Assessment of Factors Associated with Misperception of Body Weight and Body Weight Modifications Intentions Among Adults from Saudi Arabia: A Cross-Sectional Study
Ibrahim M. Gosadi

TL;DR
This study explores how adults in Saudi Arabia misperceive their body weight and how this affects their intentions to change their weight.
Contribution
The study identifies specific factors associated with body weight misperception in a Saudi population.
Findings
54% of participants had a wrong perception of their body weight.
Gender, employment, and BMI levels were statistically associated with body weight perception.
Misperception may hinder intentions for healthy behavioral change.
Abstract
Background/Objectives: Misperception of body weight might be associated with the likelihood of being in a pre-contemplation phase and with a limited intention to initiate a healthy behavioral change toward weight management. The current study investigates factors associated with the misperception of body weight, body weight satisfaction, and intentions for body weight modifications. Methods: This study utilized a cross-sectional design to reach adults from Jazan, in the southwest of Saudi Arabia. The data collection tool measured demographics, the participants’ latest height and weight, body weight perception, satisfaction, and intentions concerning body weight modification. Chi-squared tests were used to compare the demographic characteristics between those who had correct perception and those who had a wrong one. Results: A sample of 685 adult participants was included in the current…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
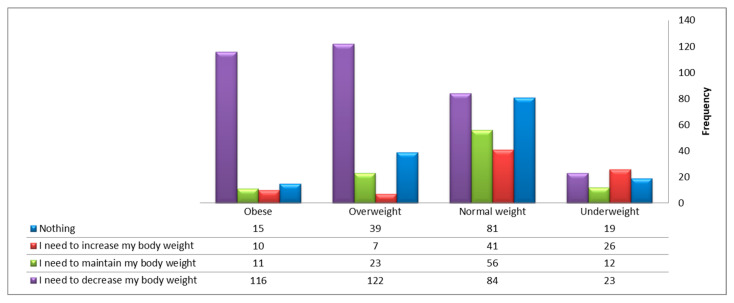 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEating Disorders and Behaviors · Obesity and Health Practices · Body Image and Dysmorphia Studies
1. Introduction
Malnutrition can be bidirectional, where excess or deficiency in food intake can lead to either being underweight or overweight and obese [1]. Perception of body weight and body image might impact satisfaction and subsequent behavior toward body weight control. On some occasions, wrong perception can lead to improper satisfaction or dissatisfaction with body weight and may result in the adoption of unhealthy practices.
Body weight abnormalities are a global health concern, especially with the high prevalence of overweight and obesity [1], and the associated rising incidence of chronic noncommunicable diseases and related mortalities. According to the World Health Organization, noncommunicable diseases were responsible for the deaths of over 43 million individuals in the year 2021, with cardiovascular diseases accounting for most of these mortalities [2]. Unhealthy lifestyle factors, including raised consumption of salt [3], carbohydrates [4,5], and fats [6], low levels of physical activity [7], and being overweight or obese [8], are major contributors to the increasing impact of noncommunicable diseases.
Promotion of the importance of healthy body weight is beneficial in increasing awareness about reducing the risk of chronic diseases, preventing premature deaths, prolonging life expectancy, and enhancing quality of life. Nonetheless, despite awareness of the benefits of promoting healthy body weight and proper lifestyle, some individuals might be at risk of developing a negative and harmful perception about their body weight. The increased use and influence of social media platforms might affect how people think about their body weight, leading to body shaming and stigmatization, and may induce problematic behavior related to weight [9]. Distorted perceptions of body weight might lead to either overestimation or underestimation.
Overestimation can lead to setting unrealistic weight loss goals and adopting unhealthy dietary habits [10]. On the contrary, some might underestimate their body weight, leading to higher satisfaction levels even when having excess weight [11]. This normalization of excess body weight can result in the adoption of unhealthy lifestyles and reduce the willingness to adopt weight control measures.
Willingness to change a behavior in order to adopt a healthy life can be explained by the transtheoretical model. This model is composed of six stages which are precontemplation, contemplation, preparation, action, maintenance, and termination [12]. The normalization of abnormal body weight and the associated misperception can leave some individuals in the precontemplation stage and lower their probability of adopting healthy behavior. Therefore, this might reduce the awareness about the importance of the required modification of the behavior and may delay the progress toward the remaining stages of a change in lifestyle.
According to the American College of Lifestyle Medicine, a healthy lifestyle involves six main elements: nutrition, physical activity, stress management, high-quality sleep, social connection, and avoidance of risky substances [13]. It can be postulated that distorted body perception may have a direct correlation with the majority of these elements. For example, weight loss management is believed to involve the cognitive characteristics of behavioral change [14,15].
Exposure to risky substances which can affect lifestyle varies according to populations. One of the studied substances that can impact lifestyle is Khat chewing which is mainly practiced in eastern countries in Africa [16] and southwestern regions of the Arabian peninsula [17,18]. Additionally, Khat chewing is also practiced among migrants living in Australia [19], USA [20], and European countries [21,22,23]. Khat has a stimulant characteristic as it contains cathinone. Additionally, Khat chewing is linked to several health consequences including mental, oral and gastric, cancer, metabolic, and nutritional conditions [24,25].
The observed influence of body weight perception on how individuals evaluate their weight status can be suggested as a primary screening measure for managing body weight abnormalities. This step can assist in identifying the stage of behavior change and assessing readiness to maintain healthy practices toward weight management. The current study measures how people view their body weight in relation to their estimated body mass index (BMI). Additionally, the study investigates the concordance between actual and perceived BMI and assesses factors associated with a wrong perception of body weight.
2. Materials and Methods
2.1. Study Design and Context
This assessment is part of an investigation that targeted adults in the Jazan region to assess BMI profile, perceptions, and methods of modifying body weight. This study utilized a cross-sectional design to reach adults from Jazan, in the southwest of Saudi Arabia. Adults living in the Jazan region were included regardless of nationality or gender. Exclusion criteria were limited to being under 18 or refusing to provide consent to participate. The measurement was conducted between November 2023 and May 2024. Participation was anonymous and voluntary, and data were collected after securing ethical approval from the Standing Committee for Scientific Research of Jazan University (number REC-44/06/446, dated December 2022).
2.2. Data Collection Tool
The developed data collection tool had five main components. The first component measured the main demographics of the participants, including age, gender, area of residence, education level, employment, monthly income, smoking, khat chewing, and having a diagnosed medical condition. The second component involved asking about the participants’ latest height and weight. The third component asked how the participants perceived their body weight—as low body weight, normal body weight, overweight, or obese. The fourth item asked about the degree of satisfaction with their current body weight. Finally, the participants were asked about their intentions concerning body weight—either to modify their body weight or to have no intention of modification.
2.3. Data Collection Process
The questionnaire was converted into an online format using Google Forms. A web link was generated and distributed on social media platforms to reach the required sample. The first page of the form contained an information sheet describing the study’s purpose and the steps to allow individuals to provide informed consent. Those who consented were granted access to the questionnaire, and those who refused were directed elsewhere.
Sampling for this investigation was not random and was mainly based on convenience sampling. Participants who agreed to take part were encouraged to share the web link with other potential participants. The sample size estimation was based on findings from a similar study conducted in Saudi Arabia, which found that 66% of adolescents had a wrong perception of their body weight [26]. The StatCalc function of Epi Info was used to estimate the sample size. A sample of 595 was calculated, assuming a 66% prevalence of adults with a wrong perception of their body weight, a 99% confidence level, and a 5% margin of error.
2.4. Data Analysis
Data analysis was conducted using the Statistical Package for Social Sciences, version 25. Frequencies and proportions were used to summarize binary and categorical variables. Mean and standard deviation (SD) were used to summarize continuous variables. BMI was estimated by dividing the reported weight in kilograms by the reported squared height in meters. The estimated BMI values were categorized into underweight, normal weight, overweight, and obese according to World Health Organization classification guidelines [27]. Cross-tabulation was used to assess concordance between body weight perception, as reported by the participants, and the estimated BMI category. The kappa test was used to measure the magnitude of agreement between the two measures. Furthermore, chi-squared tests were used to compare demographic characteristics between those with correct perception and those with incorrect perception. All the measured demographic variables were either binary or categorical except for age which was dichotomized based on the estimated sample mean as either 31 or younger or older than 31. A follow-up comparison was made to assess satisfaction levels according to whether participants underestimated, correctly estimated, or overestimated their body weight. Finally, a comparison was made to examine the intention to modify body weight according to BMI level. A p-value of 0.05 or less was considered statistically significant for the applied statistical tests.
3. Results
A total of 908 individuals were approached in the current investigation, of whom 223 were excluded due to refusal to participate, being under 18, or not providing the information required to estimate BMI. Ultimately, a sample of 685 adult participants was involved in the current analysis, which exceeded the estimated sample size due to the utilized online approaching method. The demographic data of the sample are displayed in Table 1. The mean age of the participants was 31.3 (SD: 11.1). The proportion of female participants was 52%, and more than half of the sample (55%) were from urban areas. Majority of the participants had a university education (77%), and 44% were employed or business owners. When participants were asked about their monthly income, the most frequent response was less than 5000 SAR (45.7%). Majority of the participants were never smokers and had never chewed khat. Less than half of the participants (43%) reported being diagnosed with a chronic condition. The estimated BMI of the participants indicated that 38% had normal body weight, 11% were underweight, and the remaining 50% were either overweight or obese.
Fifty-four percent of the participants had a wrong perception of their body weight. Among those with incorrect perceptions, 244 participants (35.6%) underestimated their body weight, whereas 130 participants (19%) overestimated it. Table 2 compares the demographics of the sample according to whether participants had a wrong or correct perception of their body weight. Gender, employment, smoking, khat chewing, having a diagnosed condition, and BMI levels were statistically associated with wrong body weight perception (p-values < 0.05). The frequency of women reporting wrong perceptions of body weight was higher compared to men. The frequency of incorrect perception was the lowest among students in comparison to other employment groups. Wrong perception of body weight was less common among current or former smokers and khat chewers. This may suggest that those exposed to smoking or khat chewing, either currently or previously, might be more likely to be aware of their body weight in comparison to those who were never smokers or never khat chewers. Wrong perception was also more frequent among those with a diagnosed condition. The highest frequency of wrong perception was detected among obese and underweight individuals in comparison to other BMI categories. Other demographic factors such as age, education level, area of residence, and monthly income were not associated with the misperception of body weight in the current sample.
As shown in Table 3, participants were categorized according to their estimated BMI category and cross-tabulated with their perception of body weight. It can be noted that the proportion of participants who were able to correctly identify their BMI category was 37% for those who were underweight, 56% for those with normal weight, 36.7% for those who were overweight, and 68.8% for those with obesity. The identified kappa value of agreement between perceived body weight and actual estimated BMI was 0.22, suggesting low agreement. Eighteen individuals described themselves as having low body weight, although they were categorized as overweight or obese. Among those who described themselves as having normal weight, 10% were underweight, and 33% were either overweight or obese. Underestimation of body weight was observed among the sample, where among 191 participants who were categorized as overweight, 74 participants (39%) perceived their weight as normal or low. Finally, among 152 participants who are classified as obese, 130 participants (86%) perceived themselves within lower-BMI categories, indicating a strong magnitude of underestimation.
Table 4 illustrates satisfaction with body weight according to the accuracy of perception. Ninety-one participants reported being satisfied with their weight despite underestimating their BMI. Eighty-one of those who were not satisfied with their body weight tended to overestimate it.
Table 5 and Figure 1 display the declared intention of participants concerning their body weight according to their BMI level. It can be observed that the majority of participants classified as overweight or obese intended to lose weight. However, 105 participants in these categories declared no intention to lose weight. Misconception was also observed among participants classified as normal weight or underweight, with 107 individuals indicating that they needed to lose weight—suggesting the presence of a distorted body image despite having either normal weight or being underweight.
4. Discussion
The current study was a cross-sectional investigation that aimed to assess how adults perceive their body weight, identify factors associated with wrong perceptions, and explore participants’ intentions regarding their body weight according to their level of BMI. More than half of the participants had a wrong perception of their body weight, with the majority tending to underestimate it. Female gender, being employed, practicing smoking or khat chewing, and being either underweight or obese were associated with higher frequencies of wrong perceptions of body weight. Underestimation of body weight appears to be associated with higher satisfaction levels with BMI despite having abnormal body weight. A misconception toward body weight is likely present and appears to influence participants’ intentions, with some of those who are overweight or obese reporting no intention to lose weight. In contrast, some participants with normal weight or underweight declared their intentions to lose weight, which might indicate the presence of a distorted body image.
The findings of the current study can be compared to similar local or international investigations. In a nationwide study conducted by Althumiri et al., which recruited a sample of 4709 participants from all regions of Saudi Arabia, it was reported that 42% of the sample misclassified their weight, with misclassification being higher among participants with abnormal body weight [28], similar to our findings. Additionally, Althumiri et al. concluded that misperception was associated with obesity, age group, educational level, and having a diagnosed chronic condition, which aligns with our findings—except for the impact of age and education, which were not significant in the current study. Nonetheless, Althumiri et al. did not detect a statistically significant association between gender and body weight misperception, which was identified as an important variable in the current study. Furthermore, in the current assessment, those who were retired or unemployed more frequently reported a wrong perception of body weight in comparison to employed or students. However, no association between weight perception and employment was detected in a similar Turkish study [29].
In a cross-sectional study that recruited a sample of 385 adolescents from Jazan, Saudi Arabia, who attempted to modify their body weight, it was reported that despite 55% of the adolescents having normal body weight, the majority of the sample were not satisfied with their weight (63%) [16]. This is similar to our findings, where almost 60% of the overall sample were not satisfied with their body weight across all BMI categories.
A low agreement between perceived body weight and actual BMI category was detected in the current study. This contrasts with the findings of a study conducted in Riyadh, Saudi Arabia, by Alhussaini et al. among female university students. Alhussaini et al. indicated that among the recruited female sample, the majority were between 18 and 29, and a kappa value of 0.635 was identified [30], compared to 0.22 detected in the current investigation. Nonetheless, the lower kappa value in the present study can be attributed to the broader demographic variability of the sample, which included different age groups, both men and women and various employment categories.
The frequency of body weight misperception was higher among females in the current study in comparison to males. This is similar to the findings of other studies which assessed perception of body weight according to gender. For example, in a Saudi study which involved a sample of 334 residents in Saudi Arabia, it was concluded that the prevalence of body weight misperception was higher among female [31], which is similar to the findings of the current study. Additionally, in another Nigerian study which involved a sample of 567 adults, it was also reported that body weight misperception was higher among females in comparison to males [32]. Similarly, studies that assessed body weight satisfaction and perception among younger populations suggested that females are more likely to be less satisfied by their body weight [33], and to overestimate their body weight [34].
The findings of the current study emphasize the importance of assessing the perception of body weight in addition to measuring weight and height and estimating BMI. This notion is supported by the findings of a large-scale Canadian study involving around 200,000 participants, where it was noted that being overweight or underweight was associated with lower life satisfaction, regardless of actual body weight [35]. The high prevalence of incorrect body weight perception detected in the current investigation was linked to improperly declared intentions concerning weight management among some participants. Additionally, some individuals reported being satisfied with their body weight despite having an abnormal weight.
In the current sample, underestimation of body weight was highly prevalent among overweight and obese individuals. This aligns with the findings of a Spanish study involving 1081 adult participants, where overweight individuals were more likely to underestimate their body weight [36]. Furthermore, a similar U.S. study that involved 744 adults and assessed the concordance between perceived body weight and actual BMI reported that, among participants with an overweight BMI, 32% perceived themselves as either normal or underweight, while among obese participants, 44% perceived themselves as either normal or overweight—indicating a non-negligible presence of underestimation [37].
In addition to the identified body weight underestimation among overweight and obese individuals, other demographic factors were associated with misperception. The minority of the current sample were either current or previous smokers (18%). Additionally, only 15% were either current or previous khat chewers. Nonetheless, the frequency of wrong perception of body weight was lower among those who were current or previous smokers or khat chewers in comparison to those who were never smokers or never khat chewers. These findings are different from the findings of another study which involved a sample of 53,447 Brazilian adolescents which concluded that the prevalence of body weight misperception (either underestimation or overestimation) was higher among adolescents who tried smoking [38]. Nonetheless, another Turkish study which involved a sample of 250 adults did not detect an impact of smoking on weight misperception [29].
It is possible to argue that the higher frequency of correct perception of body weight among smokers or previous smokers may be related to the association between smoking and body weight. The current evidence suggests that some individuals who are not satisfied with their body weight or perceive themselves as obese might tend to initiate smoking [39]. Additionally, smoking initiation is reported as a weight loss measure among some individuals [40,41]. Additionally, some who quit smoking might be at risk of weight gain after smoking cessation [42]. Studies that assessed body weight misperception according to khat chewing are lacking. However, khat chewing is a well-known risk factor for lower BMI among khat chewers [43,44]. Similarly, Khat is known for its impact on appetite suppression [45], and a higher risk of under nutrition [44].
The current study has multiple strengths and limitations. One strength lies in its ability to reach a sample with diverse demographic characteristics and correlate them with the likelihood of body weight misperception. This can inform future targeted interventions addressing abnormal body weight in the region and in similar local and international contexts. The main limitation relates to the inherent nature of self-reported weight and height which can be affected by higher risk of reporting bias in comparison to an objective clinical measurement. Another limitation is due to the nature of data collection process which was based on accessing the assessment tool in an online setting. This may reduce the ability of illiterate and older subjects to participate in the study which may have a potential impact on the generalizability of the study’s findings.
5. Conclusions
More than half of the participants had a wrong perception of their body weight, with the majority tending to underestimate it. Female gender, being employed, practicing smoking or khat chewing, and being either underweight or obese were associated with higher frequencies of incorrect body weight perception. The detected misperception—especially underestimation—might be linked to the likelihood of participants being in a precontemplation phase, resulting in limited intention to initiate healthy behavioral change toward weight management. The practical implications of these findings highlight the importance of incorporating weight perception assessment alongside actual BMI measurement in clinical settings. Early identification of such misconceptions and the application of appropriate cognitive therapy may be required to address body weight misperception.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Malnutrition 2024 Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition(accessed on 19 June 2025)
- 2World Health Organization Noncommunicable Diseases: Key Facts 2024 Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases(accessed on 19 June 2025)
- 3Bhattarai S.A.-O. Bista B.A.-O. Yadav B.K. Gynawali P. Poudyal A. Jha A.K. Dhimal M. Budhathoki S.S. Estimation of mean population salt intakes using spot urine samples and associations with body mass index, hypertension, raised blood sugar and hypercholesterolemia: Findings from STEPS Survey 2019, Nepal P Lo S ONE 2019171932620310.1371/journal.pone.0266662 PMC 900474635413065 · doi ↗ · pubmed ↗
- 4Thapsuwan S. Phulkerd S. Chamratrithirong A. Gray R.S. Jindarattanaporn N. Loyfah N. Thongcharoenchupong N. Pattaravanich U. Relationship between consumption of high fat, sugar or sodium (HFSS) food and obesity and non-communicable diseases BMJ Nutr. Prev. Health 20247788710.1136/bmjnph-2023-000794 PMC 1122128138966105 · doi ↗ · pubmed ↗
- 5Pressler M. Devinsky J. Duster M. Lee J.H. Glick C.S. Wiener S. Devinsky O. Dietary Transitions and Health Outcomes in Four Populations—Systematic Review Front. Nutr.2022974830510.3389/fnut.2022.74830535252289 PMC 8892920 · doi ↗ · pubmed ↗
- 6Billingsley H.E. Carbone S. Lavie C.J. Dietary Fats and Chronic Noncommunicable Diseases Nutrients 201810138510.3390/nu 1010138530274325 PMC 6213917 · doi ↗ · pubmed ↗
- 7Katzmarzyk P.T. Friedenreich C. Shiroma E.J. Lee I.M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries Br. J. Sports Med.20225610110610.1136/bjsports-2020-10364033782046 PMC 8478970 · doi ↗ · pubmed ↗
- 8Ejigu B.A. Tiruneh F.N. Katsuya T. The Link between Overweight/Obesity and Noncommunicable Diseases in Ethiopia: Evidences from Nationwide WHO STEPS Survey 2015 Int. J. Hypertens.20232023219985310.1155/2023/219985338023617 PMC 10667048 · doi ↗ · pubmed ↗