Texture and Color Enhancement Imaging-Assisted Endocytoscopy Improves Characterization of Gastric Precancerous Conditions: A Set of Interesting Comparative Images
Riccardo Vasapolli, Johannes Raphael Westphal, Christian Schulz

TL;DR
A new imaging technique improves detection of early stomach cancer risks by enhancing texture and color in endoscopic views.
Contribution
Combining endocytoscopy with texture and color enhancement imaging improves visualization of gastric precancerous changes.
Findings
TXI mode enhances visualization of mucosal and cellular structures during endocytoscopy.
TXI-assisted endocytoscopy revealed small foci of intestinal metaplasia not visible with standard imaging.
Histological analysis confirmed the presence of intestinal metaplasia detected via TXI-enhanced endocytoscopy.
Abstract
Chronic atrophic gastritis and intestinal metaplasia (IM) are gastric precancerous conditions (GPCs) associated with an increased risk of gastric cancer. Early detection and accurate characterization of GPC are therefore crucial for risk stratification and the implementation of preventive strategies. In the absence of clear mucosal changes observed through white-light imaging (WLI) or virtual chromoendoscopy, endocytoscopy can help unveil the presence of GPC by enabling in vivo assessment of nuclear and cellular structures at ultra-high magnification. Endocytoscopy is typically performed using WLI following dye-based staining of the mucosa. In this case, we demonstrate that combining endocytoscopy with the texture and color enhancement imaging (TXI) mode substantially improves the assessment of the gastric mucosa. In a 61-year-old man undergoing esophagogastroduodenoscopy, WLI showed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
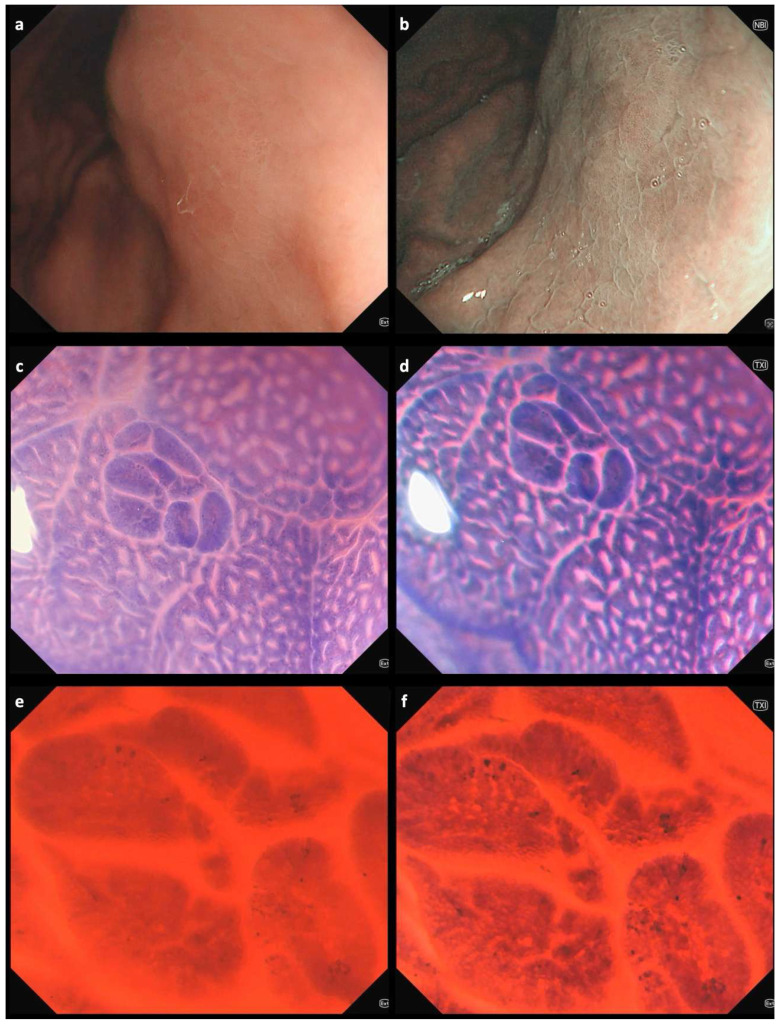 Figure 1
Figure 1- —ERANET Bavaria and Helicopredict projects
- —Deutsches Zentrum für Infektionsforschung, Partner Site Munich, Germany
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Colorectal Cancer Screening and Detection · Barrier Structure and Function Studies
Figure 1. Endoscopic images of a gastric area in the stomach corpus using white-light imaging (WLI) (a) and narrow-band imaging (NBI) (b), showing mild multifocal erythema and edema. The pit pattern reveals an uneven distribution of gastric pits and the subepithelial capillary network [1,2]; collecting venules are not visible. However, no clearly delineable lesions are observed. Endocytoscopic images from the same gastric area obtained using WLI (left) and texture and color enhancement imaging (TXI) (right) modes at different magnifications: (c,d) 150×; (e,f) 520×. Endocytoscopic assessment of defined lesions is usually performed after double staining with methylene blue and crystal violet [3,4]. In the stomach, repeated staining following mucus removal using mucolytic and defoaming agents may be necessary to obtain clear endocytoscopic images [5]. In our case of a 61-year-old man referred for esophagogastroduodenoscopy due to dyspeptic symptoms, endocytoscopy facilitated the detection of intestinal metaplasia. Characteristic changes observed through endocytoscopy include narrowing of glandular lumens, increased dye uptake, and the presence of goblet cells [6,7]. These features were even more clearly visualized when endocytoscopy was combined with TXI mode (Video S1), which enhances the visualization of structure, color tone, and brightness, thus facilitating the detection of subtle mucosal changes often missed by standard WLI [8]. The patient, who also had a positive family history of gastric cancer, was included in a three-year surveillance program in accordance with current guidelines [9]. Extensive atrophic and metaplastic changes involving both the stomach antrum and corpus are associated with the highest risk of gastric cancer development [10]. These conditions are generally identifiable using modern high-resolution white-light endoscopy combined with image-enhanced modalities such as TXI, NBI, blue laser imaging (BLI), or iScan. TXI is a readily accessible feature on modern Olympus endoscopy systems, activated similarly to NBI by simply pressing a dedicated button, which enhances mucosal texture and color contrast in real time—improving the detection of subtle lesions without requiring additional equipment or significant changes to the endoscopic workflow. Endocytoscopy may serve as a complementary tool in selected cases—particularly when subtle changes remain unclear or when targeted biopsies are required in areas without obvious mucosal alterations, especially in high-risk individuals. The transition from probe-based to fourth-generation endocytoscopy has led to significant technical advancements. In the current system, the endocytoscope is fully integrated into the distal end of a standard gastroscope or colonoscope, eliminating the need for a separate probe [3]. However, despite this progress, several limitations continue to restrict the widespread adoption of the technology. These include the need for dedicated training to obtain high-quality images—typically after a minimum of 30–50 procedures—as well as the requirement for dye-based chromoendoscopy, which can be time-consuming and particularly challenging in the stomach due to mucus interference. Further development is necessary to make endocytoscopy more practical and user-friendly. In this regard, the integration of artificial intelligence is likely to play an important role in enhancing image interpretation and clinical applicability, as suggested by preliminary studies [11,12].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Uchima H. Yao K. Endoscopic microanatomy of the normal gastrointestinal mucosa with narrow band technology and magnification Gastroenterol. Y Hepatol.20194211712610.1016/j.gastrohep.2018.10.00230471720 · doi ↗ · pubmed ↗
- 2Kurtcehajic A. Zerem E. Bokun T. Alibegovic E. Kunosic S. Hujdurovic A. Tursunovic A. Ljuca K. Could near focus endoscopy, narrow-band imaging, and acetic acid improve the visualization of microscopic features of stomach mucosa?World J. Gastrointest. Endosc.20241615716710.4253/wjge.v 16.i 3.15738577642 PMC 10989255 · doi ↗ · pubmed ↗
- 3Abad M.R.A. Shimamura Y. Fujiyoshi Y. Seewald S. Inoue H. Endocytoscopy: Technology and clinical application in upper gastrointestinal tract Transl. Gastroenterol. Hepatol.202052810.21037/tgh.2019.11.1232258532 PMC 7063519 · doi ↗ · pubmed ↗
- 4Vasapolli R. Neuhaus L. Schirra J. Neumann J. Mayerle J. Malfertheiner P. Schulz C. Microscopic alterations of the gastric mucosa in preneoplastic lesions as assessed by new-generation endocytoscopy Endoscopy 202355 E 998E 100010.1055/a-2119-121237604457 PMC 10442195 · doi ↗ · pubmed ↗
- 5Misawa M. Kudo S.-E. Takashina Y. Akimoto Y. Maeda Y. Mori Y. Kudo T. Wakamura K. Miyachi H. Ishida F. Clinical Efficacy of Endocytoscopy for Gastrointestinal Endoscopy Clin. Endosc.20215445546310.5946/ce.2021.16534233111 PMC 8357585 · doi ↗ · pubmed ↗
- 6Sato H. Inoue H. Hayee B. Ikeda H. Sato C. Phalanusitthepha C. Santi E.G.R. Kobayashi Y. Kudo S.-E. In vivo histopathology using endocytoscopy for non-neoplastic changes in the gastric mucosa: A prospective pilot study (with video)Gastrointest. Endosc.20158187588110.1016/j.gie.2014.08.01925442082 · doi ↗ · pubmed ↗
- 7Chiu P.W.Y. Ng E.K.W. To K.F. Teoh A.Y.B. Lam C.C.H. Chan F.K.L. Sung J.J.Y. Lau J.Y.W. Recognition of goblet cells upon endocytoscopy indicates the presence of gastric intestinal metaplasia Dig. Endosc.201426525610.1111/den.1205023551261 · doi ↗ · pubmed ↗
- 8Sato T. Schmid M. TXI: Texture and Color Enhancement Imaging for Endoscopic Image Enhancement J. Healthc. Eng.20212021551894810.1155/2021/551894833880168 PMC 8049784 · doi ↗ · pubmed ↗