.4103/ijo.IJO_553_2134826981 PMC 8837343 · doi ↗ · pubmed ↗
- 8Krachmer J.H. Feder R.S. Belin M.W. Keratoconus and related noninflammatory corneal thinning disorders Surv. Ophthalmol.19842823229310.1016/0039-6257(84)90094-86230745 · doi ↗ · pubmed ↗