Infectious Proctitis Mimicking Advanced Rectal Cancer: A Case Report and Update on the Differential Diagnosis of Rectal Ulcerations
Anca Maria Pop, Roman Zimmermann, Szilveszter Pekardi, Michela Cipriani, Angelika Izabela Gajur, Diana Moser, Eva Markert, Alexander Kueres-Wiese

TL;DR
A case of syphilitic proctitis was mistaken for rectal cancer, highlighting the importance of considering infectious causes in similar presentations.
Contribution
This case report emphasizes the diagnostic challenge of syphilitic proctitis mimicking rectal cancer and underscores the need for thorough patient history.
Findings
The patient's symptoms and imaging initially suggested metastatic rectal cancer.
Histologic examination ruled out malignancy and inflammatory bowel disease, leading to a diagnosis of syphilitic proctitis.
Treatment with penicillin led to complete resolution of inflammation confirmed by follow-up tests.
Abstract
Background: Infectious proctitis remains an underrecognized entity, although sexually transmitted diseases, especially bacterial infections, exhibit a marked increase in their incidence. Methods: Here, we report a case of a 44-year-old man who presented to the emergency department with lower abdominal and rectal pain, tenesmus, fever and night sweats for the past 6 days. Results: The computed tomography initially revealed a high suspicion of metastatic rectal cancer. The endoscopic findings showed a 5 cm rectal mass, suggestive of malignancy. The histologic examination showed, however, no signs of malignancy and lacked the classical features of an inflammatory bowel disease, so an infectious proctitis was further suspected. The patient reported to have had unprotected receptive anal intercourse, was tested positive for Treponema pallidum serology and received three doses of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
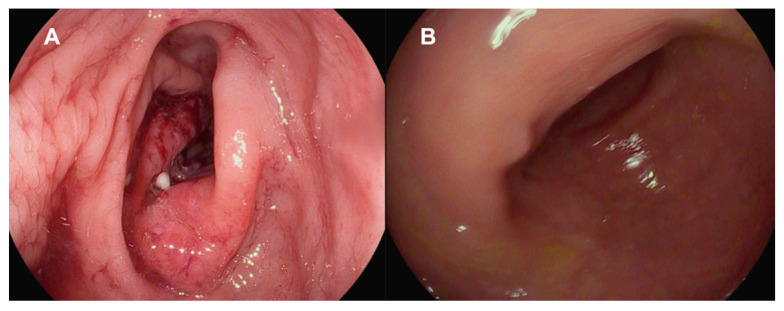 Figure 1
Figure 1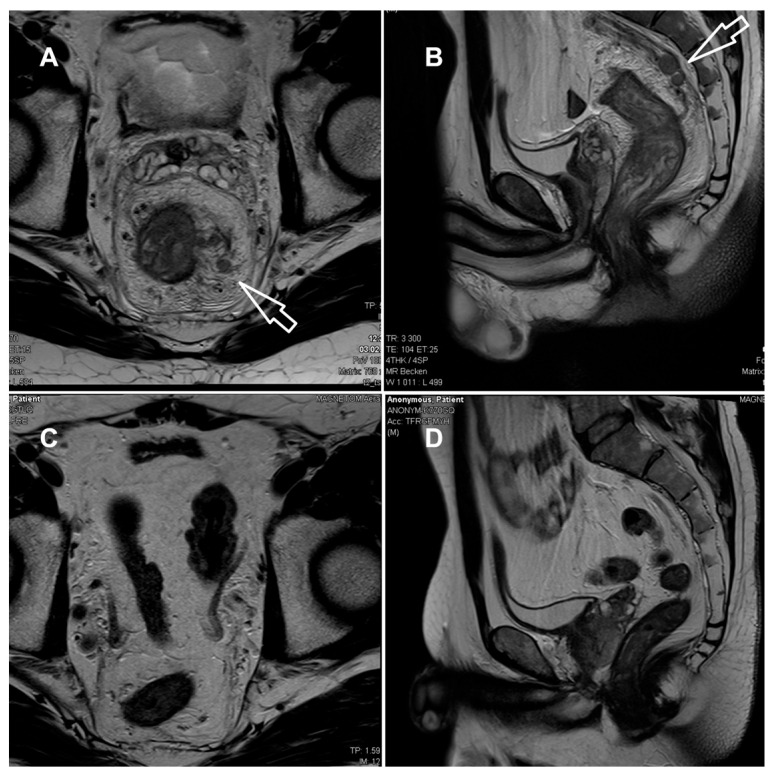 Figure 2
Figure 2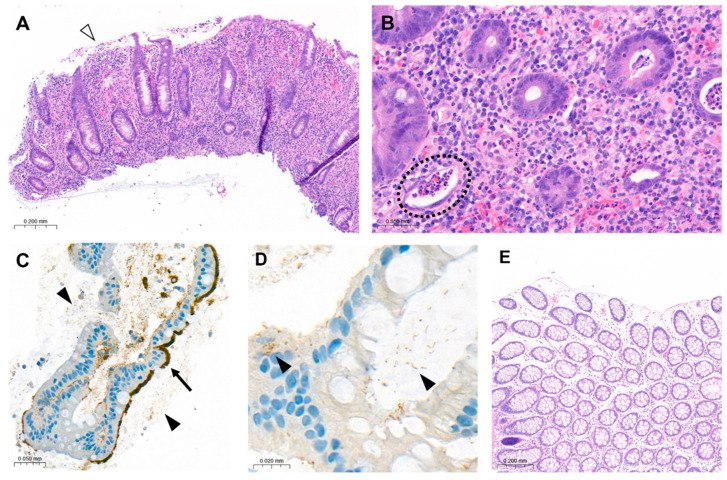 Figure 3
Figure 3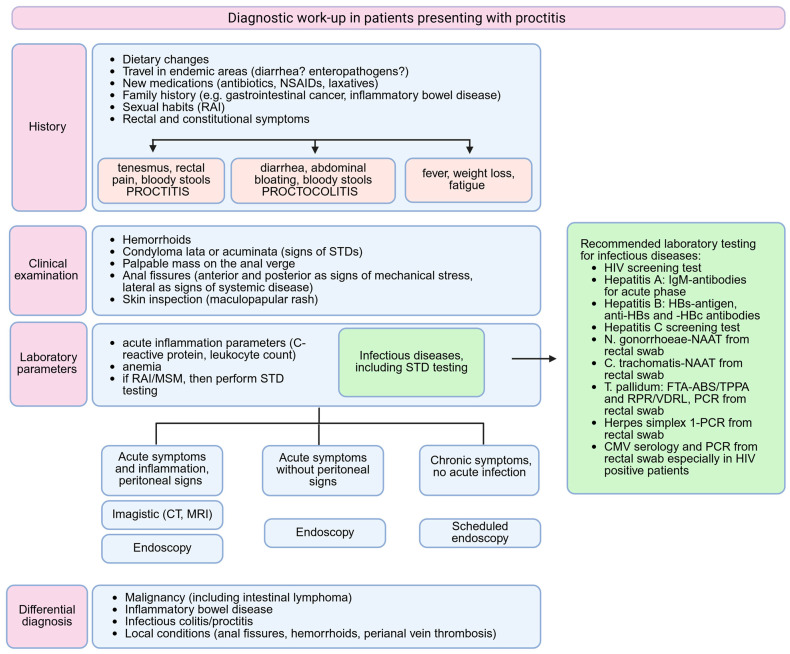 Figure 4
Figure 4- —Wil Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSyphilis Diagnosis and Treatment · Autoimmune and Inflammatory Disorders · Reproductive tract infections research
1. Introduction
Rectal ulcerations are uncommon and underrecognized manifestations of sexually transmitted diseases (STDs) due to their non-pathognomonic clinical features and inconclusive histopathological findings [1]. However, STDs must be considered in every patient presenting with rectal symptoms, due to the major implications regarding treatment and prognosis [2]. Furthermore, according to the Global Burden of Diseases 1990–2019 analyses, STDs reported a consistent increase in their absolute incidence [3].
During the last decade, in the light of emerging effective HIV treatments, the control of STDs has reached a plateau or may have even worsened for diseases such as syphilis [3,4]. The most commonly transmitted anorectal pathogens are represented by Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum and Herpes simplex virus (HSV), out of which T. pallidum reported the most marked increase since 1993 [3,5]. This trend is emphasized in higher income countries with functional screening programs, where there has been a significant rise in the incidence of bacterial infections, namely a 28% increase in gonorrhea and a 74% increase in syphilis, as reported in 2021 in the United States [4]. Syphilis exhibits a markedly high prevalence of up to 7.5% in men who have sex with men (MSM) [6]. Moreover, there are significant synergistic associations in the case of a HIV and syphilis co-infection; HIV weakens the immune system, predisposing to syphilis acquisition while syphilis fragilizes the rectal mucosa making it more vulnerable to HIV acquisition [7]. Infectious proctitis may be asymptomatic in some gonococcal and chlamydia infections [2], or may present as multiple ulcers mimicking an inflammatory bowel disease (IBD) or even a malignant tumour [8,9]. Based on these aspects, the initial acquisition of a broad personal history is of utmost importance before guiding the first diagnostic steps.
We present a case of syphilitic proctitis in a young man firstly confounded with an advanced rectal carcinoma, highlighting the most important features in the diagnosis of infectious proctitis. Moreover, the aim of our paper is to suggest a possible diagnostic work-up for proctitis and to summarize the most relevant aspects in the differential diagnosis of rectal ulcerations.
2. Case Presentation
A 44-year-old male patient presented to the Emergency Department of our hospital, complaining of a 6-day history of abdominal pain with migratory localisation and tenesmus. Moreover, the patient reported accompanying flu-like symptoms such as fever and malaise as well as night sweats. On the day of presentation, the abdominal pain was mainly localised in the left lower quadrant. The stools were normally formed and coloured; however, they exhibited a high frequency, up to hourly, and were painful. Weight loss was denied by the patient. The medical history was insignificant, revealing only well-controlled asthma. The family history was negative for malignancy as well as for IBD. Upon clinical examination, the patient reported tenderness on palpation in the left lower abdominal quadrant. Vital signs were normal with a blood pressure of 125/79 mmHg, heart rate of 95/min and an oxygen saturation of 97% on room air.
The laboratory parameters showed signs of inflammation with an elevated C-reactive protein of 110 mg/L; a leukocyte count of 4.3 G/L was normal. The computed tomography (CT) scan revealed a high suspicion of rectal carcinoma in the middle and distal third of the rectum with multiple regional and non-regional lymph nodes metastases. The patient was subsequently admitted to hospital and scheduled for a coloscopy with biopsy on the following day. The coloscopy showed a 5 cm tumour in the distal rectum with unremarkable surrounding mucosa in the rest of the colon and terminal ileum (Figure 1A). A magnetic resonance imaging (MRI) of the pelvis was advised for better definition and further described a semi-circumferential rectal carcinoma with vascular invasion, lymph nodes metastases and possible peritoneal involvement (Figure 2A,B). A CT scan of the thorax was unremarkable. The histological evaluation of the mucosal biopsies showed features of acute inflammation with erosions, cryptic abscesses with focal distribution and crypt destruction; in the lamina propria, there was an increased chronic lymphoplasmacytic inflammatory infiltrate with granulation tissue and epitheloid cell granulomas. There was no architectural disorder or signs of malignancy (Figure 3A,B). The Wartin–Starry stain and T. pallidum immunohistochemistry (IHC) (Figure 3C,D) highlighted multiple spirochetic bacteria on the mucosal surface in a band-like distribution, without clear evidence of intraepithelial bacteria, as characteristic of T. pallidum infection.
After clinicopathologic correlation of the available investigations, further serologic testing of the patient was performed. The patient reported a history of multiple sexual male partners. Tests for HIV and hepatitis B and C were negative. Both treponemal-specific tests (T. pallidum-hemagglutination-assay = TPHA and T. pallidum-antibodies) and a nontreponemal test (rapid plasma reagin, RPR) were positive. The polymerase chain reaction (PCR) results of a rectal swab were negative for T. pallidum, N. gonorrhoeae, C. trachomatis and HSV 1/2. Due to the negative T. pallidum-PCR from the rectal swab and lack of previous syphilis testing, which could have helped to estimate the time of infection, we diagnosed a late latent syphilis. Therefore, a treatment with a total of three doses of 2.4 million units of intramuscular benzathine penicillin G (once a week for 3 weeks) was recommended. The patient was symptom-free after the completion of the antibiotic treatment and no Jarisch–Herxheimer reaction was observed. A control rectosigmoidoscopy (Figure 1B), as well as the MRI (Figure 2C,D) at 3 months and the histologic evaluation (Figure 3E) showed a complete resolution of the inflammation.
3. Discussion
Syphilitic proctitis is a rare condition, which requires a high degree of suspicion before diagnosis and can otherwise mimic multiple conditions, extending from IBD to malignant patterns. Our case emphasizes the importance of a broad clinical history before initiating diagnostic steps, usually difficult to be performed in an emergency department. Despite the increasing incidence of STDs, especially of bacterial infections, the infectious proctitis seems to remain underrecognized. Firstly, rectal STD screening among MSM is less frequently performed compared to urethral screening [10]. Previous research showed that sexual health providers were two to six times more likely to perform urethral STD testing for gonorrhea and chlamydia than rectal testing [11]. Since the diagnosis of another STD is one of the most significant predictors of HIV acquisition and asymptomatic carriage is possible, testing for urethral, pharyngeal and rectal STDs should simultaneously be performed [12]. The clinical presentation is in the great majority of cases identical in STD and IBD proctitis, as symptoms such as anal discharge, tenesmus, fever, vomiting or weight loss significantly overlap [13]. Endoscopically, STD proctitis is associated with friable, ulcerated and hyperemic mucosa, which is also encountered in IBD. Moreover, the presence of rectal strictures or masses may indicate signs of malignancy [14,15]. Therefore, the diagnosis is often suspected based on the histologic examination, which fails to identify malignancy or IBD features. Histologically, the STD colitis lacks the IBD features such as cryptic damage, mucosal eosinophilia or presence of granulomas, being characterized by an abundant submucosal and perivascular plasma cell infiltrate [16].
To the best of our knowledge, there are approximately 50 cases of syphilitic proctitis described beginning from the 1960s. A summary of the available cases in the literature published in the last 25 years and their clinical and histological features is presented in Table 1.
Based on the previously published clinical data on STD proctitis, we suggest a possible algorithm, which can guide a reasonable diagnosis in patients presenting with rectal symptoms (Figure 4).
All cases were diagnosed in men and transgender women, initially presenting with symptoms and clinical findings related to rectal malignancy. A first diagnosis of infectious proctitis sparing an elaborate imagistic and histologic work-up was encountered only in cases of HIV-positive MSM or in patients presenting directly to a sexual health service with chronic symptoms [30,31,32,33,34,37].
A thorough medical history before initiating further endoscopic and imagistic diagnosis is important, as the identification of risk factors such as MSM, receptive anal intercourse (RAI) in the last 6 months or HIV seropositive status warrants STD testing [2]. If patients omit or refuse to mention these aspects, then a complete clinical examination could identify the presence of condylomata or anal fissures. Condylomata may sometimes be misdiagnosed as haemorrhoids and in patients presenting with multiple rectal and systemic symptoms a simple diagnosis of haemorrhoids should be doubted [38]. The number and localization of anal fissures matters, as the vast majority of anal fissures are due to mechanic stress, being in 90% of cases located in the posterior midline [49]. The presence of multiple or lateral fissures may indicate systemic disease such as syphilis, HIV, malignancy, Crohn’s disease or tuberculosis [49,50]. An acute presentation with new onset symptoms (fever, severe anal and abdominal pain, vomiting) can pose difficulties in following a specific algorithm, by necessitating an immediate diagnosis. An imagistic scan is not usually recommended as a first-line investigation, as it may lead to false diagnosis, such as rectal malignancy [51]. However, a CT scan may be performed when peritoneal signs are present, in a case in which an endoscopy is contraindicated, or in order to evaluate for possible internally draining abscess, strictures or mucosal ulcerations in the more proximal intestine [1]. Due to its higher costs, MRI is not a standard tool in an emergency department and is therefore performed in a later setting.
When infectious proctitis is suspected, several pathogens must be taken into consideration and simultaneously tested for identifying co-infections. The most prevalent rectal pathogens in MSM are C. trachomatis (average prevalence 9%) and N. gonorrhoeae (average prevalence 6.1%), which are both in the majority of cases asymptomatic; appropriate testing relies on the detection of pathogens by nucleic acid amplification tests (NAATs) performed from rectal swabs [52]. Lymphogranuloma venereum, caused by the C. trachomatis genovars L1, L2 and L3, is an endemic infection in MSM and usually presents as proctitis with purulent anal discharge, rectal bleeding and pain with possible pelvic lymphadenopathy; the detection of specific C. trachomatis-DNA is diagnostic and should be performed in all MSM with positive C. trachomatis rectal swabs [53]. Testing for rectal M. genitalium is not routinely recommended in MSM, since it has not been significantly associated with the development of proctitis and should be considered only in cases with persistent anal symptoms after excluding other infectious causes [2]. Cytomegalovirus can also cause rectal ulcerations and must always be tested in HIV-positive patients, as it is considered an indicator of advanced disease [2].
A combination of directly identified pathogens on the histologic sample and a positive serologic test is the preferred method for diagnosing an infectious proctitis [54]. In our case, there was no direct evidence of T. pallidum bacteria on the rectal biopsy; however, the lack of malignant and IBD classic features together with the serologic confirmation of an active syphilis indicated the diagnosis of a syphilitic proctitis. A diagnosis of primary rectal syphilis is frequently difficult as the rectal chancre, characteristic of this stage, is painless, superficial and discharges clear secretion. On the other hand, syphilitic proctitis indicates the progression to a secondary syphilis, being accompanied by systemic manifestations like fever or generalized lymphadenopathy [54].
The actual guidelines recommend the use of treponemal screening tests such as TPHA, T. pallidum particle agglutination assay (TPPA) or enzyme immunoassay (EIA), which are sensitive in detecting early syphilis, but may give false positive results. Nontreponemal tests such as RPR or the Venereal Disease Research Laboratory (VDRL) can detect only active syphilis and can miss very early forms of disease. If screening is based on the performance of both a treponemal and nontreponemal test, then the nontreponemal test must be performed quantitatively [54]. It is important to mention that in some patients a negative nontreponemal test may be followed by a positive treponemal test. This is due to an excess of antibodies in the undiluted serum, referred to as the prozone phenomenon in the early stages of syphilis, and is more often encountered in HIV-positive patients [34,39]. In our medical centre, however, a treponemal test is always first performed, and is, when positive, followed by a nontreponemal test. This allows the detection of the disease in early stages and reduces the chance of false negative interpretations due to the prozone phenomenon.
PCR tests are recommended for atypical sites of syphilis, such as oral cavity or rectum, where a distinction from the commensal spirochetes is needed [55]. However, the sensitivity and specificity of PCR in the secondary and latent stages of syphilis remain low, which impairs PCR testing from becoming a routine diagnostic tool. In a study by Shields et al., the sensitivity of PCR swabs in secondary syphilis was 50%, while the specificity was 100% [56]. Another study conducted by Costa-Silva et al. reported a sensitivity of 81% with the same high specificity of 100% [57]. The high chance of false negative PCR swabs in secondary syphilis was partially explained by various research groups based on the following possible hypotheses: the sample collection in routine PCRs usually lacks the required quality for a correct acquisition and the high antibody titres encountered in secondary syphilis impair the development of a high treponemal DNA load in tissue samples [58,59,60]. The direct visualization of spirochetes using dark-field microscopy or Warthin–Starry staining is specific, but difficult to be performed and often provides a false negative result [54]. When serology is negative, the IHC staining has excellent specificity in diagnosing secondary syphilis, but is not part of the routine diagnosis [58].
In our case, the sexual history, lack of malignant features on the histologic sample and the positive T. pallidum serology were considered suggestive and enough for sustaining the diagnosis of syphilitic proctitis, which was later confirmed by the resolution of symptoms under appropriate antibiotic therapy.
4. Conclusions
Syphilitic proctitis, although relatively rare among causes of infectious proctitis, requires a high degree of suspicion in order to avoid clinical overdiagnosis. It may mimic various conditions from IBD to rectal malignancy. Therefore, clinicians must be aware of the increasing incidence of STDs and perform the appropriate screening tests in high-risk populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Struyve M. Meersseman W. Van Moerkercke W. Primary syphilitic proctitis: Case report and literature review Acta Gastroenterol. Belg.20188143043230350534 · pubmed ↗
- 2de Vries H.J.C. Nori A.V. Kiellberg Larsen H. Kreuter A. Padovese V. Pallawela S. Vall-Mayans M. Ross J. 2021 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens J. Eur. Acad. Dermatol. Venereol.202171434144310.1111/jdv.1726934057249 · doi ↗ · pubmed ↗
- 3Zheng Y. Yu Q. Lin Y. Zhou Y. Lan L. Yang S. Wu J. Global burden and trends of sexually transmitted infections from 1990 to 2019: An observational trend study Lancet Infect. Dis.20222254155110.1016/S 1473-3099(21)00448-534942091 · doi ↗ · pubmed ↗
- 4Sinka K. The global burden of sexually transmitted infections Clin. Dermatol.20244211011810.1016/j.clindermatol.2023.12.00238142791 · doi ↗ · pubmed ↗
- 5Refugio O.N. Klausner J.D. Syphilis incidence in men who have sex with men with human immunodeficiency virus comorbidity and the importance of integrating sexually transmitted infection prevention into HIV care Expert. Rev. Anti Infect. Ther.20181632133110.1080/14787210.2018.144682829489420 PMC 6352966 · doi ↗ · pubmed ↗
- 6Tsuboi M. Evans J. Davies E.P. Rowley J. Korenromp E.L. Clayton T. Taylor M.M. Mabey D. Chico R.M. Prevalence of syphilis among men who have sex with men: A global systematic review and meta-analysis from 2000–20Lancet Glob. Health 20219 e 1110 e 111810.1016/S 2214-109X(21)00221-734246332 PMC 9150735 · doi ↗ · pubmed ↗
- 7Su R. Liu Y. Shan D. Li P. Ge L. Li D. Prevalence of HIV/syphilis co-infection among men who have sex with men in China: A systematic review and meta-analysis BMC Public Health 202525129710.1186/s 12889-025-22499-540197258 PMC 11974192 · doi ↗ · pubmed ↗
- 8Sousa M. Pinho R. Rodrigues A. Infectious proctitis due to syphilis and chlamydia: An exuberant presentation Rev. Esp. Enferm. Dig.201911181381410.17235/reed.2019.6175/201931545062 · doi ↗ · pubmed ↗