Health Education in Mass Gatherings: A Scoping Review to Guide Public Health Preparedness and Practice
Rania Zaini, Altaf A. Abdulkhaliq, Saleh A. K. Saleh, Heba M. Adly, Salwa Abdulmajeed Aldahlawi, Laila A. Alharbi, Hani M. Almoallim, Nahla H. Hariri, Ismail Ahmad Alghamdi, Majed Sameer Obaid, Amar Mohammad A. Alkhotani, Aous Sami Hayat Alhazmi, Anas A. Khan, Fahad A. Alamri

TL;DR
This review explores how health education impacts attendees at mass gatherings like pilgrimages and sports events, finding that tailored, accessible education improves outcomes.
Contribution
The study provides a comprehensive scoping review of health education effectiveness in mass gatherings, emphasizing tailored delivery and language.
Findings
Health education effectiveness varies in mass gatherings, with most studies agreeing it should start before events and continue during.
Tailored health education in local languages improves acceptability and outcomes among attendees.
Evidence is inconsistent, but suggests online and offline delivery methods should be available based on participant preferences.
Abstract
Objectives: In view of a lack of evidence on the subject, we aimed to perform a scoping review to understand the impact of health education among people attending mass gatherings. Methods: We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Guidelines. PubMed, EMBASE, Scopus, and Cochrane Library were searched from inception to March 2025 to identify eligible studies. Observational and interventional studies that reported the impact of health education on any health-related outcome among those attending a mass gathering were considered. A narrative synthesis of review results was performed to gather evidence. Recommendations were framed in the context of this evidence. Results: Of the 1731 records, only 17 studies met the inclusion criteria. These included cross-sectional (n = 10), pre-post design (n = 3),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
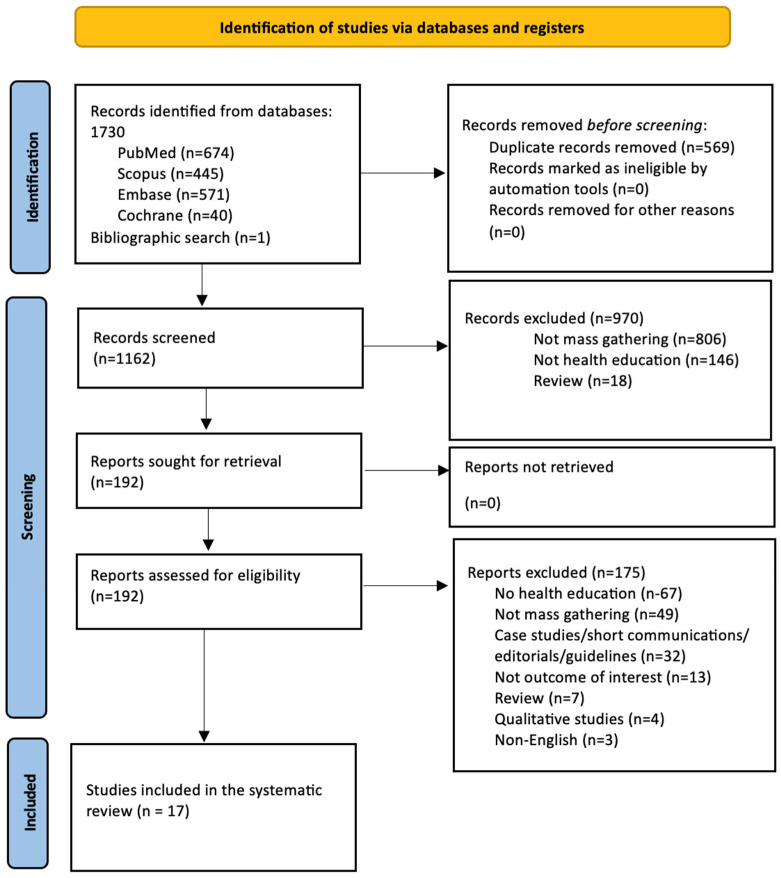 Figure 1
Figure 1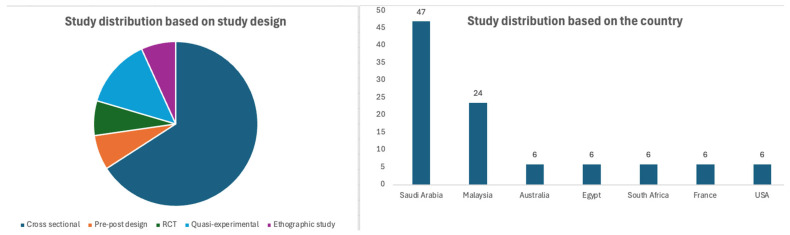 Figure 2
Figure 2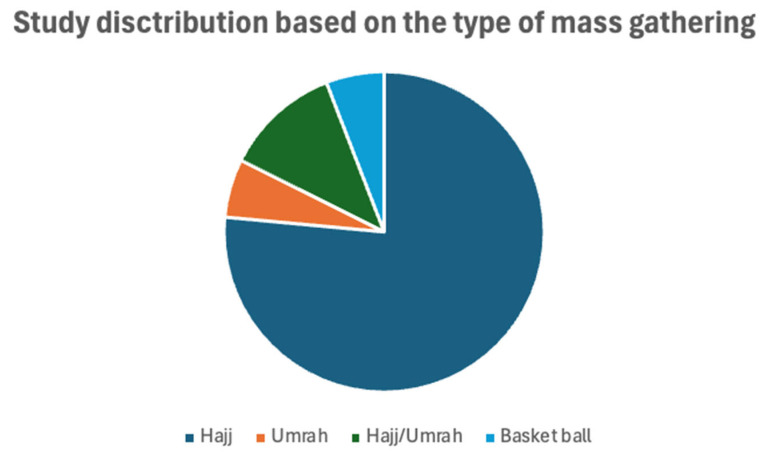 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTravel-related health issues · School Health and Nursing Education · Viral Infections and Vectors
1. Introduction
Events grounded in cultural, religious, social, or recreational traditions are integral to human society and are often classified as mass gatherings. The World Health Organization (WHO) defines mass gatherings as “an organized or unplanned event where the number of people attending is sufficient to strain the planning and response resources of the community, state, or nation hosting the event” [1]. Similarly, the Center for Disease Control and Prevention (CDC) Yellow Book describes it as “large numbers of people (>1000) at a specific location, for a specific purpose” [2]. Practically speaking, a mass gathering can be any assembly of people large enough to strain local resources [3].
Despite their positive societal and cultural value, mass gatherings pose a significant public health challenge due to the potential for infectious disease outbreaks and other health-related complications [4]. The convergence of large populations in confined or shared spaces during mass gatherings significantly increases health hazards. Outbreaks of respiratory infections, foodborne illnesses, heat-related illnesses, injuries, and exacerbation of non-communicable diseases have all been reported during such events [5,6]. Mass gatherings pose a significant infectious disease risk, with 72 respiratory outbreaks linked to such events from 2005–2014, with over 840,000 respiratory infection cases tied to the Union of European Football Associations (UEFA) Euro 2020 games [7], and recent measles surges in South Korea linked to international events [8]. These trends highlight the urgent need for targeted public health interventions and education. These challenges are further exaggerated by inadequate sanitation, poor crowd control, limited access to healthcare services, and the presence of high-risk groups such as the elderly or immunocompromised individuals [9,10]. To mitigate these risks, several preventive and public health strategies have been recommended, including the promotion of hand hygiene, mask wearing, environmental sanitation, vaccination, and crowd health surveillance [11,12,13,14].
Health education has emerged as a particularly important and cost-effective measure [11,14]. It plays a pivotal role in empowering individuals with the knowledge and motivation needed to adopt safer health practices, adhere to guidelines, and respond effectively during emergencies [15]. Health education influences health behavior, and its impact can be understood through various frameworks, one of which is the health belief model (HBM). The HBM posits that individuals’ engagement in health-related behaviors is determined by their perceptions of susceptibility, severity, benefits, and barriers, along with cues to action and self-efficacy [16,17,18]. Focusing on health education and health-related behaviors is especially important for mass gatherings due to the increased risk of infectious disease transmission in crowded, diverse settings [19]. In the context of mass gatherings, health-related behavior can be considered the first line of defense against infectious disease, particularly when medical interventions are limited [17]. Applying behavioral models like the HBM helps tailor messages so that they include psychological factors, such as perceived risk and self-efficacy, making interventions more effective [16,18]. Tailoring education to these psychological constructs increases the likelihood of meaningful behaviour change. Applying such a model ensures that interventions are not only informative but also motivational and behaviorally grounded [19,20], particularly at mass gatherings.
Although health education is widely recognized as a cornerstone of disease prevention, there is limited consolidated evidence evaluating its effectiveness in the specific context of mass gathering events. Most available studies and existing systematic reviews focus on broader intervention strategies, with health education often being included as part of a larger public health package rather than as an isolated component [11,14,21]. This lack of focused analysis limits our understanding of the standalone effectiveness of health education, particularly in the unique context of mass gatherings. To date, there is no comprehensive literature evidence that isolates and evaluates the specific contributions of health education in these settings. This scoping review addresses that gap by systematically mapping the available evidence on health education as an independent preventive measure at mass gatherings, offering novel insights into its role, implementation, and impact. Scoping reviews are particularly valuable for mapping the breadth and depth of existing literature on a topic, especially when the area is complex or not well defined. They help identify research gaps, clarify key concepts, and inform future studies or policy decisions by synthesizing diverse sources of evidence [22,23].
Given the increasing scale and frequency of mass gatherings, increased infections and antibiotic resistance worldwide and the health challenges they pose, it is essential to critically examine the available evidence regarding the role of health education. This information will help us planning the future events and prevention of mass gathering-associated health hazards. Therefore, this scoping review aims to explore and map the existing literature on the effectiveness of health education during mass gatherings, thereby identifying research gaps and guiding future public health policies and interventions.
2. Materials and Methods
This scoping review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Guidelines [24]. The review was conducted following the Arksey and O’Malley’s scoping review framework which outlines five key stages in its process, with an optional sixth stage: (1) research question identification, (2) relevant study identification, (3) study selection, (4) data charting, (5) results reporting, and (6) consultation of an expert [25]. The protocol for this study is registered in PROSPERO with a registration number: CRD42025637008.
2.1. Stage 1: Identifying the Research Question
The research question was identified following a thorough preliminary literature review, which in turn emphasized the lack of evidence or consensus on the impact of health education among participants attending a mass gathering. The research question was clearly defined with the concept of interest (impact of health education on health outcomes), target population (participants attending any mass gathering), and context (any setting irrespective of purpose, geographical area, and type of participants).
2.2. Stage 2: Identifying Relevant Studies
A comprehensive search of the literature was conducted in PubMed, EMBASE, Scopus, and Cochrane library databases from inception to March 2025 to locate all relevant studies. The search terms entered were selected from Medical Subject Heading (MeSH) terms and the existing literature. The keywords identified were “mass gathering”, “mass event”, “crowd”, “hajj”, AND “health education”, “medical education”, “health promotion”. We also manually searched the bibliographies of relevant reviews to identify additional relevant studies. Detailed search strategy used in various databases is provided in Supplementary File S1.
2.3. Stage 3: Study Selection
This review employed Joanna Briggs Institute’s (JBI) framework for scoping reviews to match the study selection with the review question [26]. We included studies that met the predefined eligibility criteria.
2.4. Study Eligibility Criteria
2.4.1. Population
The study population included any adult patients (aged > 18 years) attending any kind of mass gathering irrespective of their gender and ethnicity. We did not apply any other restriction to the population.
2.4.2. Concept
The concept for this review was focused on health education in any of its forms provided to those attending a mass gathering. We considered all types of health education strategies that can be delivered through any medium of communication, such as online, offline, paper, videos, or a combination, through any method of delivery, such as in-person, virtual, smartphone, computer, or a combination. Any health-related outcomes, including knowledge, attitude, and practice, resulting from receiving health education were considered an outcome of interest. Studies that focused on basic education or knowledge without discussing health education were excluded. However, we did not consider studies that reported outcomes from those who provide the services, instead of those attending the mass gathering.
2.4.3. Context
We considered any settings where a mass gathering can occur, including but not limited to religious events, sports, festivals, concerts, school events, and university events. We excluded those studies which involved individual enrolment without a mass gathering. Further, we did not consider interventions that were based on personal rather than preventive measures during mass gatherings.
2.4.4. Type of Studies
We included all types of observational and interventional studies. Only studies published in the English language were considered for this review. Narrative or systematic reviews, conference abstracts, unpublished studies, and letters to the editor were excluded from this review. Qualitative studies were also excluded as our primary focus was on assessing the effectiveness and implementation of health education interventions, which are more directly addressed through quantitative and mixed-methods research.
Following the database search and removal of duplicates, the remaining studies were screened for titles and abstracts, and the full texts were evaluated for relevant citations using predefined inclusion criteria by two independent reviewers (A.A.A., and L.A.A.) from the research team. Disagreement was resolved through discussion or, when necessary, by a third independent evaluator (A.M.A.A. or A.A.K.).
2.5. Stage 4: Charting the Data
A pre-designed standardised data extraction form created in Microsoft Excel was used to avoid bias in the data abstraction process. The data were extracted by two independent authors (A.A.A., and L.A.A.) after verifying the data in the extraction form for its correctness and consistency. The collected data includes first author’s last name, country, year of publication, type of mass gathering, characteristics of participants, type of education, mode of education, and the outcomes. To ensure inter-reviewer reliability, data extraction was conducted independently by two reviewers using a standardized form. Any discrepancies were resolved through discussion and consensus, with a third reviewer (A.M.A.A. or A.A.K.) consulted when needed. This process helped minimize bias and enhance the consistency and accuracy of the extracted data.
2.6. Stage 5: Collating, Summarising, and Reporting the Results
Each eligible study was scrutinized for impacts of health education as a whole or as part of a preventive strategy and benefits among the patients attending a mass gathering. We considered studies that reported any health-related outcome. Studies lacking relevant information related to the research topic were excluded. All evidence extracted using this systematic process was summarized narratively and presented in a tabular form according to the health education strategy and its impact on health among participants who attended the mass gathering. Unfortunately, the high heterogeneity in study objectives, intervention adopted, mode of delivery, designs, and reported outcomes among the studies made it difficult to perform a statistical analysis, and it forced us to a narrative synthesis. Broadly, the outcomes were classified under the umbrella of improvement in knowledge, attitude, and practice and then detailed as per the individual outcomes. The available effect measures (such as percentage [%], mean difference [MD], or odds ratio [OR]) were summarized with a 95% confidence interval [CI] and p-value for significance.
3. Results
3.1. This Study Selection Process
The literature search yielded a total of 1730 articles and one additional study from bibliographic search. After removal of duplicates (n = 569) and exclusion of 970 non-relevant articles during the initial screening, 192 relevant articles were considered for full-text screening. Of these, 175 studies were excluded for appropriate reasons. Finally, only 17 studies [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] were considered for this review. The PRISMA flow diagram of the study selection process is provided in Figure 1. The detailed reasons for exclusion of individual studies are provided in Supplementary File S2.
3.2. Characteristics of Included Studies
Among the 17 included studies, 10 (58%) were cross-sectional studies. In the remaining studies, 3 (18%) were pre-post design, 1 (6%) was a randomized controlled trial (RCT), 2 (12%) were quasi-experimental, and 1 (6%) was an ethnographic study. All of these studies were published between 2008 and 2023. The country-wise distribution found that most studies were from Saudi Arabia (n = 8), followed by Malaysia (n = 4). The sample size varied from 57 to 1221 in the included studies. The studies included participants who attended hajj (n = 13), umrah (n = 1), hajj/umrah (n = 2), and basketball games (n = 1). Detailed information on the included studies is provided in Table 1. The study distribution, based on the study design, country, and the type of mass gathering, is presented in Figure 2 and Figure 3.
3.3. Characteristics of Health Education
Health education was either provided before or during the mass gathering, with a majority provided before the mass gathering event. This education was provided as a whole program or part of other education or general advice before the participants attended the mass gathering. These educational programs are targeted at improving the practice of better health etiquette during mass gatherings. The educational intervention was delivered or participants received the information in various methods such as in-person classes/workshops, videos/films, leaflets, magazines, television (TV) and radio programs, mobile applications, specialist travel clinics, specific hajj/ministry websites, other general websites, press and publications, social media, leaflets, medication labels, internet sources, and previous experiences. This education was provided by general practitioners, nurses, family and friends, any health care providers, selected physicians, pharmacists, health educators, and tour groups/hajj agents. The detailed information on health education is provided in Table 1.
3.4. Details and Focus of the Health Education
Although a good number of studies provided detailed information on the focus and contents of health education, some studies did not [28,29,30,41]. The focus of health education was asthma education [27], medication storage and handling [31], insulin storage [35], hand rubbing and mask use [32], prevention of influenza-like-illness [33], prevention of respiratory tract infection [36] medical seeking training [34], Middle East respiratory syndrome coronavirus-2 (MERS Cov-2) [39], cardio-pulmonary resuscitation (CPR) training [40], injury prevention [44] and general or various health education as part of the hajj/umrah pilgrimage [37,38,42,45] based on mass gatherings. Detailed information on various health education given to those who attend a mas gathering is provided in Table 2 and Supplementary File S3.
3.5. Effectiveness of Health Education
3.5.1. Knowledge, Attitude, and Practice
A total of six studies explored the impact of health education on the knowledge, attitude, or practice of good health etiquette among individuals participating in mass gatherings. A study by Tobaiqy et al. [30] observed significantly higher healthy practices, such as use of face mask (p = 0.04), avoiding sun exposure (p = 0.03), and healthy practice scores (p = 0.02) among those who received health education. Interestingly, Turkestani et al.’s study [42] noted that health education provided to pilgrims in their mother tongue through the pictorial chart as well as the distribution of pictorial pamphlets can significantly increase their knowledge on healthy practices (p < 0.05). This study reported a better knowledge score after the intervention. However, three studies [32,36,37] recorded no significant effect of health education on participants’ health-related knowledge, attitudes, or practices. The study by Alamry et al. [43] reported that there was a good average practice score (6.7 ± 2.1 out of 8) among the participants.
3.5.2. Vaccination
Three studies [28,29,41] reported that health recommendations and education could significantly improve the vaccine uptake. The study by Alqahtani et al. indicates that the advice from general practitioners (OR: 1.9) and the group leaders (OR: 2.1) almost doubled the vaccine intake compared to those who did not receive the education.
3.5.3. Compliance with the Use of Face Mask
A quasi-experimental study by Goni et al. [33] reported that a smartphone-based health education intervention significantly increased the compliance on overall face mask use (25% vs. 2%; p < 0.001), use of N95 mask (21.2% vs. 2%; p = 0.005); disposing the masks (44.2% vs. 16%; p = 0.004); mask use in masjid (44.2% vs. 22%; p = 0.05); and mask use in crowded areas (32.7% vs. 14%; 0.026). Similar findings were reported in two additional studies conducted in Egypt and Saudi Arabia, both of which demonstrated a positive impact of health education on significantly (p < 0.05) improving face mask compliance among pilgrims (29, 30). The study by Alamry et al. [43] reports that 99.9% of participants used a mask in crowded places.
3.5.4. Hand Hygiene
A study by Khamis et al. [29] reported that those who received a health education had better hand hygiene practice (58.7% vs. 11.8%) compared to those who did not. In contrast, a study by Salmuna et al. [32] reported no significant difference between pre- and post-hand-rub compliance (0.369) among hajj pilgrims in the intervention group.
3.5.5. Respiratory Infections
A quasi-experimental study by Goni et al. [33] reported that a smartphone-based health education intervention significantly reduced the occurrence of symptoms of respiratory tract infections (9.6% vs. 26.0%; p = 0.038).
3.5.6. Viral Infections
The study by Migault et al. [39] recorded that information about MERS-CoV provided by a nurse using an information leaflet increased the overall rate of correct responses (11 of 13) for MERS-CoV. However, the individual response to specific domains such as routes of transmission, symptoms, preventive behaviors to adopt, vaccines, and specific treatments remained lower than 50%.
3.5.7. Asthma Education
A study by Ramli et al. [27] reported the provision of general advice regarding asthma management as part of hajj-training. However, there was very little or no intake of this education as it was optional for the participants. There was also a lack of an individualized educational plan in this study.
3.5.8. Medication Storage
Receiving health education on medication storage was independently associated with good knowledge on appropriate storage of all medications (OR: 2.7; 95% CI: 1.4–5.0; p = 0.001) in hajj pilgrims [31]. Similar results were found among diabetic hajj pilgrims regarding insulin storage (0.52 ± 0.21 vs. 0.38 ± 0.19; p = 0.001) [35].
3.5.9. Cardio-Pulmonary Resuscitation (CPR)
The study by Beskind et al. [40] recorded that CPR training was not significantly effective in improving participant responsiveness. However, a significant improvement was found in chest compression depth and hands-off time following the video intervention.
3.5.10. Acceptance or Helpfulness of Health Education
Three studies indicated that the acceptance or helpfulness of health education among the participants was very high. The study by Tobaiqy et al. reported that 65% of the participants found the health education easier to follow and helpful, and 23% reported that the health education was beneficial to some extent [30]. Another study by Salmuna et al. recorded that there was a significant (p < 0.013) difference between pre-and post-hajj perception among hajj pilgrims in the intervention group [32]. Alamry et al. [43] reported that all of their participants benefited from the health education.
3.6. Practice Implications
Start health education early and in the native language: Health education should begin in pilgrims’ home countries, using their native language, and continue in the host country (e.g., Saudi Arabia during Hajj/Umrah) [27,29,30,31,34,35,42].Build a strong educator–participant relationship: Establishing trust and communication between health educators and pilgrims is key to effective education and care delivery during mass gatherings [31,46].Tailor education to pilgrims’ needs: Education should consider individual factors such as health literacy, age, medical conditions, and preferences (e.g., using visuals or simplified language) [28,30,31,38].Boost participation through incentives and requirements: Developing engaging methods and possibly making educational sessions mandatory could improve participation and information uptake [28,30,38].Focus on preventive measures: Educational materials should emphasize preventive health practices alongside general advice to maximize impact [33,36,45].Use technology to increase reach and engagement: Mobile apps and social media platforms can make health education more accessible and widely accepted [33,36].Develop standardized content in collaboration with authorities: A standard health education package should be created with the Ministry of Health to ensure consistency. It could be shared via official travel websites and transportation systems (e.g., flights, buses, ships) [42].
3.7. Research Implications
Identify system-level barriers: More research is needed to understand the system level challenges in implementing health education programs for mass gatherings [44]. Identifying the type of gathering is very important to understand these barriers [47].Conduct large, long-term comparative studies: There is a need for large-scale studies comparing the effectiveness of different education methods, especially in terms of long-term knowledge retention [44].Examine the impact of information sources and relationships: Studies should explore how various information channels and the provider–receiver dynamic influence health education outcomes [27,30].Define what effective health education looks like: More research should clarify what constitutes effective health education for pilgrims. This should cover content, format, access, delivery, provider, language, and follow-up strategies [30].Understand pilgrims’ perceptions and knowledge gaps: Investigating pilgrims’ views will help identify knowledge gaps, which can inform the design of more targeted and effective education programs [32,48]. There is a lack of research evidence on how pilgrims perceive risks and adopt information, and how best to interact with their willingness to be trained in preventive measures [13].
4. Discussion
4.1. General Background of Discussion
Mass gatherings are increasing globally due to factors such as religious pilgrimages, international sporting events, and festivals. This rise presents both opportunities for cultural exchange and challenges in managing public health, safety, and logistics [2,49]. Health education is an important factor that improves practice and decreases disease burden during these events. However, this has rarely been addressed in the literature. This scoping review aimed to explore the existing knowledge on the impact of health education among mass gathering attendees. It also identified gaps in the current literature and provided practical and research implications to guide future efforts by stakeholders and researchers.
4.2. Findings from the Evidence and Discussion
Available evidence on health education for mass gatherings is scarce or not provided in an adequate manner. The need for structured and culturally sensitive health education aligns with global frameworks, such as the WHO guidelines on mass gatherings. These should emphasize risk communication, health promotion, and community engagement as core pillars of preparedness and response strategies [1,50]. Moreover, this approach supports Sustainable Development Goal 3 that focuses on good health and well-being, by promoting health literacy and access to essential health information, thereby empowering individuals to make informed decisions and reduce preventable health risks during mass gatherings [51]. Tailored health education aligned with these goals not only addresses individual behavior change but also contributes to broader public health resilience in line with global health objectives.
Our current review summarized beneficial effects of health education on improving the knowledge, attitude, and practice of pilgrims. However, these were based on the type and contents of the education provided. Furthermore, the language in which such education is delivered and who provides this education matters greatly in the uptake among the pilgrims [28,38,41,42]. Some pilgrims were observed to possess good health attitudes and practices, although their education level was low [46]. This might be due to their experience or personal knowledge from a previous pilgrimage. Interestingly, all studies reported that health recommendations and education could significantly improve the vaccine uptake, especially when advised by general practitioners or group leaders [28,29,41]. This evidence indicates that health education for pilgrims is highly effective when tailored in content, language, and delivered by trusted sources. Even those with lower education levels can exhibit good health practices, likely due to prior experiences. Trusted figures like general practitioners and group leaders play a key role in boosting vaccine uptake.
The mode of delivery plays a very important role in participant education, especially when there is room for continuous education [52]. This can be possible through digital delivery or mobile/online-based education where the participants can have continuous access. Additionally, this also can ensure access for their healthcare providers when needed [53]. Current challenges, such as digital literacy, participant convenience, internet availability, and availability of health educators, should be considered for effective digital health delivery [54]. Additionally, converting these education materials into alternative forms like short videos, documentaries, and audio-visuals with original case scenarios will help participants recollect this information in a stronger way and has been found to be most effective [53,55]. Hence, regional health authorities should encourage these initiatives for better health practices among those attending a mass gathering.
Evidence from this review indicates that health education can significantly increase compliance with regular face mask use in various settings like the masjid or crowded areas. Additionally, it improves rates of safe disposal and handling of masks [29,30,33]. Although health education significantly improved hand hygiene practices [29], compliance with hand-rubbing was not improved [32]. This suggests a gap between knowledge acquisition and behavioral execution in specific practices [12,56,57]. A recent pilot clinical trial explored the relationship between practicing hand hygiene and rates of ARI in Umrah pilgrimage, and no significant relation could be established [58]. However, this study established the feasibility of conducting large clinical trials in this domain. Factors such as accessibility, cultural preferences, or misconceptions about hand-rub effectiveness may contribute to this discrepancy [37,59]. Therefore, targeted interventions addressing these specific barriers, alongside general education, may be necessary to ensure consistent adoption of all recommended hygiene practices during mass gatherings.
Health education can significantly decrease the occurrence of respiratory infections [33], and increase the overall knowledge on these infections [39]. However, domain-specific knowledge on routes of transmission, symptoms, preventive behaviors to adopt, vaccines, and specific treatments remained lower than 50% among participants [39]. While general health education has shown a positive impact on reducing respiratory infections and improving overall awareness, there is a limited understanding of specific aspects, such as transmission routes, symptom recognition, nonpharmaceutical interventions, personal protective behaviors and environmental hygiene, as well as targeted prevention strategies such as hygiene promotion, mask use, and social distancing [60,61]. This highlights a critical gap in educational outreach. Although one recent trial failed to establish a relationship between the best hand-hygienic practice and incidence of respiratory infection, it could open the possibilities to conducting large trials in this domain [58]. It is important to note that there was no or little uptake of asthma education among a set of hajj-pilgrimage attendees [27]. However, it was provided as optional education along with other general advice. This indicates that broad messages alone may not be sufficient; instead, more focused, topic-specific content is needed to deepen understanding [62]. The low uptake of asthma education among certain pilgrim groups further emphasizes the need for tailored interventions that address individual health conditions and prioritize high-risk populations. Strengthening the depth and reach of education programs could significantly enhance preparedness and health outcomes during mass gatherings [11,28,30,31,38].
Health education significantly improved the knowledge and practice of medication storage among all pilgrims and those with specific diseases like diabetes [31,35]. The improvement in medication storage practices among pilgrims reflects the potential of targeted health education to influence practical, disease-specific behaviours [35,63]. Proper medication management is particularly crucial in extreme environments like those encountered during mass gatherings, where temperature control and accessibility can be challenging. For individuals with chronic conditions such as diabetes, safe storage directly impacts treatment effectiveness and health outcomes [64,65,66]. This suggests that when health education addresses both general and condition-specific needs, it can empower pilgrims to take proactive steps in managing their health more effectively throughout their journey.
There is evidence that indicates musculoskeletal benefits through the application of personalized intervention, especially when more physical activities are involved in events or gatherings [44]. It is very important to provide specific tailored musculoskeletal health-based interventions for music or band students, for example, and those preparing for or performing in concerts, given the physical demands required [67,68,69]. Repetitive movements, prolonged practice sessions, and performance-related stress can lead to muscular strain and pain over time. The effectiveness of a short, structured injury prevention session highlights the value of integrating such strategies into music education programs, especially in universities [69,70]. By equipping students with practical tools to protect their physical health, institutions can help sustain their long-term performance ability and overall well-being.
No significant benefit was observed with CPR education or health education in reducing the outpatient and emergency room visits among the pilgrims [40,45]. However, a significant improvement was found in hands-off time during chest compressions following the video intervention. This might be due to participants’ inability to grasp this information and the need for more tailored information to be adapted in the future. Though none of the studies addressed the impact of education in preventing hand-cut injuries while slaughtering, it is very important to educate pilgrims on safe and preventive measures to take while performing the slaughtering [14,71].
4.3. Limitations and Gaps
Though this scoping review extensively addressed the current knowledge and understanding on the impact of health education in mass gatherings, there are gaps and limitations in the existing evidence. The lack of organized education programs and lesser intake of these programs [27,29,32,46], self-reported outcomes in studies due to cross-sectional study nature and associated recall bias [31,33,35,36,38,45,48,60], short duration, lesser sample size, and lack of follow-up [33,34,40,44,45] were limitations of this review. Additionally, high heterogeneity in health education and related outcomes might have hampered the complete generalizability of findings. Finally, the exclusion of non-English language studies, grey literatures, and qualitative studies might have contributed to us missing some important papers. Additionally, hajj and umrah are the largest mass gathering across the globe and there is a possibility that many papers have been published in regional languages. However, a comprehensive search strategy and use of multiple databases may have helped us to locate the maximum possible literature on this topic.
5. Conclusions
Overall, the evidence from this review underscores the vital role of targeted and well-delivered health education in improving health-related knowledge, attitudes, and practices among individuals participating in mass gatherings. Brief interventions which focus on targeted participants can yield meaningful benefits. From enhancing preventive behaviors to improving medication storage and reducing infections, health education proves to be a powerful tool in preparing for mass gathering events. However, the current lack of conclusive evidence highlights the need for further research to strengthen and expand this area of study. Trusted sources and culturally tailored content significantly influence effectiveness, and even brief interventions can yield meaningful benefits, as seen in injury prevention among music students. There was an absolute lack of evidence in assessing the effectiveness of health education on clinical outcomes such as morbidity, mortality, and quality of life. Future efforts should focus on refining educational strategies to ensure they are accessible, relevant, and responsive to the unique needs of diverse populations in high-risk, high-density settings.
Deviation from the Registered Protocol
Though the actual protocol for this study was registered to understand the effectiveness of health education in reducing morbidity and mortality during mass gathering events (PROSPERO ID: CRD42025637008), we could not find any studies on it. Hence, we modified our outcomes into “all health-related outcomes” instead of “morbidity and mortality”.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Public Health for Mass Gatherings: Key Considerations WHO Geneva, Switzerland 2015
- 2Halsey E. CDC Yellow Book 2026: Health Information for International Travel Oxford University Press Oxford, UK 2025
- 3Al-Tawfiq J.A. Gautret P. Benkouiten S. Memish Z.A. Mass Gatherings and the Spread of Respiratory Infections. Lessons from the Hajj Ann. Am. Thorac. Soc.20161375976510.1513/Annals ATS.201511-772FR 27088298 · doi ↗ · pubmed ↗
- 4David S. Roy N. Public health perspectives from the biggest human mass gathering on earth: Kumbh Mela, India Int. J. Infect. Dis.201647424510.1016/j.ijid.2016.01.01026827807 · doi ↗ · pubmed ↗
- 5Parker S. Steffen R. Rashid H. Cabada M.M. A Memish Z. Gautret P. Sokhna C. Sharma A. Shlim D.R. Leshem E. Sacred journeys and pilgrimages: Health risks associated with travels for religious purposes J. Travel Med.202431 taae 12210.1093/jtm/taae 12239216102 PMC 11646089 · doi ↗ · pubmed ↗
- 6Memish Z.A. Steffen R. White P. Dar O. Azhar E.I. Sharma A. Zumla A. Mass gatherings medicine: Public health issues arising from mass gathering religious and sporting events Lancet 20193932073208410.1016/S 0140-6736(19)30501-X 31106753 PMC 7159069 · doi ↗ · pubmed ↗
- 7Dehning J. Mohr S.B. Contreras S. Dönges P. Iftekhar E.N. Schulz O. Bechtle P. Priesemann V. Impact of the Euro 2020 championship on the spread of COVID-19Nat. Commun.20231412210.1038/s 41467-022-35512-x 36653337 PMC 9849464 · doi ↗ · pubmed ↗
- 8Johnson D.R. Health Communications Matter: A Comparative Case Study of Best Practices to Combat Misinformation and Disinformation During the COVID-19 Pandemic Ph.D. Thesis The University of North Carolina Chapel Hill, NC, USA 2024