Using Implementation Theories to Tailor International Clinical Guidelines for Post-Stroke Gait Disorders
Salem F. Alatawi

TL;DR
This study explores how to adapt international stroke guidelines for gait disorders by considering factors like organizational settings, clinician expertise, and patient needs.
Contribution
The study introduces a systematic approach using implementation theories to tailor stroke rehabilitation guidelines for gait disorders.
Findings
21 recommendations reached consensus in phase one, with 14 rated highly applicable by physiotherapists.
Four key themes influencing tailoring were identified: organizational factors, clinician factors, patient factors, and research design.
No recommendations were rejected, and all were considered feasible with some adjustments.
Abstract
Background/objective: Tailoring involves adapting research findings and evidence to suit specific contexts and audiences. This study examines how international stroke guidelines can be tailored to address gait issues after a stroke. Methods: A three-phase consensus method approach was used. A 10-member health experts panel extracted recommendations from three national clinical guidelines in the first phase. In the second phase, 362 physiotherapists completed an online questionnaire to assess the feasibility of adopting the extracted recommendations. In the third phase, a 15-physical therapist consensus workshop was convened to clarify factors that might affect the tailoring process of the extracted recommendations of gait disorder rehabilitation. Results: In phase one, 21 recommendations reached consensus. In the second phase, 362 stroke physiotherapists rated the applicability of these…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
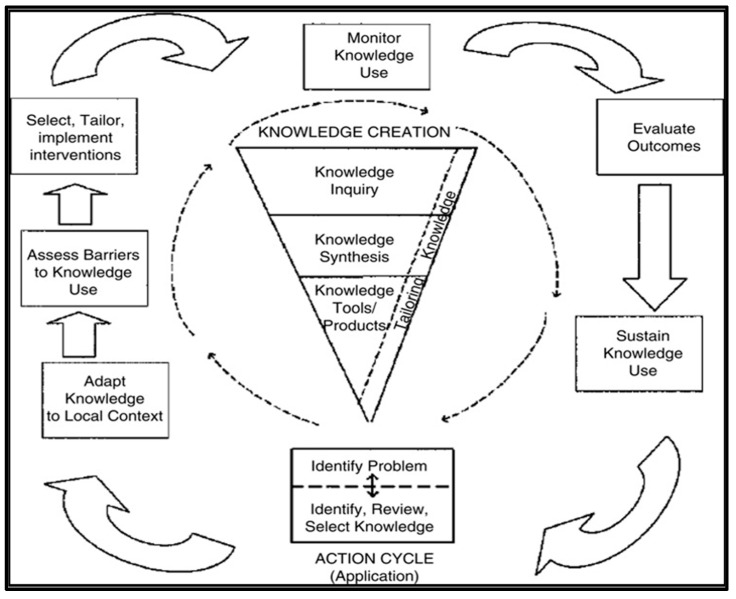 Figure 1
Figure 1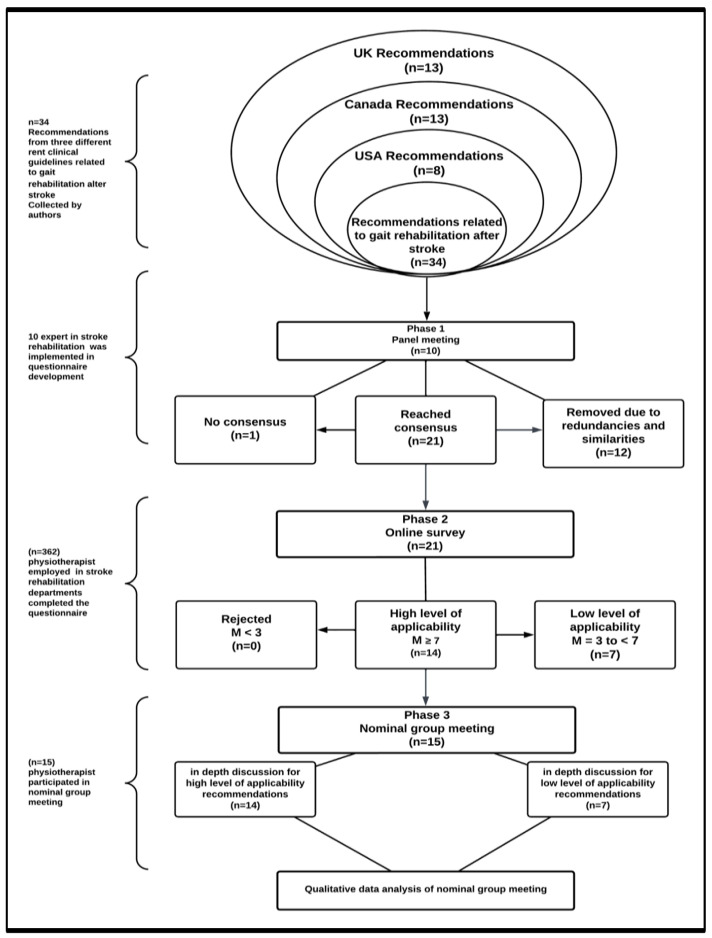 Figure 2
Figure 2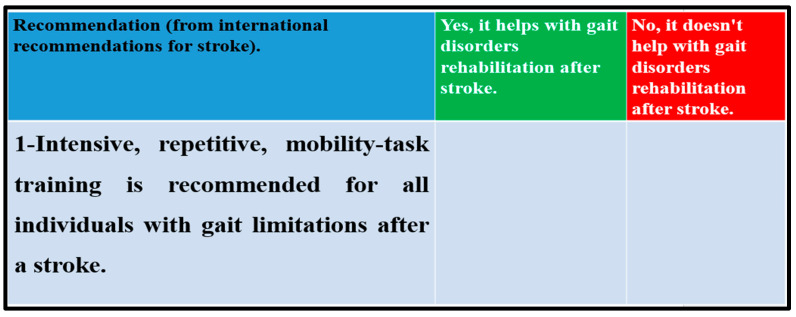 Figure 3
Figure 3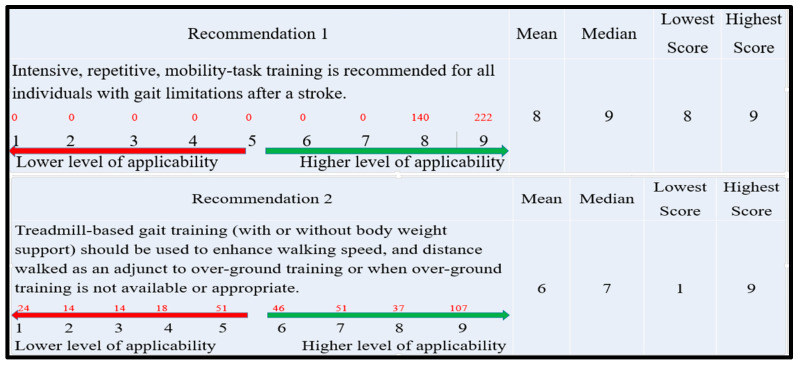 Figure 4
Figure 4- —deanship of research and graduate studies at the University of Tabuk
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical practice guidelines implementation · Health Systems, Economic Evaluations, Quality of Life · Health Policy Implementation Science
1. Introduction
Clinical practice guidelines (CPGs) are essential resources for healthcare professionals and patients aiming to make informed treatment decisions grounded in empirical research [1]. The development of these guidelines follows a structured process that includes several crucial steps: identifying the clinical problem, assembling a multidisciplinary team for guideline development, forming a systematic review team, and conducting a literature review to identify the most reliable research evidence and pertinent practice experiences [2].
Many countries have developed National Clinical Guidelines (NCGs) for stroke management. These guidelines are important for guaranteeing standardized care and enhancing outcomes for individuals affected by stroke [3]. Examples of countries that have established their guidelines include the United States (the American Heart Association (AHA) and the American Stroke Association (ASA)) [4,5], the United Kingdom (the National Institute for Health and Care Excellence (NICE)) [6], and Canada (the Canadian Stroke Best Practices Recommendations) [7]. However, these CPGs encompass a wide range of stroke-related issues, which may hinder the effective implementation of these guidelines in clinical practice [1,2].
Stroke is the leading cause of long-term disability and the second-leading cause of death worldwide [1]. Gait disorders often arise after a stroke and can significantly affect an individual’s mobility, independence, and overall quality of life. It is estimated that nearly 60–80% of stroke survivors experience gait disorders [2].
Stroke is the leading cause of long-term disability and the second-leading cause of death worldwide [8]. Gait disorders are among the most common clinical conditions that arise after a stroke [8]. Nearly 60–80% of individuals who have suffered a stroke experience impairment in their gait [8]. However, despite national guidelines providing evidence for healthcare interventions addressing gait disorders post-stroke, their practical implementation often falls short [1]. Consequently, a gap exists between the development of evidence-based best practices and their implementation in everyday clinical settings.
The vascular topography of acute stroke refers to how blood vessels are affected and which parts of the brain suffer from reduced blood flow or bleeding. Understanding this topography is essential for evaluating the stroke’s impact on motor functions, especially regarding gait disorders [9]. Gait disorders, such as hemiparesis, ataxia, and bradykinesia, are frequently observed in individuals after a stroke. However, there is an intricate connection between the vascular topography of acute stroke and these gait disorders [9].
Understanding the affected areas of the brain can guide treatment strategies and enhance recovery outcomes for individuals facing gait issues related to stroke. A clinical report identified lacunar stroke as the primary subtype of infarction occurring in the territory of the posterior cerebral artery (PCA) [9]. The study also found that certain symptoms were more common in stroke patients with PCA infarction than in those with ischemic strokes from the middle cerebral artery (MCA) and anterior cerebral artery (ACA) [9].
The NCGs provide substantial evidence regarding gait disorders following a stroke. However, implementing gait CPGs can be challenging for several reasons [1,2]. The authors [10,11,12] suggest that many guidelines are not adequately tailored to meet the specific needs of individual patients. They point out that variability in factors such as age, mobility levels, and specific injuries necessitates personalized approaches, which standardized guidelines often lack.
Implementing international clinical guidelines can be challenging due to various factors. The literature identifies several common challenges to the successful implementation of these guidelines, including variability in healthcare systems, cultural differences, resource limitations, resistance to change, lack of awareness or knowledge, training and education needs, inconsistent interpretation, patient engagement, and issues related to policy and funding [12,13]. The authors concluded that overcoming these challenges requires a multi-faceted approach that includes education, resource allocation, and the promotion of a culture of evidence-based practice. Additionally, collaboration among stakeholders—such as healthcare providers, policymakers, and patients—is crucial for effective implementation [12,13].
These challenges may redirect focus to national clinical recommendations, which offer a detailed examination of the evidence supporting healthcare interventions [11,12,13]. Researchers have noted a possible delay in adherence to these recommendations, despite the growing amount of data available [8,9,10]. Consequently, there exists a gap between the evidence currently available and its application in daily practice [12,13,14].
Implementation research explores strategies that connect evidence with practice, thereby improving the relevance and applicability of this evidence [14]. Current literature indicates that our understanding of the methods for implementing evidence-based practices might be limited [14]. Evidence implementation frameworks are increasingly available, and this field is progressing rapidly. Notable examples of these frameworks include the Ottawa Model of Research Use [15], PARIHS [16], and KTA [17].
The Knowledge-to-Action (KTA) framework encompasses both knowledge creation and action (Figure 1). This theoretical framework utilizes the knowledge funnel/triangle as a metaphor for the process of knowledge filtration, also referred to as tailoring. Throughout the knowledge creation process, tailoring results in synthesized information that may be more advantageous to end consumers. According to Graham et al. (2006) [17], tailoring facilitates collaboration between researchers and knowledge users, allowing them to share insights and develop solutions together [17]. Furthermore, this approach has the potential to impact professional practice.
The KTA framework effectively demonstrates how national clinical guidelines can function as a funnel or triangle for knowledge creation. However, tailoring—an essential element of knowledge creation within the KTA framework—has proven to be a significant challenge. Consequently, the primary aim of this study was to employ a technique that enhances understanding of the tailoring process and its practical application in stroke rehabilitation. The research question looked at how “tailoring” can be used in the funnel structure of the KTA framework to create recommendations based on different international clinical guidelines for gait disorders after a stroke.
2. Methods
A mixed-method study was used. A consensus approach was employed to explore tailoring within the Knowledge-to-Action (KTA) framework. The methodology consisted of three phases: a panel, a survey, and a nominal group meeting (NGM) (Figure 2).
The decision to use the KTA framework over other implementation theories stems from its inclusion of the key concept of tailoring in the knowledge creation process. The consensus approach was selected to deepen the understanding of how tailoring functions and its relevance in stroke rehabilitation, while also exploring the various factors that affect the implementation process.
The continuation of the study received approval from the local research ethics commission (LREC) at the University of Tabuk. All participants provided informed consent before engaging in the study.
2.1. Phase 1: The Panel Phase
The authors independently collected the post-stroke gait disorder recommendations from the US, UK, and Canadian stroke guidelines. They collected 34 recommendations from the US, UK, and Canadian stroke guidelines for panel voting to determine their applicability to stroke-related gait disorder rehabilitation.
2.1.1. The Sample Size
The panel group consisted of 7 clinicians and 3 academics; all recruited from local hospital systems and universities. The inclusion criteria required that participants be either physiotherapists with expertise in stroke rehabilitation working in hospitals or academics who possess extensive experience in stroke rehabilitation and integrate it into their university curriculum.
2.1.2. The Procedure
A projector displayed all recommendations during the panel meeting. Participants were instructed to organize the recommendations as needed before voting on their relevance and suitability for stroke rehabilitation using a two-point Likert scale: “Yes, it helps with gait disorders rehabilitation after stroke” and “No, it doesn’t help with gait disorders rehabilitation after stroke”.
2.1.3. Data Analysis
Any recommendation that received at least 70% approval from the votes was included, while those that did not meet this threshold were excluded based on the consensus findings [18] (Figure 3). The survey for the next phase was developed based on the consensus findings.
2.2. Phase 2: The Survey
The goal of this survey was to find out what specialized stroke physiotherapists think about how realistic it is to apply the agreed-upon recommendations from Phase 1 (the panel meeting) in actual stroke rehabilitation settings.
2.2.1. The Sample Size
The online survey was distributed to 598 participants. The survey exclusively comprised physiotherapists in Saudi Arabia who met the eligibility criteria of having a minimum of one year of experience in stroke rehabilitation. The study excluded physiotherapists who were not actively involved in stroke rehabilitation practice.
2.2.2. The Procedure
Each recommendation was rated on a Likert scale from 1 to 9, with 1 indicating the lowest level of agreement and 9 indicating the highest level of agreement [19] (Figure 4). We distributed questionnaires generated by Google Forms to Saudi physiotherapists via social networks to increase the number of eligible responses. Participation in the questionnaire required an email address. Consequently, all participants were sent an invitation, a cover letter, and a form of consent.
2.2.3. Data Analysis
The Statistical Package for the Social Science version 25 for windows (SPSS Version25; IBM, Armonk, NY, USA) was employed to calculate the frequency, median, and interquartile range for each recommendation. The absence of consensus made recommendations with a median score below 3 unacceptable. Recommendations with a median score of three or above were chosen for the nominal group discussion (phase 3) [19].
2.3. Phase 3: Nominal Group Meeting
This phase involved analyzing the survey results from phase 2 to discuss participants’ ratings of the recommendations. The objective was to identify and deliberate on recommendations that achieved consensus, defined as a median score of 7 or above, as well as those that did not reach consensus, indicated by a median score below 3. Additionally, it is important to explore why some recommendations attained consensus despite exhibiting significant score variations (for instance, with a lowest score of 1 and a highest score of 9), while others showed only minor variations (for example, with a lowest score of 8 and a highest score of 9).
2.3.1. The Sample Size
During this phase, 15 stroke rehabilitation physiotherapists who had completed the survey (phase 2) expressed interest in a nominal group meeting.
2.3.2. The Procedure
Before starting the discussion, the questionnaire findings were shown on screen. The NGM guide featured open-ended and probing questions specifically designed to align with the study’s objectives. These questions aimed to gather essential information required to achieve the study’s goals (Appendix A). Fifteen stroke rehabilitation physiotherapists who completed the questionnaire expressed interest in an NGM to discuss Phase 2’s findings.
Braun and Clarke’s [20] thematic analysis is performed manually and comprises six distinct phases: (1) familiarization, which entails actively reading the data to understand its depth and breadth; (2) coding, in which the researcher identifies compelling and significant pieces of data that may contribute to theme development; (3) linking the identified themes to all coded data; (4) examining the coded data to develop cohesive and refined themes; (5) identifying topic titles along with the associated data; and (6) reporting, which involves writing the final analysis and detailing the identified themes (Appendix B).
2.3.3. Data Analysis
The transcripts were analyzed for themes. Two researchers, focusing on data coding, carefully reviewed the transcriptions from the NGM. They entered the transcriptions in Excel files for the coding process. Following this, the researchers independently identified the main themes and subthemes.
To create initial themes and subthemes, begin by identifying patterns of meaning within the codes. Establish subthemes. Next, analyze the subthemes to identify overarching concepts. Finally, verify the proposed themes against the dataset to assess how accurately they represent the data. Participant numbers (P#s) were assigned to maintain anonymity.
3. Results
Understanding physiotherapists’ viewpoints, assessing their ratings of the recommendations to reach consensus, and analyzing the discussions from the notional group meeting may aid in identifying potential barriers and supports to consider during the implementation of the final recommendation regarding gait disorders after stroke.
3.1. Result of Phase 1: Panel Meeting
We provided a comprehensive set of 34 recommendations for panel voting to determine their applicability to stroke-related gait disorder rehabilitation. Twelve recommendations were eliminated due to their duplication with the stroke recommendations from the US, UK, and Canada. Table 1 displays the characteristics of the panel meeting participants.
After eliminating duplicate recommendations, a total of 21 recommendations achieved a consensus level (70%), and one recommendation fell short of achieving a consensus level based on the panel’s voting.
3.2. Result of Phase 2: Online Survey
In this phase, out of the 598 participants in the survey, 362 provided complete data (Table 2). In total, 14 of 21 stroke rehabilitation gait recommendations were highly useful (with a median score of 7 or higher). Only seven recommendations obtained a median score of 3–7, indicating minimal applicability. No recommendation was rejected (Appendix C).
3.3. Results of Phase 3: Nominal Group Meeting (NMG)
Fifteen stroke rehabilitation physiotherapists (n = 15) who completed the survey in phase 2 expressed interest in participating in a nominal group meeting. The characteristics of the participants in this phase are presented in Table 3.
In this phase, we analyzed the online survey findings that had previously been disrupted in phase 2. Four main themes and nine subthemes were derived from the NMG (Table 4). This analysis aims to clarify why some recommendations reached a consensus level while others did not. This phase’s findings may shed light on why participants modified the recommendations before implementing them in their practice.
3.3.1. Organizational Factors
All participants agreed that organizational issues could impact the tailoring of rehabilitation evidence for stroke gait disorders. In subtheme 1 (clinical context), participants said that the resources available at work—like money, staff, time, and equipment—were very important in deciding whether to use rehabilitation recommendations for stroke gait disorders in their everyday jobs. They noted that the resources of healthcare facilities could influence the implementation of these recommendations.
“I recognize the significance of this recommendation for stroke gait rehabilitation; however, my department does not have the necessary equipment to implement it. I voted 5 out of 9.”
We noted a considerable consensus among recommendations that did not require equipment, in contrast to those that did. For example, several recommendations received a median score of 9.
“This recommendation does not require any equipment; it depends instead on the professional’s skill. In my opinion, these comments may help clarify the rationale for achieving a median value of 9.”
Participants concurred that organizational culture (subtheme 2) significantly influences the tailoring of clinical practice recommendations. Key elements of this culture include strong leadership, staff training, effective communication among healthcare professionals, teamwork, and feedback from clinical experiences.
“I rated some recommendations based on departmental teamwork and communication. This fosters knowledge exchange, which contributes to the development of optimal practices.”
Participants in subtheme 3 (Organizational policies) emphasized a conflict between the desire to tailor recommendations and the need to adhere to organizational policies. While participants believe that personalized recommendations could benefit their patients, this conflict may impede the practical implementation of those suggestions, as they may not conform to established organizational guidelines.
“In my opinion, certain recommendations may be feasible and could be implemented”. However, rigid organizational policies can obstruct the effective application of evidence in real-world clinical settings.”
3.3.2. Individual Clinician Factors
Participants emphasized the importance of considering individual factors when tailoring recommendations for rehabilitating gait disorders in stroke patients. They noted that their knowledge, skills, experience, and training significantly influenced how they ranked the recommendations in the survey (Phase 2). This reliance on personal expertise may explain the variability in consensus ratings among participants regarding specific recommendations. One participant remarked,
“Individuals lacking sufficient expertise, practical experience, skills, and training may have a limited understanding of recommendation effectiveness in producing favorable results with patients.”
Those in the “clinical experience and expertise” group said that their past use of the recommendations and their understanding of how to use them in real-life situations influenced their choice to apply them in helping patients with stroke-related walking problems. As one participant stated,
“If the recommendation is not being utilized, it is unlikely that one would use it on a daily basis.”
3.3.3. Patient Factors
The third theme explored patient variables that could potentially impact recommendations for the rehabilitation of gait disorders following a stroke. The first subtheme focused on how various health conditions can affect clinical practice recommendations. Participants noted that different medical concerns and comorbidities can influence the tailoring of recommendations. One participant stated,
“Before considering the implementation of any recommendations for my patient, I took into account medical problems related to strokes, as well as memory and cognitive issues that affect individuals who have experienced a stroke.”
Participants in the second subtheme highlighted the importance of patient engagement and shared decision-making in physiotherapy practice. They emphasized that when physiotherapists engage in shared decision-making with patients, it can lead to improved health outcomes, increased patient satisfaction, and more personalized treatment approaches. One participant remarked,
“When deciding which recommendations to incorporate into my practice, I considered how I could effectively engage with my patients in meaningful discussions and provide clear explanations about this recommendation to ensure that interventions align with their values, preferences, and goals.”
3.3.4. Other Factors
The findings suggest that additional factors may influence participants’ decisions regarding the implementation of certain recommendations in their clinical practice. The first subtheme is titled “Research of RCT Design”. Participants noted that research methodologies, such as randomized controlled trials (RCTs), may not be applicable to all patients and can be difficult to implement. The stringent protocols of RCTs can limit the ability to tailor interventions to align with each patient’s specific needs, preferences, and treatment responses, ultimately diminishing their effectiveness. Several participants talked about the importance of employing qualitative research methods to collect empirical data from healthcare professionals, patients, and caregivers involved in rehabilitation for gait disorders following a stroke. One participant noted,
“The strict inclusion and exclusion criteria of a randomized controlled trial (RCT) may exclude the patients I am trying to treat. Therefore, increasing the use of qualitative methods may be beneficial.”
Client-related factors associated with the stages of stroke also affected how participants tailored their recommendations (the second subtheme). In the initial phase of a stroke, the primary focus is on preventing further complications. In contrast, patients in the later stages may require more intensive and specialized rehabilitation aimed at addressing functional impairments. One participant explained how this insight could influence the tailoring of specific clinical practice recommendations, stating,
“For me, in the early stages, I occasionally focused on the prevention of secondary complications, whereas in the late stages, I used to focus on the improvement of motor function.”
4. Discussion
This study examined the factors that may affect the tailoring of gait disorder recommendations based on international stroke guidelines. Several factors require investigation to evaluate their impact on the effectiveness of this tailoring process:
4.1. Organizational Factors
The findings indicate that the implementation of recommendations within a specific organization relies on several key factors: funding, staffing, time management, leadership, ongoing training and education, communication, and policies. These elements significantly influence the range of professional activities permitted within the organization. The results support previous research, which demonstrates the value of considering specific requirements, priorities, regulations, and resources when customizing recommendations for clinical practice [21,22]. Prior studies suggest that assessing user perspectives, available resources, daily routines, local leadership, opinion leaders, and systems is essential for effectively adapting knowledge to local contexts [21,22]. This research highlights that successful implementation of changes is more likely in organizations that prioritize evidence-based planning, promote open discussions, and allocate resources effectively.
4.2. Individual Clinician Factors
The findings of this study indicate that specific clinician characteristics significantly influence the tailoring and implementation of evidence in clinical settings. The effectiveness of tailored recommendations in clinical practice is heavily dependent on clinical skills, experience, knowledge, beliefs, and attitudes [14,23,24]. These factors are essential for integrating recommendations into patient-centered healthcare
Consistent with this study’s findings, several researchers argue that involving end users in the tailoring of evidence-based interventions to fit their specific context has proven to be effective [14,22,23]. Additionally, when end users are not engaged in the tailoring process, it often results in inadequate tailoring rates and negatively affects outcome quality [23].
This research emphasizes the value of end-user feedback in the tailoring process [14,23]. By exploring professional attitudes, organizations can gain a deeper understanding of how to implement and sustain evidence-based practices [14,23,24]. Pereira et al. demonstrated that modifying implementation strategies to address locally recognized barriers and facilitators can enhance the acceptance of recommendations and improve care interventions [22].
4.3. Patient Factors
This study found that the physical, cognitive, and psychological abilities of stroke patients significantly influenced rehabilitation recommendations for gait disorders. The evidence suggests that individuals with multiple comorbidities or complex medical histories may require a personalized approach, as national recommendations may not fully address their specific clinical situations [23,24]. Several authors emphasized the importance of thoroughly evaluating potential treatment options and their feasibility for individual patients before applying recommendations in clinical practice [25]. Additionally, the study’s findings highlighted that patient engagement is crucial in the physiotherapists’ decision-making process regarding the application of national recommendations. Aligning evidence-based practices with the patient’s goals, values, and preferences is essential for effective implementation. Shared decision-making is vital to ensure that the treatment plan aligns with the patient’s priorities [25,26].
4.4. Other Factors
Feasibility refers to the practicality of proposed evidence for implementation, specifically how well it aligns with current practices [27]. The study’s results showed that the practicality of the recommendations from a randomized controlled trial (RCT) significantly impacted how they were used to treat walking problems after a stroke [26,27,28]. This challenge underscores the concept of feasibility. The research suggested that physicians may need to incorporate information from various sources, such as observational studies, patient registries, and real-world evidence, alongside RCTs to better tailor treatment plans for stroke management [27,28]. Furthermore, employing adaptive trial designs, personalized outcome measures, and considering patient preferences and goals can help bridge the gap between RCT evidence and the unique needs of stroke patients [25,26,27].
Therefore, recommendations must be tailored to fit within existing delivery models in the targeted setting [26]. The importance of feasibility, in terms of practical and organizational factors, has been emphasized as crucial for effectively translating research findings into sustainable healthcare delivery and improved patient outcomes. By focusing on feasibility, we can ensure the optimal implementation of evidence. However, some authors have expressed concerns about the difficulty of maintaining accuracy when adapting evidence-based principles to specific settings [26,28]. Excessive modification of these recommendations can result in a loss of their original meaning, potentially negatively impacting the quality of care and its outcomes.
5. Study Limitations
All participants in this study were Saudi physiotherapists, indicating that their expertise is specific to the context of Saudi healthcare. As a result, the research findings may only be applicable to similar environments. The primary objective of the study was to tailor stroke guidelines to address specific issues, such as gait impairments, rather than to generalize findings statistically. Furthermore, rehabilitation center managers played a role in recruiting stroke physiotherapists during the data collection phase, which may have created a sense of obligation for participants to take part in the study. Communication with stroke physiotherapists also required prior approval from the management of the rehabilitation centers. Another limitation of this study is its inability to evaluate how well individuals and organizations adhere to the established recommendations. There is a need for international collaboration.
6. Conclusions
The KTA framework incorporates tailoring as a key element of its funnel structure. The key to successful tailoring is that there is a match between the expected research findings, the targeted knowledge users, and the knowledge translation strategies selected. Furthermore, essential issues should be explored before tailoring recommendations from international clinical guidelines to a specific issue. This includes examining organizational, individual, and patient factors, engaging end users, and assessing feasibility. This study demonstrates how a systematic approach, such as the consensus method, can effectively facilitate the conversion of research knowledge into practical applications. However, it is necessary to account for various factors to successfully tailor international recommendations that align with real-world practices.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guerra-Farfan E. Garcia-Sanchez Y. Jornet-Gibert M. Nunez J.H. Balaguer-Castro M. Madden K. Clinical practice guidelines: The good, the bad, and the ugly Injury 202354 S 26S 2910.1016/j.injury.2022.01.04735135686 · doi ↗ · pubmed ↗
- 2Nilsen E.S. Myrhaug H.T. Johansen M. Oliver S. Oxman A.D. Methods of consumer involvement in developing healthcare policy and research, clinical practice guidelines and patient information material Cochrane Database Syst. Rev.20063 CD 00456310.1002/14651858.CD 004563.pub 216856050 PMC 6464810 · doi ↗ · pubmed ↗
- 3Institute of Medicine (US) Committee on Clinical Practice Guidelines Guidelines for Clinical Practice: From Development to Use Field M.J. Lohr K.N. National Academies Press Washington, DC, USA 199225121254 · pubmed ↗
- 4American Heart Association Available online: https://www.heart.org/(accessed on 25 May 2025)
- 5American Stroke Association Available online: https://www.stroke.org/en/(accessed on 25 May 2025)
- 6National Institute for Health and Care Excellence Available online: https://www.nice.org.uk/(accessed on 25 May 2025)
- 7The Canadian Stroke Best Practices Recommendations Available online: https://www.strokebestpractices.ca/(accessed on 25 May 2025)
- 8Duncan P.W. Zorowitz R. Bates B. Choi J.Y. Glasberg J.J. Graham G.D. Katz R.C. Lamberty K. Reker D. Management of Adult Stroke Rehabilitation Care: A Clinical Practice Guideline Stroke 200536 e 100e 14310.1161/01.STR.0000180861.54180.FF 16120836 · doi ↗ · pubmed ↗