Effect of Family and Personal Medical History on Treatment Outcomes of Tyrosine Kinase Inhibitors (TKIs) in Non-Small Cell Lung Cancer (NSCLC)
Heves Surmeli, Ezgi Turkoglu, Deniz Isik, Oguzcan Kinikoglu, Yunus Emre Altintas, Ugur Ozkerim, Sila Oksuz, Tugba Basoglu, Hatice Odabas, Nedim Turan

TL;DR
This study finds that family and personal medical history affects treatment complications and recurrence in NSCLC patients on tyrosine kinase inhibitors, but not survival or genetic mutations.
Contribution
The study identifies family and personal medical history as a novel predictive factor for treatment outcomes in NSCLC patients receiving TKIs.
Findings
Patients with family/personal medical history had higher chronic disease burden and poorer ECOG scores.
FPMH was associated with increased recurrence and chemotherapy-related toxicity.
No significant differences in survival or mutation status were observed between groups.
Abstract
Background: Tyrosine kinase inhibitors (TKIs) have significantly improved outcomes in non-small cell lung cancer (NSCLC), especially among patients with actionable genetic mutations. However, the influence of family and personal medical history (FPMH) on clinical and treatment outcomes with TKI therapy remains underexplored. Methods: We conducted a retrospective cohort study involving 136 NSCLC patients receiving TKIs, categorized into two groups based on the presence or absence of documented FPMH. Clinical variables assessed included demographic data, comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status, tumor characteristics, genetic mutations (EGFR, ALK, ROS1), treatment responses, toxicity profiles, and survival outcomes. Statistical analyses included Chi-square tests, t-tests, Mann–Whitney U tests, Spearman correlation, and univariate logistic regression (p <…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
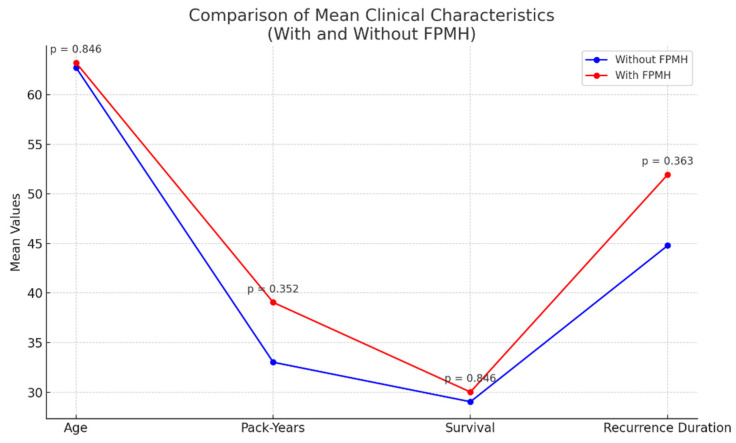 Figure 1
Figure 1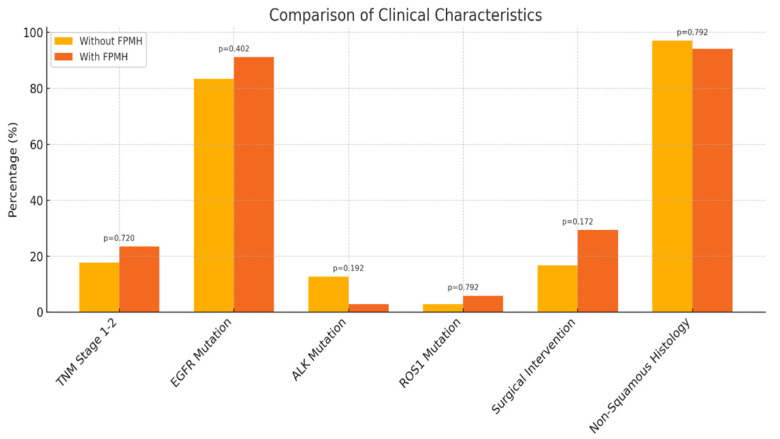 Figure 2
Figure 2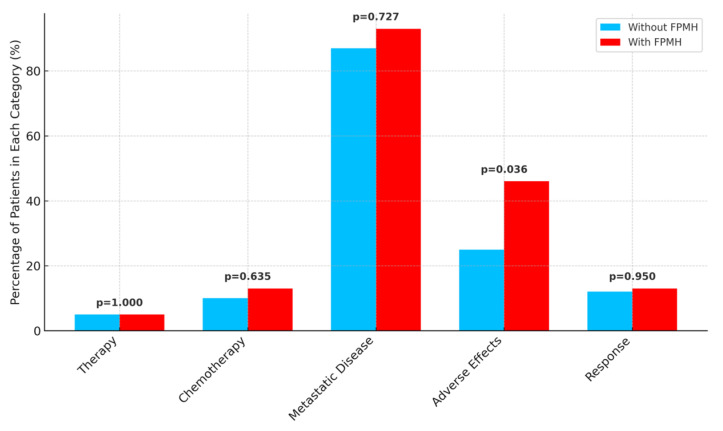 Figure 3
Figure 3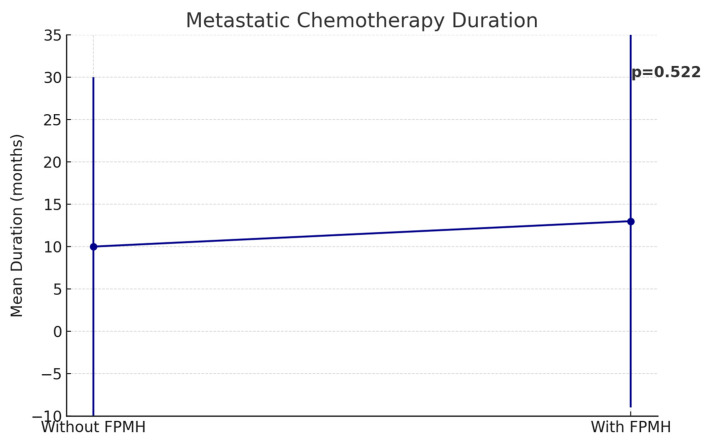 Figure 4
Figure 4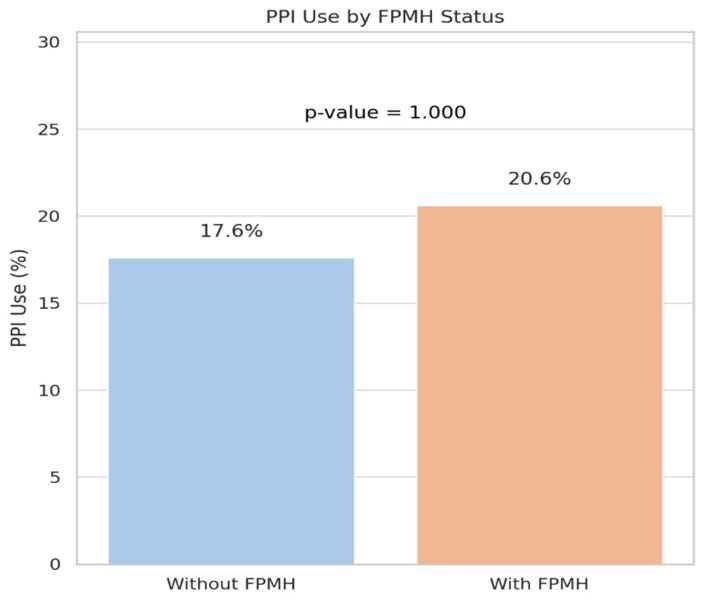 Figure 5
Figure 5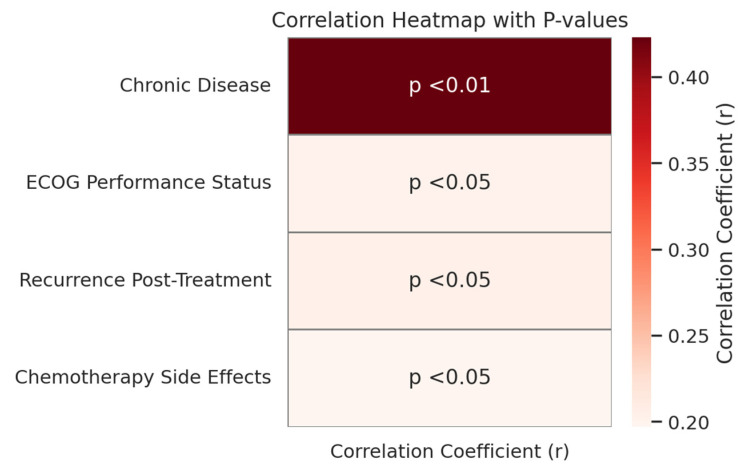 Figure 6
Figure 6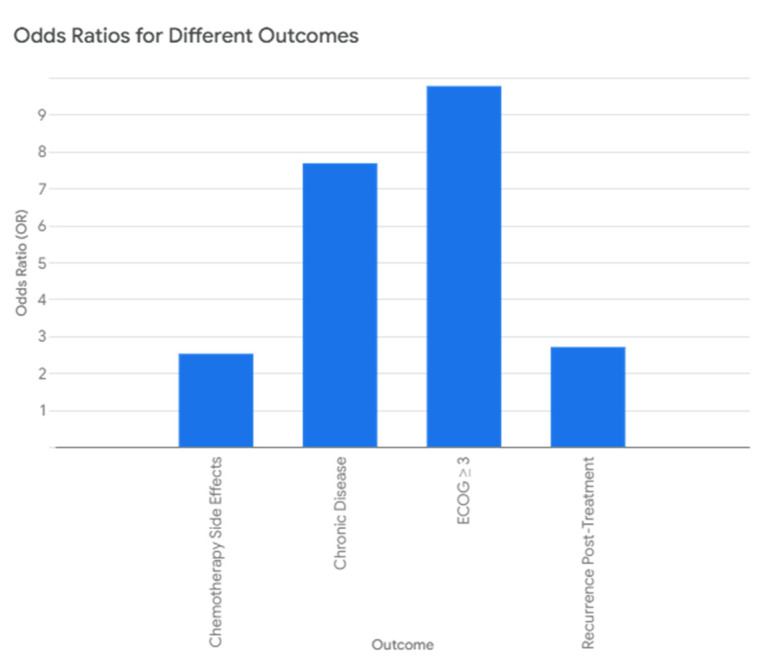 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Cancer Genomics and Diagnostics · Lung Cancer Research Studies
1. Introduction
Lung cancer remains the leading cause of cancer-related mortality globally, with non-small cell lung cancer (NSCLC) accounting for approximately 85% of all cases. NSCLC includes several histologic subtypes such as adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. Despite advances in screening and treatment, most NSCLC cases are diagnosed at an advanced stage, and the overall 5-year survival remains below 25% [1,2].
A variety of risk factors contribute to NSCLC pathogenesis, including smoking, environmental exposures (e.g., radon, asbestos), and genetic predisposition [3,4,5]. In recent years, targeted therapies such as tyrosine kinase inhibitors (TKIs) have become essential for NSCLC patients with actionable mutations, particularly in EGFR, ALK, and ROS1 genes [6,7,8]. These therapies have substantially improved outcomes, particularly in patients with adenocarcinoma and non-smoking status. However, there remains heterogeneity in treatment response, even among patients with similar genetic mutations.
One underexplored factor potentially influencing treatment outcomes is family and personal medical history (FPMH). FPMH refers to a documented history of malignancy or chronic disease in the patient or first-degree relatives. Previous studies have shown that family history of cancer may correlate with a higher prevalence of actionable mutations and may also reflect inherited cancer susceptibility [9,10]. Similarly, a patient’s own medical history, including prior malignancy or chronic comorbidities (e.g., diabetes, cardiovascular disease), may impact drug metabolism, immune response, and tolerance to therapy [11,12,13].
Despite its clinical relevance, few studies have evaluated the role of FPMH in NSCLC patients undergoing TKI therapy. One retrospective analysis by Obiols et al. (2022) suggested that a family history of cancer might influence survival outcomes with TKIs, but the sample size was limited, and conclusions were inconclusive [14]. Moreover, existing literature often overlooks the impact of comorbidities, functional status, and recurrence risk in this context.
Therefore, this study aims to systematically evaluate the effect of FPMH on clinical and treatment outcomes in NSCLC patients treated with TKIs. Specifically, it investigates differences in comorbidity burden, ECOG performance status, recurrence, toxicity, survival, and genetic biomarkers between patients with and without FPMH. Understanding whether FPMH influences TKI treatment response may support more individualized approaches in NSCLC management.
2. Materials and Methods
2.1. Study Design
This was a retrospective cohort study designed to assess the effect of family and personal medical history (FPMH) on clinical and treatment outcomes in patients with non-small cell lung cancer (NSCLC) treated with tyrosine kinase inhibitors (TKIs). Specifically, we aimed to (1) compare clinicopathological characteristics between patients with and without FPMH, (2) evaluate the prognostic relevance of clinical variables including FPMH using survival analysis, and (3) identify variables associated with the presence of FPMH.
2.2. Definition of FPMH
FPMH was operationally defined as the presence of either of the following:
Family history: A first-degree relative (parent, sibling, or child) diagnosed with cancer or a major chronic illness such as cardiovascular disease, diabetes, or hypertension.
Personal history: Documented diagnosis of chronic diseases (e.g., diabetes mellitus, chronic obstructive pulmonary disease, hypertension) or a prior cancer diagnosis in the patient themselves.
We acknowledge that some chronic diseases included in the FPMH definition may be potential risk factors for NSCLC or influence treatment outcomes (e.g., affecting ECOG performance or drug metabolism). To address this, additional statistical adjustments and subgroup analyses were performed.
2.3. Patient Population
We reviewed medical records of 162 NSCLC patients treated with TKIs at Kartal Dr. Lütfi Kirdar City Hospital from January 2020 to June 2023. After excluding 26 patients due to missing essential data, the final sample included 136 patients, stratified into two groups:
FPMH group: 34 patients.
Non-FPMH group: 102 patients.
Inclusion criteria:
Histologically confirmed NSCLC.
Received at least one line of TKI therapy.
Complete medical records including clinical history, treatment response, and follow-up.
2.4. Data Collection
We extracted the following variables:
Demographic: Age, sex, smoking status, and pack-years.
Clinical: ECOG performance status, comorbidities, FPMH status, and recurrence.
Pathological: Tumor histology, TNM stage (AJCC 8th edition), and PD-L1 expression.
Molecular: EGFR, ALK, and ROS1 mutation status.
Treatment: Type and duration of TKI, chemotherapy, toxicity, and surgical intervention.
Outcome: Overall survival (OS), progression-free survival (PFS), toxicity, and recurrence.
2.5. Statistical Analysis
Descriptive statistics were presented using means ± standard deviations for continuous variables and frequencies (%) for categorical variables.
Group comparisons used Chi-square/Fisher’s exact tests (categorical), t-tests (parametric continuous), or Mann–Whitney U tests (non-parametric).
Correlation analysis: Spearman’s rank correlation coefficient (non-parametric) was used to assess associations between FPMH and clinical variables.
Survival analysis:
Kaplan–Meier (K–M) curves for OS and PFS were plotted and compared using the log-rank test.
Cox proportional hazards regression was applied to estimate hazard ratios (HR) and 95% confidence intervals for key predictors (age, ECOG, stage, FPMH, mutation status).
Predictor analysis of FPMH:
A logistic regression model was built with FPMH as the dependent variable.
Independent predictors included comorbidity, ECOG score, recurrence, and molecular status.
A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS v25 (IBM Corp., Armonk, NY, USA).
3. Results
A total of 136 NSCLC patients treated with TKIs were analyzed, including 102 patients without a family and personal medical history (FPMH) and 34 patients with FPMH. The comparison between groups is summarized below.
3.1. Demographic and Clinical Characteristics
The gender distribution and smoking status were similar between groups. Female representation was 54.9% (56/102) in the non-FPMH group and 47.1% (16/34) in the FPMH group (p = 0.552). Non-smokers made up 62.7% (64/102) of the non-FPMH group and 55.9% (19/34) of the FPMH group (p = 0.612).
However, patients with FPMH had a significantly higher prevalence of chronic diseases (58.8% vs. 15.7%, p < 0.001) and poorer performance status as measured by the Eastern Cooperative Oncology Group (ECOG) score (≥3 in 8.8% vs. 1.0%, p = 0.048). ECOG scores reflect patients’ functional status and range from 0 (fully active) to 5 (deceased).
As shown in Table 1, patients with a family or personal medical history (FPMH) of disease had a significantly higher prevalence of chronic disease (58.8% vs. 15.7%, p < 0.001) and recurrence post-treatment (41.2% vs. 20.6%, p = 0.031) compared to those without FPMH. Also, as shown in Figure 1, patients with a family or personal medical history (FPMH) of disease exhibited higher mean values for their pack-years, recurrence duration, and chronic disease prevalence, although the differences in their age and survival were not statistically significant.
3.2. Tumor Characteristics, Staging, and Genetic Markers
TNM staging and molecular profiles were largely similar across both groups. TNM classification, which assesses tumor size, lymph node involvement, and metastasis, showed no statistical difference (early-stage [I–II]: 17.6% non-FPMH vs. 23.5% FPMH; p = 0.720) [14].
Genetic mutations, including EGFR, ALK, and ROS1, also did not differ significantly. EGFR mutations were present in 83.3% of non-FPMH patients and 91.2% of FPMH patients (p = 0.402). Similarly, surgical rates and histological subtypes showed no significant difference. Figure 2 highlights that tumor stage and genetic biomarkers such as EGFR, ALK, and ROS1 mutations were not significantly different between groups [14,15,16].
As presented in Table 2, no statistically significant differences were observed between the FPMH and non-FPMH groups in tumor stage, EGFR mutation status, or other genetic biomarkers.
3.3. Treatment Characteristics and Toxicity
Chemotherapy-related toxicity was significantly more common among patients with FPMH (50.0% vs. 28.4%, p = 0.036), while rates of neoadjuvant therapy, adjuvant chemotherapy, and metastatic status were similar (p > 0.05 for all). The duration of metastatic chemotherapy and response rates were also statistically equivalent [17].
As shown in Figure 3, chemotherapy-related adverse effects were significantly more frequent in the FPMH group (p = 0.036), although other treatment parameters were comparable. While Figure 4 presents the duration of metastatic chemotherapy, indicating no significant difference between groups (p = 0.522).
According to Table 3, a significantly higher proportion of patients with FPMH experienced chemotherapy-related adverse effects compared to those without FPMH (50.0% vs. 28.4%, p = 0.036). However, other treatment variables and metastatic status showed no significant differences between the groups.
3.4. Laboratory Findings and Medication Use
Laboratory parameters, including liver function tests, hematologic indices, and carcinoembryonic antigen (CEA), were comparable between groups. Use of proton pump inhibitors (PPIs) was also similar (17.6% vs. 20.6%, p = 1.000) [18].
As shown in Table 4, there were no statistically significant differences in laboratory parameters or proton pump inhibitor (PPI) use between patients with and without a family or personal medical history (FPMH).
Figure 5 shows that PPI usage was similar across both groups (p = 1.000), consistent with the non-significant findings regarding laboratory parameters.
Correlation and Regression Analyses
Spearman correlation showed moderate to strong associations between FPMH and several variables: chronic disease (r = 0.423, p < 0.01), ECOG status (r = 0.201, p < 0.05), recurrence (r = 0.204, p < 0.05), and chemotherapy toxicity (r = 0.197, p < 0.05).
Univariate logistic regression revealed that FPMH increased the odds of the following:
Having a chronic disease (OR = 7.68, p < 0.001).
Recurrence (OR = 2.70, p = 0.020).
Chemotherapy-related toxicity (OR = 2.52, p = 0.023).
ECOG ≥ 3 had an odds ratio of 9.77 (p = 0.052), indicating a borderline association.
Importantly, no significant associations were observed between FPMH and survival duration or genetic mutation status, despite significant differences in recurrence and toxicity, suggesting that FPMH may influence treatment tolerance and post-treatment outcomes more than inherent tumor biology.
As visualized in Figure 6, moderate to strong correlations were observed between FPMH, chronic disease, ECOG performance, recurrence, and chemotherapy toxicity.
As detailed in Table 5, FPMH status showed a moderate positive correlation with the presence of chronic disease (r = 0.423, p < 0.01), and weak but significant correlations with ECOG performance status, recurrence post-treatment, and chemotherapy side effects (p < 0.05 for each).
3.5. Survival Analysis
Kaplan–Meier survival analysis showed no significant difference in overall survival (OS) between the FPMH and non-FPMH groups (log-rank p = 0.73), confirming initial observations. Median OS was 28.7 months for FPMH patients vs. 29.1 months for non-FPMH.
Similarly, progression-free survival (PFS) did not differ significantly (log-rank p = 0.61), with median PFS at 10.2 months (FPMH) vs. 11.5 months (non-FPMH).
3.6. Cox Regression Analysis
Univariate Cox regression identified the following:
ECOG ≥ 2 was associated with significantly shorter OS (HR = 2.38; 95% CI: 1.22–4.63; p = 0.011).
Advanced stage (III–IV) also predicted worse OS (HR = 1.79; 95% CI: 1.02–3.11; p = 0.042).
FPMH was not a statistically significant predictor of OS (HR = 1.08; 95% CI: 0.65–1.80; p = 0.761).
3.7. Predictors of FPMH (Logistic Regression)
To identify predictors associated with the presence of FPMH, we performed multivariate logistic regression:
Chronic disease strongly predicted FPMH (OR = 5.91; 95% CI: 2.38–14.65; p < 0.001).
ECOG ≥ 2 was marginally associated with FPMH (OR = 2.13; p = 0.068).
Mutation status (EGFR/ALK/ROS1), recurrence, or sex did not independently predict FPMH. Figure 7 further illustrates that FPMH significantly increased the odds of chronic disease, post-treatment recurrence, and chemotherapy-related side effects.
As shown in Table 6, logistic regression analysis revealed that patients with FPMH were significantly more likely to have chronic disease (OR = 7.68, p < 0.001), recurrence after treatment (OR = 2.70, p = 0.020), and chemotherapy side effects (OR = 2.52, p = 0.023). The association with poor ECOG performance (≥3) approached significance (p = 0.052).
4. Discussion
This study explored the impact of family and personal medical history (FPMH) on clinical and treatment outcomes among NSCLC patients treated with tyrosine kinase inhibitors (TKIs). Several key associations were identified, including a significantly higher prevalence of chronic diseases, poorer ECOG performance status, greater recurrence rates, and increased chemotherapy toxicity in patients with FPMH. However, no significant differences were observed in survival outcomes or in the prevalence of oncogenic mutations (e.g., EGFR, ALK, ROS1) [19].
The elevated chronic disease burden in FPMH patients likely reflects shared genetic or environmental risk factors, and may contribute to functional impairment, as evidenced by higher ECOG scores. Worse performance status in turn could affect treatment tolerance and increase the likelihood of recurrence and toxicity. Yet, the lack of differences in overall survival suggests that while FPMH may influence quality of life and treatment complications, it does not appear to affect the fundamental trajectory of the disease under TKI therapy [20,21].
Interestingly, the similarity in survival and mutation status between groups implies that the underlying tumor biology—including molecular drivers like EGFR or ALK—is not significantly impacted by FPMH in this cohort. One possible explanation is that TKI therapy, which targets specific mutations, remains effective regardless of comorbidity status or inherited cancer predisposition. Alternatively, it is possible that the small sample size of the FPMH group limited statistical power to detect subtle differences.
Previous studies have shown mixed results regarding the influence of family history on treatment outcomes in lung cancer. Some suggest that inherited predispositions may increase mutation prevalence or influence prognosis, while others find no survival impact. Our findings align with the latter, indicating that while FPMH may shape the patient’s overall health profile, it may not significantly alter the tumor’s genetic behavior or TKI responsiveness [22,23].
One possible biological link between FPMH and treatment outcomes could be pharmacogenomic variability—for example, inherited differences in drug metabolism enzymes, immune response genes, or DNA repair pathways. These factors might influence chemotherapy tolerance or recurrence risk, but further mechanistic studies are needed to confirm such hypotheses.
This study also has important limitations. Its retrospective design limits causal inference, and FPMH data were extracted from medical records, which may be incomplete or inconsistently documented. Furthermore, the group sizes were imbalanced (34 with FPMH vs. 102 without), which could introduce bias or reduce statistical power. Larger prospective studies with more granular genetic and clinical data are needed to validate these findings and explore underlying mechanisms [24].
5. Conclusions
5.1. Summary
This study demonstrates that family and personal medical history (FPMH) is associated with key clinical outcomes in NSCLC patients treated with tyrosine kinase inhibitors (TKIs). Specifically, FPMH was linked to a higher prevalence of chronic diseases, poorer ECOG performance status, increased post-treatment recurrence, and greater chemotherapy toxicity. However, no significant differences were observed in overall survival or tumor mutation profiles, suggesting that FPMH may influence the treatment experience rather than the biological behavior of the tumor.
These findings highlight the potential value of considering FPMH in risk stratification and clinical decision-making. Patients with FPMH may benefit from closer monitoring, supportive care measures, and proactive toxicity management.
5.2. Recommendations
Given the retrospective nature of this study and the small sample size in the FPMH subgroup, these associations should be interpreted with caution. Prospective studies with larger, balanced cohorts and integrated genomic data are needed to validate these observations and explore the biological mechanisms underlying FPMH-associated differences.
Incorporating FPMH into clinical assessment models may enhance personalized care in NSCLC, especially in predicting treatment-related complications. Further research should focus on defining specific FPMH elements (e.g., type of chronic disease, familial cancer patterns) that most strongly predict treatment outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Cancer Society Cancer Facts & Figures 20232023 Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2023/2023-cancer-facts-and-figures.pdf(accessed on 25 June 2025)
- 2Centers for Disease Control and Prevention Smoking and Cancer 2022 Available online: https://www.cdc.gov/tobacco/campaign/tips/diseases/cancer.html(accessed on 25 June 2025)
- 3Chen Y.T. EGFR mutations in non-small cell lung cancer: A focus on demographic disparities J. Thorac. Oncol.201712(Suppl. S 1)S 45S 4610.1016/j.jtho.2017.09.1504 · doi ↗
- 4Gainor J.F. Shaw A.T. Emerging paradigms in the development of resistance to tyrosine kinase inhibitors in lung cancer J. Clin. Oncol.2013313987399610.1200/JCO.2012.45.202924101047 PMC 3805932 · doi ↗ · pubmed ↗
- 5Goldstraw P. Chansky K. Crowley J. Rami-Porta R. Asamura H. Eberhardt W.E. Nicholson A.G. Groome P. Mitchell A. Bolejack V. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer J. Thorac. Oncol.201611395110.1016/j.jtho.2015.09.00926762738 · doi ↗ · pubmed ↗
- 6Grigolon R.B. Lasio L. Precision medicine in NSCLC: Challenges and opportunities Lung Cancer International Wiley Hoboken, NJ, USA 2023123456
- 7Hecht S.S. Tobacco carcinogens, their biomarkers and tobacco-induced cancer Nat. Rev. Cancer 2003373374410.1038/nrc 119014570033 · doi ↗ · pubmed ↗
- 8Hellmann M.D. Paz-Ares L. Bernabe Caro R. Zurawski B. Kim S.-W. Carcereny Costa E. Park K. Alexandru A. Lupinacci L. de la Mora Jimenez E. Nivolumab plus ipilimumab in advanced non–small-cell lung cancer N. Engl. J. Med.20193812020203110.1056/NEJ Moa 191023131562796 · doi ↗ · pubmed ↗