Knowledge and Risk Perception Regarding Keratinocyte Carcinoma in Lay People: A Systematic Review and Meta-Analysis
Luisa Leonie Brokmeier, Laura Ilic, Sophia Haas, Wolfgang Uter, Markus Vincent Heppt, Olaf Gefeller, Isabelle Kaiser

TL;DR
This study finds that the general public has low awareness and underestimates the risk of keratinocyte carcinoma, a common skin cancer, highlighting the need for better health education.
Contribution
The paper provides the first systematic review and meta-analysis on lay people's knowledge and risk perception of keratinocyte carcinoma.
Findings
Only 20.75% of respondents were aware of basal cell carcinoma, the most common type of keratinocyte carcinoma.
Respondents significantly underestimated the frequency of keratinocyte carcinoma, with only 7.21% identifying it as the most common skin cancer.
Concern about developing keratinocyte carcinoma was reported by only 25–30% of respondents, indicating low risk perception.
Abstract
Background/Objectives: The increasing incidence rates of keratinocyte carcinoma (KC), particularly in fair-skinned populations, call for efforts to intensify health education of the general population in addressing this prevalent skin cancer type. As a preparatory step, this systematic review summarizes the published research on the knowledge and risk perception regarding KC among individuals without medical training. Methods: The review was registered in PROSPERO (CRD42024618851) and adheres to PRISMA guidelines. The databases PubMed, Scopus, Web of Science, PsycArticles, and PsycINFO were searched on 30 July 2024. Studies were eligible if knowledge and/or risk perception was assessed in lay people. Risk of bias (ROB) was assessed with the Joanna Briggs Institute checklist for prevalence studies. Comparable outcomes (e.g., awareness of terms for KC) were meta-analyzed. Results:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
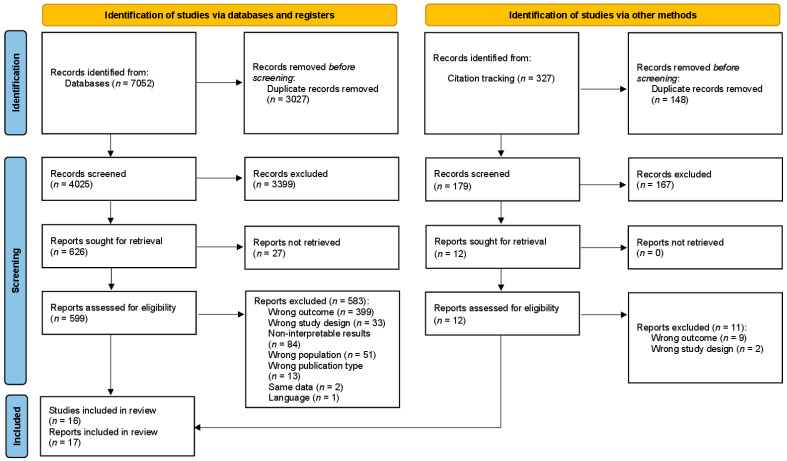 Figure 1
Figure 1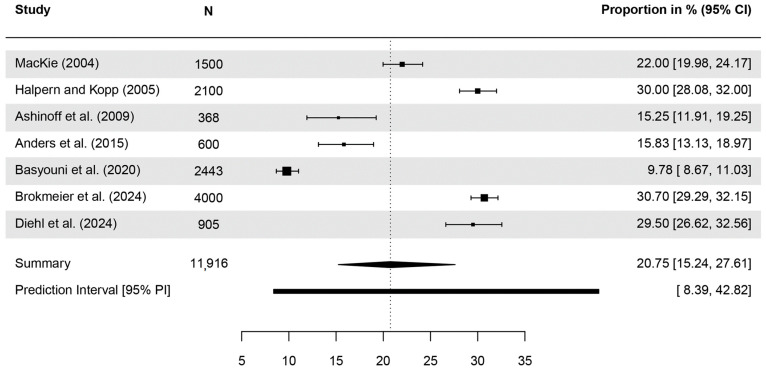 Figure 2
Figure 2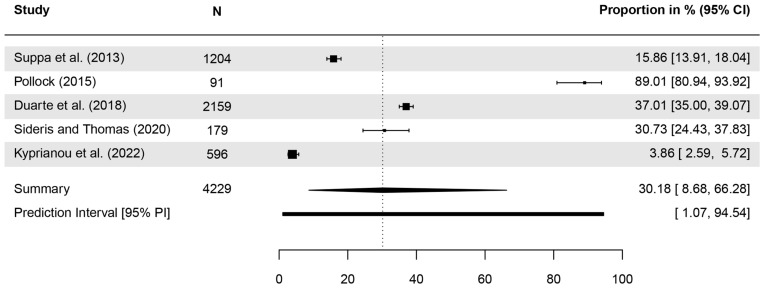 Figure 3
Figure 3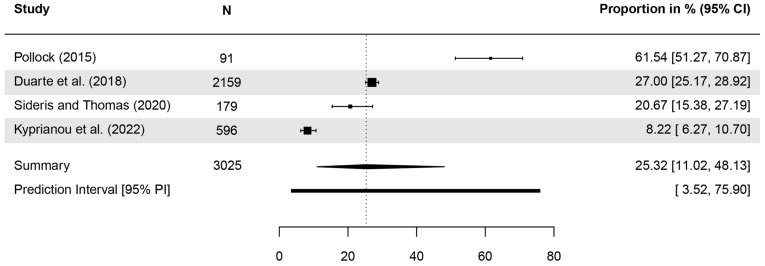 Figure 4
Figure 4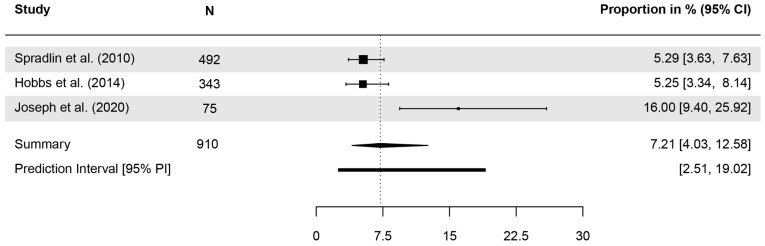 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNonmelanoma Skin Cancer Studies · Skin Protection and Aging · Cutaneous Melanoma Detection and Management
1. Introduction
Knowledge about a disease and its prevention, as well as personal risk perception regarding the disease, are factors influencing preventive behavior [1,2]. This is of relevance especially for preventable diseases that are very common, such as several types of cancer [3]. One of the most common types of cancers—especially among fair-skinned populations—is skin cancer, more specifically keratinocyte carcinoma (KC) [4,5,6]. KC, often referred to as nonmelanoma skin cancer (NMSC), comprises basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) [7]. The IARC Globocan database, comprising data from population-based cancer registries in 185 countries, shows that 1.23 million subjects were registered as incident KC cases in 2022 [8]. This reported incidence of KC seriously underestimates the global burden of these skin cancers, as some cancer registries do not routinely collect KC data and worldwide coverage of Globocan is incomplete [9,10]. Especially registration of BCC, which is the dominant subgroup of KC, is inadequate [11]. According to the Global Burden of Disease (GBD) Study [12], which employed sophisticated modeling techniques to correct for underreporting in registry data, there were an estimated 6.34 million incident cases of KC globally in 2021 [13]. Incidence rates are expected to increase further in the near future [6,14] and pose a large burden on healthcare systems [15]. Since for both BCC and SCC, extensive ultraviolet radiation (UV) exposure has been established as a strong risk factor [15,16], preventive measures in terms of a reduction in UV exposure could positively impact individuals’ health [17] and reduce the economic burden for healthcare systems [18]. A Belgian study conducted in 2016 estimated that investments in campaigns for skin cancer prevention would return 3.6 times of savings for healthcare providers [19].
Raising knowledge and awareness is an important preparatory step in the process of prevention. Even in secondary and tertiary prevention, health literacy is an important factor. According to a review, lower health literacy was associated with poorer quality of life and poorer experience of care in cancer patients [20]. Furthermore, trained medical personnel seem to overestimate health literacy in their (medically untrained) patients, impairing doctor–patient communication [21], highlighting the need to assess accurate levels of knowledge in lay people. As a starting point for prevention campaigns, it is therefore essential to first assess the knowledge and risk perception of KC among the general population to identify shortcomings. There are systematic reviews on skin cancer knowledge, e.g., [22] or consequences of sun exposure, e.g., [23], but not specifically for KC. A previous systematic review claims to have investigated knowledge and risk perception of KC [24]. However, none of the included studies assessed items on KC; they all referred to skin cancer in general. Nevertheless, the authors related their results to KC, since their goal was to provide advice on skin cancer prevention for outdoor workers. It is possible, though, that especially lay people with no professional training might perceive KC differently from skin cancer in general. Thus, to our knowledge, no systematic literature review has been conducted to address the knowledge and risk perception of KC in lay people. The aim of our work is to fill this gap by synthesizing all available information.
2. Materials and Methods
This systematic review was conducted and reported following the PRISMA guideline [25] (see Supplementary Material Table S1) as part of a larger review project registered with PROSPERO (registration number: CRD42024618851).
2.1. Eligibility Criteria
Following the SPIDER search strategy [26], all studies fulfill the following eligibility criteria:
- Sample: General population and subsamples thereof. Samples of participants with medical training (e.g., physicians, medical students, or nurses) or skin cancer patients were excluded.
- Phenomenon of Interest: Knowledge about, risk perception, or attitudes towards KC. This also includes awareness, familiarity, or beliefs. Studies focusing only on UV-related knowledge or UV behavioral assessment were excluded.
- Design: Cross-sectional surveys, cohort studies, baseline data of intervention studies.
- Evaluation: Items had to be sufficiently described to ascertain they were distinctly assessing the phenomenon of interest (i.e., no items referring to skin cancer in general or summary scores including other outcomes).
- Research Type: Quantitative, peer-reviewed studies. Qualitative studies, conference abstracts, dissertations, case reports, commentaries, editorials or reviews were excluded.
Studies published in German, English, and French were eligible.
2.2. Search Strategy
Five databases, including Medline (via PubMed), EMBASE (via Scopus), Web of Science, PsycArticles, and PsycINFO, were systematically searched using keywords and MeSH terms regarding knowledge and risk perception in combination with skin cancer (e.g., melanoma, nonmelanoma, keratinocyte carcinoma) and terms referring to the study design (e.g., interview* or cross-sectional). The detailed search strings and the syntax of the searches in the five databases can be found in the Supplementary Material Text S1. The search was conducted on 30 July 2024.
Furthermore, the method of forward and backward citation tracking [27,28] was used. For the latter, three systematic reviews [22,23,24] as well as one study [29] with similar research questions as this review were selected and their reference list extracted from Scopus. For the forward citation tracking, Scopus was used to identify and export all publications citing three main studies [30,31,32] on knowledge and risk perception regarding skin cancer. Before implementation and in accordance with the PRESS guideline [33], the search process had been reviewed by members of the team who were not involved in its original development.
All references rendered were allocated to an Endnote [34] library and duplicates were eliminated. The screening process was conducted and organized using the systematic review management software Rayyan [35]. In pairs, two researchers independently reviewed the titles and abstracts of this reference list for relevant articles (first screening phase). Following the rationale of sensitivity, inclusion by only one reviewer was sufficient to include the article for the full-text screening. In this second screening phase, the entire article was read by two researchers independently to decide upon its eligibility. During this screening phase, labels were applied to identify studies with items referring to knowledge and risk perception regarding KC. Additionally, all full texts were searched for KC-related terms to ensure that no studies were missed. Disagreements were discussed until a consensus was reached. If uncertainties prevailed, a third researcher was consulted.
2.3. Data Extraction
Two researchers independently extracted data on sample characteristics, item specifics, and results for each study using the Agency for Healthcare Research and Quality’s (AHRQ) Systematic Review Data Repository Plus (SRDR+, https://srdrplus.ahrq.gov, last accessed on 30 April 2025). Study and sample characteristics were collected on country and date of data collection, population, recruitment procedure, sample size, percentage of female and male participants, and participants’ age. As outcomes, we extracted details on the exact wording of the items assessed. If this was not explicitly stated in the methods section or in the Supplementary Material, the phrase used in the studies to report their results was extracted. The number of analyzed participants, number and/or percentage of responses, as well as further outcome details (e.g., sex differences) were extracted. On SRDR+, a form was created to ensure a standardized extraction process. We piloted the extraction with two randomly selected studies to detect any misunderstandings. SRDR+ automatically detects conflicts between extractions, which were checked and resolved by an independent third researcher.
2.4. Risk of Bias (ROB) Assessment
To assess the ROB of the individual studies, the Joanna Briggs Institute (JBI) checklist for prevalence studies [36] was applied. It includes nine items relating to sample selection, outcome measurement, analysis methods, and reporting standards. One item specifically assesses whether the sample size of the study is sufficient and thus requires a decision, in which a minimum sample size is considered sufficient. We set n = 250 as the required minimum sample size. This is to some extent arbitrary but justified as studies with a smaller sample size lead to estimates of proportions with 95% confidence intervals (CIs) that can exceed 10% in width, which we consider to be too wide. If criteria were met, items were answered with yes (versus no). Too little information reported in the study led to the verdict ‘unclear’. The JBI tool does not provide detailed instructions on how to conclude an overall ROB. We based the overall ROB rating on a joint critical appraisal of all relevant aspects, with low methodological study quality in key aspects not being compensated for by other components of the study with a higher methodological quality. We therefore established a rating standard as follows: High concerns or an unclear rating regarding items indicating a selection bias, measurement bias, or an inadequate sample size led to an overall rating of high ROB or unclear, respectively. In particular, inadequate sampling strategies and response rate management, invalid methods of measurement, or sample sizes below 250 were rated as high ROB. After establishing these decision criteria, studies were rated independently by two researchers each. In the case of discrepant ROB ratings, consensus meetings were held to discuss the disagreements and reach a consensus decision.
2.5. Data Synthesis
The main characteristics and ROB ratings of the included studies were summarized in a table. The results (i.e., proportions) regarding knowledge and risk perception were classified into subcategories to compare outcomes. Outcomes were comparable, if the items assessed the same construct on the same scale, reporting quantitative data on the proportion of the sample in said outcome categories. As subcategories for KC-specific knowledge, four topics were identified: (1) awareness of terms for KC, (2) identification of KC as a type of skin cancer, (3) knowledge regarding the prevalence of KC, and (4) more detailed, specific knowledge regarding KC. There was no study reporting risk perception regarding KC. However, concern about developing KC was found in two studies. Meta-analyses were conducted for comparable items if at least three studies were allocated in a subgroup. If not provided by the study, proportions and their corresponding confidence intervals (CIs) were calculated, using the Wilson method for the latter. The meta-analyses were conducted using a generalized linear mixed model (GLMM) with random effects. Between-study heterogeneity was assessed by calculating the I^2^-statistic (range 0–100%, with high heterogeneity assumed for I^2^ ≥ 75%) [37]. The maximum-likelihood estimator of the between-study variance (τ^2^) was derived from the GLMM and is additionally reported. In a scenario with high between-study heterogeneity, the 95% CI of the pooled estimate of the proportion of interest does not adequately reflect the uncertainty of statements about that proportion [38]. Therefore, we expanded the forest plot to also show the 95% prediction interval (PI) of the proportion of interest [39]. A 95% PI is defined as a range for the true proportion of interest that covers 95% of future study results. In contrast to the CI for the pooled meta-analytical estimate, the PI incorporates the structural between-study heterogeneity. We did not conduct statistical tests for publication bias since it is advised not to use them when pooling proportions [40]. Analyses were conducted in R version 4.2.2 using the R packages ‘meta’ and ‘metafor’.
3. Results
The search rendered initially 7379 references. After removal of duplicates, 4204 studies were screened in the first phase, and 638 in the second. Knowledge of and attitudes towards KC as defined in our inclusion criteria were addressed in 17 studies (see Figure 1; for a detailed list of exclusions during the full text screening, see Supplementary Table S2). Three studies [41,42,43] were excluded even though they explicitly addressed KC knowledge and risk awareness in their titles and/or abstracts. However, the items reported were only referring to ‘skin cancer’ in general, thus not meeting the predefined inclusion criteria. One study [44] was identified because it was cited in the methods section of one of the included studies [45]. Two of the included studies analyzed overlapping data from the same study [46,47]. Therefore, only data on the target population of outdoor workers was extracted from the second study [47].
Included studies were published between 1991 and 2024, with data assessed in Europe, USA, Australia, and Saudi Arabia. Sample sizes ranged from 37 to 4000, summing up to 16,728 individuals assessed (corrected for overlap between [46,47]). Age of participants ranged from 14 to 89 years, with proportions of female participants ranging from 0% to 70%. ROB was rated low in two studies, high in eight studies, and unclear in seven studies (Table 1). Inadequate convenience sampling or small sample sizes were the main reasons for high ROB ratings. Unclear ratings were due to insufficient reporting of study details.
3.1. Awareness of Terms for KC
Seven studies investigated whether participants were familiar with or had heard of terms referring to KC (Table 2). Colloquial terms for KC were assessed in two studies [46,47] and were most familiar to participants (60.9–72.8%). Awareness regarding the medical terms BCC (9.8–30.7%) [30,46,47,49,50,54,55] and SCC (22.6–23.0%) [46,47] was lower.
A meta-analysis of seven studies reporting quantitative data on awareness of the term BCC indicated a pooled estimate of 20.75% (95% CI = 15.24–27.61, τ^2^ = 0.25, I^2^ = 98.6%, p < 0.001; Figure 2). In one study, 32.7% of the sample knew at least one of four terms referring to SCC, while 12.8% knew of the term ‘Basaliom’ (German for BCC) [54]. Two studies [46,54] reported gender differences with females reporting a higher level of awareness of KC-specific terms.
3.2. Identification of KC as a Type of Skin Cancer
In six studies, participants were asked to identify BCC and SCC as types of cancer. Correct answers ranged from <10% [58] to 90% [44] (Table 3). Meta-analyses indicated that 30.18% (CI = 8.68–66.29, τ^2^ = 2.95, I^2^ = 98.9%, p < 0.001, included studies [k] = 5; Figure 3) and 25.32% (CI = 11.02–48.13, τ^2^ = 1.03, I^2^ = 97.8%, p < 0.001, k = 4; Figure 4) of respondents were able to identify BCC and SCC, respectively.
3.3. Knowledge Regarding the Prevalence of KC
Three studies investigated whether participants knew that BCC is the most common type of skin cancer. The correct response rate ranged from 5.2 to 16%, with a pooled proportion of 7.21% (CI = 4.03–12.58, τ^2^ = 0.22, I^2^ = 83.7%, p = 0.002, k = 3; Figure 5). When asked to estimate the prevalence of KC in comparison to malignant melanoma [46], only 27.4% correctly assumed KC to be more prevalent (Table 4).
3.4. Specific Knowledge Regarding KC
Four studies investigated specific knowledge regarding KC (Table 5). Correct responses regarding signs of KC ranged from 18.0% (‘Light or white spots on the skin’) to 72.8% (‘Reddish, rough, scaly skin spots’) [46,47]. Identifying which was not a sign of BCC was incorrectly answered by 41% [48]. Sunlight was known as a factor contributing to KC by 71.4–78.7% [46,47]. Almost half of the sample of the general population overestimated the severity of KC compared to malignant melanoma (equally severe: 37.4%, more severe: 12.4%), while 21.2% answered ‘I don’t know’ [46]. In another study, 43–73% of the participants were able to identify BCC and SCC as malignant in pictures of skin lesions [56]. Specific facts about BCC and SCC were asked as multiple-choice items in one study and yielded incorrect responses of 86% (SCC) and 52% (BCC), respectively [48].
3.5. Concern About Developing KC
Two studies [46,47] reported whether participants were concerned about developing KC. A greater proportion of the sample of outdoor workers expressed their concern (30.0%) compared to the general population (25.0%). However, in both samples, an even larger part of the study participants (32.0–37.3%) had never thought about it (Table 6).
4. Discussion
Our search for studies investigating knowledge and risk perception regarding KC identified 17 eligible studies for inclusion in this systematic review. Only two of these studies were rated as low in ROB, indicating a lack of high-quality research on the topic. All studies were conducted in countries of the Northern Hemisphere and Australia. Concerning South America, Africa, and Asia with their partly fair-skinned populations and non-negligible NMSC mortality rates [59], respectively, further research into relevant knowledge domains seems warranted. It is worrisome that there are no studies in these regions, and thus no indication of what knowledge level to build prevention campaigns on. This will lead to even greater inequalities in the future. While skin cancer incidence is expected to rise globally, this increase is predicted to be stronger in low- and middle-income countries [60]. In these countries, healthcare infrastructure and financial budgets for prevention are insufficient, which exacerbates existing inequalities [60]. The instruments used in the studies to assess knowledge and risk perception, as well as the sociodemographic and constitutional characteristics of the study samples, showed vast heterogeneity.
Overall, our synthesis of the study results revealed a low level of knowledge and awareness of KC: Only slightly more than one-fifth of respondents had heard of BCC or SCC. Acknowledging the fact that BCC and SCC are medical terms, the awareness of colloquial terms for KC was substantially higher in one German study. Still, about 30–40% of lay people were unaware of KC. In comparison, the proportions of individuals having heard of skin cancer are far higher (e.g., 97%) [52]. There is clearly a lack of awareness of the differentiation of skin cancer into different types, leaving the two most common types, BCC and SCC, unknown to most lay people. In women, this deficit of awareness seems to be less pronounced: Two of the included studies reported sex differences in awareness [46,54], with women being more aware of KC-related terms. This is in line with previous research, showing that women seem to be more knowledgeable of health topics in general [61]. The authors argue that this might be due to women’s role as care takers in families or because they might have more experience in navigating the healthcare system. Therefore, it might be reasonable to focus health education primarily on men [62]. Unfortunately, only two studies reported gender differences, but one of these did not report actual gender-specific proportions for women and men separately [54]. More research should determine whether there is a persistent gender knowledge gap.
Furthermore, the disease frequency of KC is underestimated by lay people: Only one in fourteen could identify BCC as the most common type of skin cancer. In the one study reporting all answers given, melanoma was assumed to be the most common form (63%) [57]. This might be due to the fact that melanoma is more fatal than KC, and thus receives more attention in health education campaigns [63]. However, since KC is more prevalent and incidences are expected to increase [64], it deserves more awareness.
The fact that UV radiation is a major risk factor for KC seems to be more common knowledge (71.4–78.7%). However, awareness of this causal relationship with skin cancer in general as opposed to KC seems to be far higher, reaching proportions of more than 90% [24]. This may indicate that some individuals regard KC as an entirely distinct form of cancer. On the other hand, one could argue that the proportion of awareness about the causal relationship between UV radiation and KC is surprisingly high, given the fact that most respondents in our analyses were unaware of KC. This might be explained by language differences: UV radiation as a risk factor for KC was an item in the German study [46,47], and was assessed using the colloquial German term for KC (‘white skin cancer’). This might have encouraged respondents to mingle in their knowledge about skin cancer in general or it might indicate that respondents conflate risk factors for KC and melanoma. This hypothesis is further supported by answers to items investigating knowledge about signs of KC. In Brokmeier et al. [46], more than 20% of respondents stated that changes in nevi are signs of KC, indicating that these respondents do not distinguish between KC and melanoma. Thus, there is conflicting evidence from the studies as to whether KC is perceived as a distinct type of skin cancer, or whether it is considered the same as or even a subtype of melanoma. Future research should investigate what exactly it is that the general population considers to be KC. This might have further implications for health education. Possibly, it would need to address a basic understanding of BCC and SCC as distinct types of skin cancer before conveying any more detailed information. All types of skin cancer are linked to UV exposure, but the harmful effects of different UV exposure patterns vary depending on the skin cancer type [65]. Populations with different sun exposure patterns thus require different skin cancer education specifically tailored to their needs, which means considering the pre-intervention knowledge level of the targeted population [66]. For instance, chronic UV exposure increases especially the risk for SCC, making this type of skin cancer highly relevant for outdoor workers [67]. Furthermore, signs vary among different types of skin cancer. Therefore, to promote secondary prevention, such tailored health education could include information on what signs to look for depending on skin cancer type. Even though the German Guideline Program in Oncology (GGPO) on Skin Cancer Prevention [68] highlights the importance on secondary prevention, it focuses only on melanoma in this regard. Our findings indicate that additional focus on the early detection of KC is needed. Acquisition of knowledge on risk factors and prevention should best be based on complete and reliable sources of information, such as the GGPO. However, it has been shown that a minority of internet resources meet these prerequisites [69].
Knowledge and risk perception are both factors included in several health behavior models (e.g., Behavior Change Wheel [70]; Health Belief Model [71]; Health Action Process Approach [72]). According to these models, knowledge alone is insufficient to prompt individuals to engage in preventive behavior. Beliefs or perceptions that there is a risk to the individual’s health play an essential role in the process of health behavior change [73]. For instance, a systematic review found associations between risk perception regarding breast cancer and preventive behavior [74]. As recommended by Edmonds et al. [75], risk perception regarding cancer should be assessed as comparative risk, i.e., asking participants to estimate their risk compared to others. However, our systematic search identified only two studies [46,47], using overlapping data, which investigated a form of risk perception about KC, namely, concern about developing KC. Results of these studies suggest that about one third of interviewed individuals have never thought about developing KC as opposed to a quarter of respondents actually being concerned, while the rest had never thought about it. This, as well as the underestimation of the high incidence of KC, indicate that there is a lack of awareness regarding the high probability of developing KC during lifetime, which, for example, has reached 69% in Australia [76]. Supporting this, a low risk awareness regarding KC was found in qualitative studies [77,78]. However, there is obviously a lack of quantitative data to draw public health policy conclusions. The high prevalence of KC calls for further studies addressing the perception of its risk in the general population.
Even though we did a comprehensive search for studies investigating knowledge and risk perception of KC with search terms covering a broad range of possible concepts and research items, we cannot exclude having missed relevant studies. Furthermore, as outlined in the Methods section, a formal assessment of publication bias for non-significant epidemiological or survey data is not recommended. However, we would expect a publication bias in this line of research favoring large sample sizes. Yet, we have found and included four studies with less than 250 participants, suggesting a probably negligible bias. The low number of studies included did not allow for quantitative syntheses of results for all subcategories of outcomes, let alone sensitivity analysis focusing exclusively on studies of low ROB or other subgroup analyses. A further problem that impedes the comparability of results is the considerable measurement heterogeneity in the studies. The resulting high heterogeneity of study-specific results is further reflected in very broad prediction intervals, indicating that future studies may find proportions for percentages of people aware of BCC ranging between one and 95%, in one instance. In particular, KC-specific knowledge items were too heterogeneously assessed in the included studies to be reasonably compared with another. For such a comparison, a standardized instrument would be required. Some studies, e.g., [79], have used the Skin Cancer and Sun Knowledge (SCSK) Scale [80] which assesses knowledge about sun protective behavior and (fewer) items on skin cancer in general. Two items of 25 refer to both melanoma and KC (most common type of skin cancer and signs of skin cancer). However, KC is not stated specifically. KC as the most common type of skin cancer deserves a more prominent role in the assessment of skin cancer knowledge. The SCSK could be adapted and used as a standardized assessment tool. Future items could assess knowledge about risk factors for and consequences of KC, types of skin cancer, or focus on the high prevalence of KC. In addition to a standardized assessment of KC-specific knowledge, transparent and complete reporting in the publications is also essential. This approach is imperative for the accurate interpretation of results and the evaluation of study quality. The STROBE guidelines [81] have been developed for the reporting of observational studies. It is recommended that subsequent studies adhere to these guidelines. Furthermore, analyses of temporal changes in knowledge levels over the last decades, which have been performed in the context of knowledge about melanoma risk factors [32,82], would be interesting but would require more comparable outcomes, as well. In two German reports [46,47], a culture-specific colloquial term (translated as ‘white skin cancer’) was used for KC in assessing knowledge. Proportions in awareness for colloquial terms might have been higher in other populations, but this has not been explored in other studies. This calls for further research in other cultures with their corresponding colloquial KC terms. Overall, the lack of high-quality research as well as the high heterogeneity observed in the conducted meta-analyses mandates caution in interpreting or generalizing the reported results. To decrease ROB, future studies should adhere diligently to adequate sampling strategies, since this was the main reason for high ROB ratings.
5. Conclusions
To our knowledge, this is the first systematic review of published literature on knowledge about and perception of KC. Overall, knowledge of and concern about KC seem to be rather low. However, only few studies were found, especially addressing the perception of KC, and those found showed heterogenous results and mostly a high ROB. Synthesizing the evidence from these studies was additionally hampered by the lack of standardized instruments for assessing outcomes related to knowledge and perception. This calls for the development of standardized assessment instruments and more research in this area, ultimately leading to better health education on KC for the general population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Majid U. Wasim A. Bakshi S. Truong J. Knowledge, (mis-)conceptions, risk perception, and behavior change during pandemics: A scoping review of 149 studies Public Underst. Sci.20202977779910.1177/096366252096336533073717 · doi ↗ · pubmed ↗
- 2Sheeran P. Harris P.R. Epton T. Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies Psychol. Bull.201414051154310.1037/a 003306523731175 · doi ↗ · pubmed ↗
- 3Anand P. Kunnumakkara A.B. Sundaram C. Harikumar K.B. Tharakan S.T. Lai O.S. Sung B. Aggarwal B.B. Cancer is a preventable disease that requires major lifestyle changes Pharm. Res.2008252097211610.1007/s 11095-008-9661-918626751 PMC 2515569 · doi ↗ · pubmed ↗
- 4Lomas A. Leonardi-Bee J. Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer Br. J. Dermatol.20121661069108010.1111/j.1365-2133.2012.10830.x 22251204 · doi ↗ · pubmed ↗
- 5Leiter U. Keim U. Garbe C. Epidemiology of Skin Cancer: Update 2019 Sunlight, Vitamin D and Skin Cancer Reichrath J. Springer International Publishing Cham, Switzerland 202012313910.1007/978-3-030-46227-7_632918216 · doi ↗ · pubmed ↗
- 6Brochez L. Volkmer B. Hoorens I. Garbe C. Röcken M. Schüz J. Whiteman D.C. Autier P. Greinert R. Boonen B. Skin cancer in Europe today and challenges for tomorrow J. Eur. Acad. Dermatol. Venereol.20253927227710.1111/jdv.2036839377431 · doi ↗ · pubmed ↗
- 7Karimkhani C. Boyers L.N. Dellavalle R.P. Weinstock M.A. It’s time for “keratinocyte carcinoma” to replace the term “nonmelanoma skin cancer”J. Am. Acad. Dermatol.20157218618710.1016/j.jaad.2014.09.03625497921 · doi ↗ · pubmed ↗
- 8Ferlay J. Ervik M. Lam F. Laversanne M. Colombet M. Mery L. Piñeros M. Znaor A. Soerjomataram I. Bray F. Global Cancer Observatory: Cancer Today International Agency for Research on Cancer Lyon, France 2024 Available online: https://gco.iarc.who.int/today(accessed on 30 May 2025)