A Novel Serum-Based Bioassay for Quantification of Cancer-Associated Transformation Activity: A Case–Control and Animal Study
Aye Aye Khine, Hsuan-Shun Huang, Pao-Chu Chen, Chun-Shuo Hsu, Ying-Hsi Chen, Sung-Chao Chu, Tang-Yuan Chu

TL;DR
A new blood test detects ovarian cancer by measuring how cancer-related factors in the blood cause cells to grow abnormally.
Contribution
A novel serum-based bioassay using TY cells to detect cancer-associated transformation activity is introduced.
Findings
TY cells effectively distinguished cancer sera from controls with high statistical significance.
The AIG-promoting activity in sera correlated strongly with tumor burden in a mouse model.
HGF/c-MET and IGF/IGF-1R signaling pathways mediate the observed AIG-promoting activity.
Abstract
Background/Objectives: The detection of ovarian cancer remains challenging due to the lack of reliable serum biomarkers that reflect malignant transformation rather than mere tumor presence. We developed a novel biotest using an immortalized human fallopian tube epithelial cell line (TY), which exhibits anchorage-independent growth (AIG) in response to cancer-associated serum factors. Methods: Sera from ovarian and breast cancer patients, non-cancer controls, and ID8 ovarian cancer-bearing mice were tested for AIG-promoting activity in TY cells. Results: TY cells (passage 96) effectively distinguished cancer sera from controls (68.50 ± 2.12 vs. 17.50 ± 3.54 colonies, p < 0.01) and correlated with serum CA125 levels (r = 0.73, p = 0.03) in ovarian cancer patients. Receiver operating characteristic (ROC) analysis showed high diagnostic accuracy (AUC = 0.85, cutoff: 23.75 colonies). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
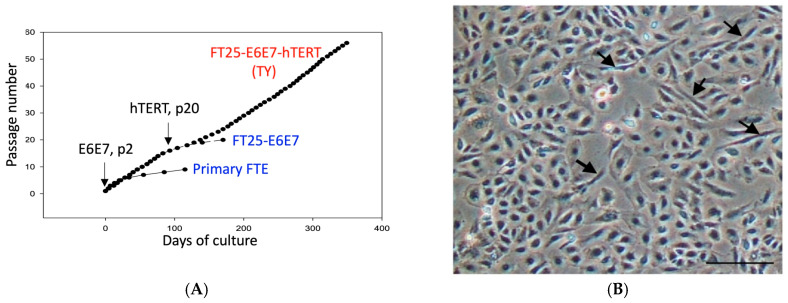 Figure 1
Figure 1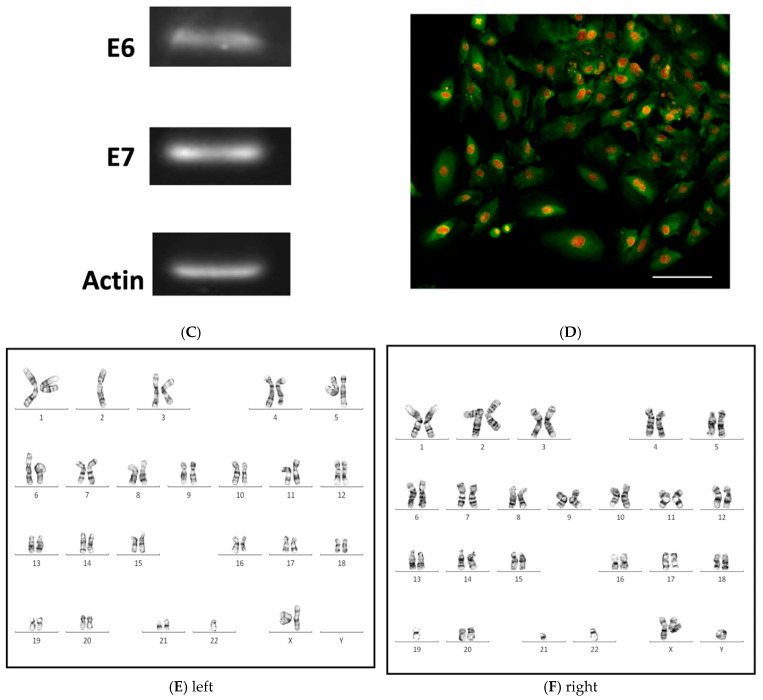 Figure 2
Figure 2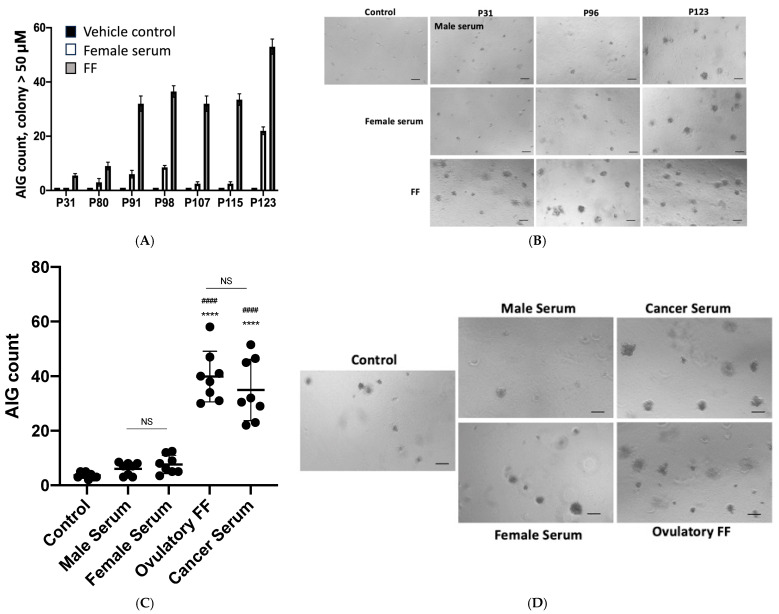 Figure 3
Figure 3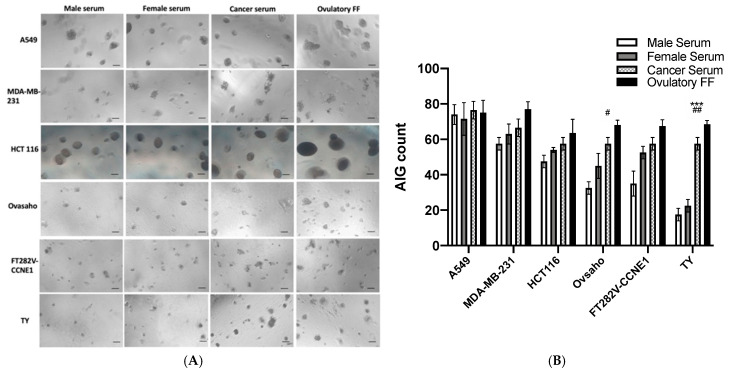 Figure 4
Figure 4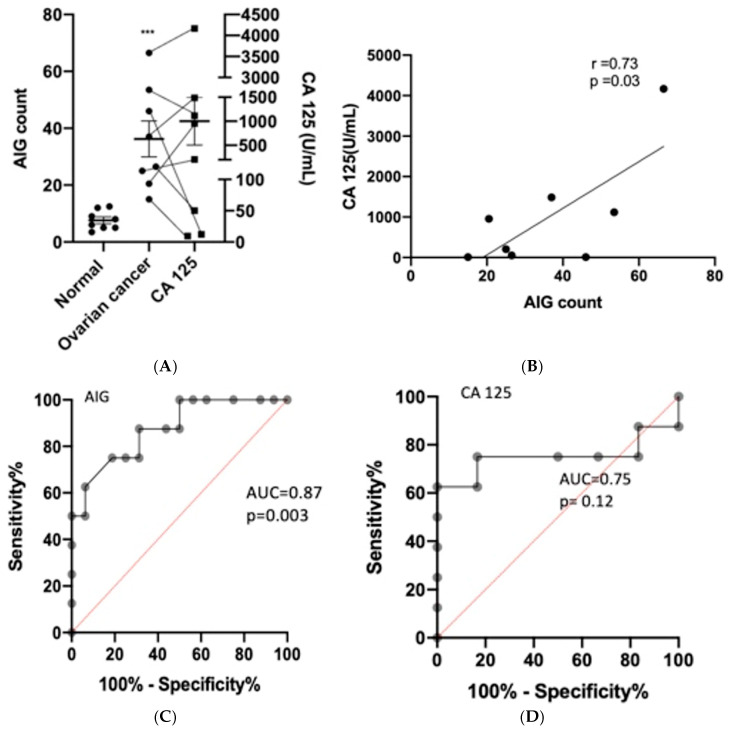 Figure 5
Figure 5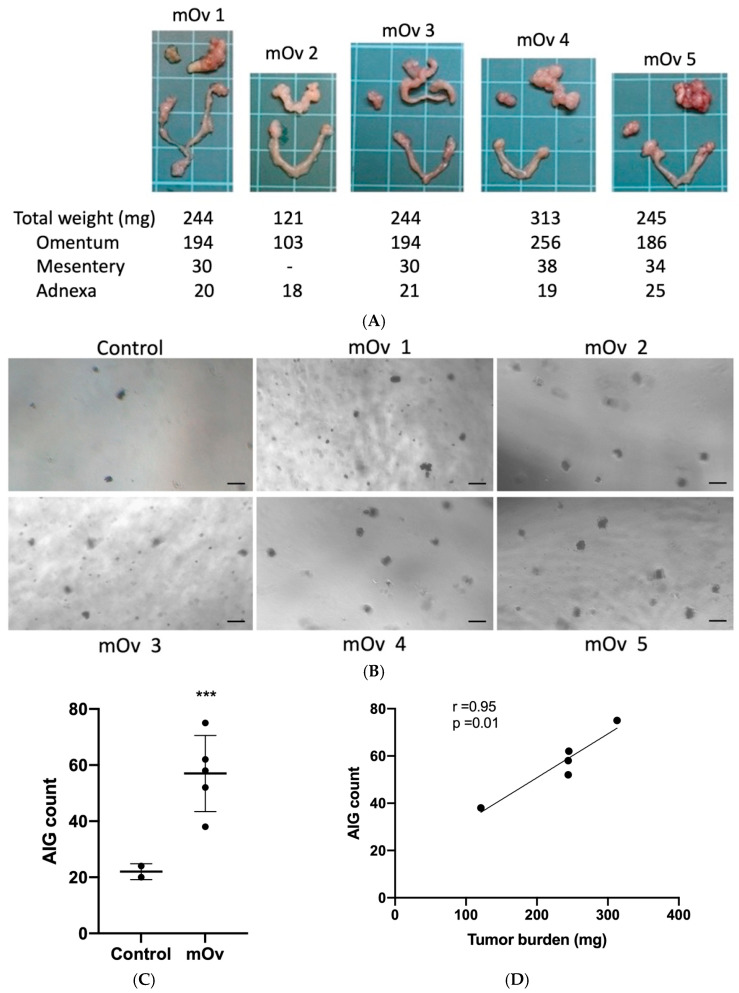 Figure 6
Figure 6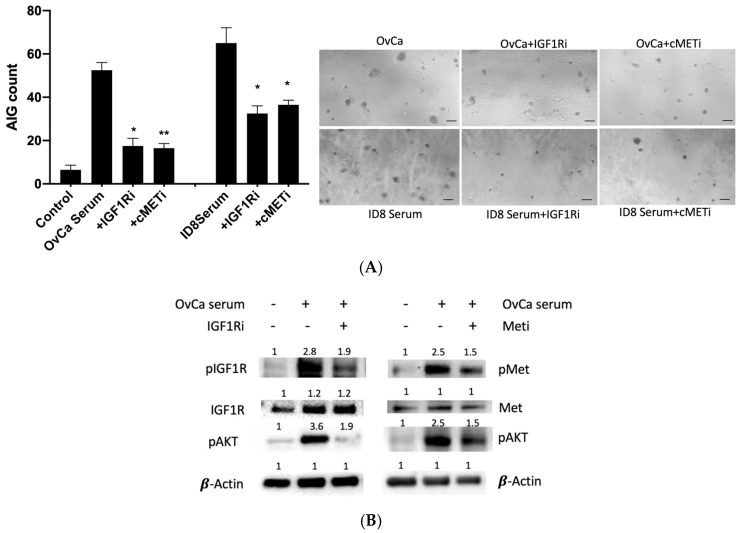 Figure 7
Figure 7- —Buddhist Hualien Tzu Chi General Hospital
- —Buddhist Tzu Chi Medical Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · Cancer Cells and Metastasis · Lung Cancer Treatments and Mutations
1. Introduction
Despite advances in cancer screening, approximately 50% of malignancies are still detected at advanced stages. While established screening programs have reduced mortality for cervical, breast, and colorectal cancers [1,2], most cancers—particularly those that are deeply located and rapidly disseminating—remain challenging to diagnose early. Ovarian cancer exemplifies this problem, as it is often asymptomatic until late stages and lacks reliable detection methods [3].
Blood-based testing represents the most non-invasive and widely acceptable approach for cancer diagnosis. However, only a few malignancies—such as multiple myeloma [4], gestational trophoblastic diseases [5], and germ cell tumors [6]—have tumor markers with sufficient diagnostic utility. For ovarian cancer, current biomarkers like carbohydrate antigen 125 (CA125) and human epididymis protein 4 (HE4) suffer from low specificity and sensitivity, leading to high false-positive rates [7]. Notably, large-scale screening trials using these markers failed to reduce ovarian cancer mortality [8,9], and HE4 provided no additional diagnostic benefit over CA125 [10,11].
A fundamental limitation of existing tests is their reliance on surrogate markers rather than assessing the biological hallmarks of cancer. An ideal diagnostic assay should directly measure malignant potential, such as the capacity for anchorage-independent growth (AIG), a defining feature of transformed cells. Unlike normal cells, which undergo anoikis when detached, cancer cells acquire the ability to survive and proliferate without attaching to a solid surface. A biotest that can measure the AIG-promoting activity in serum may offer a functional readout of malignancy and an idea blood test for cancer diagnosis.
We previously established an immortalized human cell line, TY, from the fallopian tube fimbria epithelium, named for its developer, Professor Tang-Yuan Chu. TY cells form AIG colonies in soft agar in response to various transforming signals, including ovulatory follicular fluid [12]. Key mediators of this process—such as insulin-like growth factor 2 (IGF-2), hepatocyte growth factor (HGF), and epidermal growth factor receptor ligands—drive malignant transformation [13,14,15,16]. Intriguingly, TY cells also responded to sera from cancer patients, suggesting their potential utility for tumor-derived factors.
In this retrospective study, we aimed to validate the diagnostic performance of the TY-based AIG assay for ovarian cancer detection, optimize testing conditions to maximize sensitivity and specificity, and determine whether AIG activity correlates with tumor burden in preclinical models. By focusing on the functional hallmark of malignancy—rather than indirect markers—this biotest holds promise for improving early cancer detection.
2. Materials and Methods
2.1. Serum Samples
Sera ovarian cancer patients (n = 8) and normal controls (8 female and 8 male) were provided by the Tzuchi Joint Tissue Bank of Gynecological Oncology (supported by Buddhist Tzuchi Medical Foundation, TCMMP104, and Hualien Tzuchi General hospital, TCRD113-075). Sera of breast cancer patients (n = 8) were provided by the National Biobank Consortium of Taiwan (NBCT, No. 230115). Follicular fluids were collected from women undertaking oocyte retrieval for in vitro fertilization program in Hualien Tzuchi Hospital. The Research Ethics Committee of Hualien Tzuchi Hospital (IRB101-09, IRB112-241-B) approved the study. Informed consent was received from all individuals and patients.
Serum samples were prepared before scheduled surgery or during OPD visit. FFs devoid of blood or flush medium contamination were collected at the time of sono-guided transvaginal oocyte retrieval as described earlier [12]. Sera from 8–10 week old 5 female C57BL/6 mice were collected soon after post-euthanasia. All the serum and FF samples were aliquoted into 1.5 mL Eppendorf and stored at −80 °C, and were used for this study from 2022 January to 2024 June.
2.2. Cell Culture
Immortalized fallopian tube epithelium cells FT282-CCNE1 (a kind gift from Dr. Ronny Drapkin) [17], were maintained in MCDB105 and M199 media (Sigma, St. Louis, MO, USA) supplemented with 10% fetal bovine serum (FBS) and 100 IU/mL of penicillin, and 100 μg/mL of streptomycin. The human high-grade serous carcinoma cell line OVSAHO was cultured in RPMI-1640 medium with 10% FBS, 100 IU/mL of penicillin, and 100 μg/mL of streptomycin. MDA-MB-231 human breast adenocarcinoma cells were cultured in Dulbecco’s modified Eagle’s medium (DMEM, Sigma, USA) supplemented with 10% FBS, 100 IU/mL of penicillin, and 100 µg/mL of streptomycin. HCT116 human colon adenocarcinoma cells and A594 human non-small cell lung carcinoma cells were cultured in RPMI-1640 (Sigma, USA) medium with L-glutamine and sodium bicarbonate, supplemented with 10% FBS, 100 IU/mL of penicillin, and 100 µg/mL of streptomycin.
2.3. Development of TY Cells
To establish an immortalized human fallopian tube epithelial cell line, the fimbria tissue at distal fallopian tube was treated with 1% trypsin and 5 mM EDTA for 30 min to separate the epithelium. The peeled epithelium was then digested with collagenase (c2674, Sigma, USA) at 1.5 mg/mL for 1 h, and cultured in DMEM, 10% FBS, with 5 μg/mL insulin on a 0.1% gelatin-coated plate. At passage two, the primarily cultured fimbria epithelial cells were transduced with an HPV16 E6/E7 lentivirus and subsequently with a lentiviral hTERT (Applied Biological Materials Inc., Richmond, BC, Canada) at passage 20 to generate the TY cell line. The cells were maintained in the same way as the FT282-CCNE1 fallopian tube epithelium cells.
2.4. Anchorage Independent Growth (AIG) Assay
The AIG assay was performed using a two-layer soft agar system. For the base layer, 0.8% agarose was prepared by dissolving agarose powder in distilled water at 100 °C for 10 min, then mixed with an equal volume of serum-free medium to achieve a final 0.4% concentration. The upper layer containing cells was prepared by suspending 500 TY cells in 0.4% agarose (maintained at 37 °C) with serum-free medium. In each well of a 96-well plate, 50 µL of the 0.8% base agar was allowed to solidify before adding 50 µL of the cell-containing 0.4% upper agar mixed with test sera or ovulatory follicular fluid (FF) at a final concentration of 10%. Fresh serum/FF was replenished at 48 h, and serum-free medium was added every 72 h to maintain moisture. After 10 days of culture at 37 °C with 5% CO_2_, colonies >50 µm in diameter were quantified manually under phase-contrast microscopy. For inhibitor studies, TY cells were pretreated with 100 nM picropodophyllin (PPP) or 10 µM AMG-337 for 30 min prior to agar embedding.
2.5. Western Blot
Western blot analysis was performed by quantifying protein concentrations using Bradford reagent (Bio-Rad, #500-0006, Hercules, CA, USA), denaturing 30 μg of protein per sample in 4× Laemmli buffer at 95 °C for 5 min, followed by separation via SDS-PAGE and transfer to nitrocellulose membranes. Membranes were probed overnight at 4 °C with primary antibodies against c-MET (BS-0668R, Bioss, Wuhan, China), phospho-c-MET (#3077S), IGF-1Rβ (#3027S), phospho-IGF-1Rβ (#3918S) (all 1:1000 from Cell Signaling, Danvers, MA, USA), and β-actin (#4967S, 1:5000, Cell Signaling, USA) as loading control, followed by TBST washes and incubation with HRP-conjugated secondary antibodies. Protein bands were visualized using ECL detection reagent (GE Healthcare, RPN2209, Buckinghamshire, UK) and imaged.
2.6. ID8 Syngeneic Mouse Ovarian Cancer Model
The mouse ovarian cancer cell line ID8 (SCC145, Sigma-Aldrich, St. Louis, MO, USA) was maintained in high-glucose Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 4% fetal bovine serum (FBS), 5 μg/mL insulin, 5 μg/mL transferrin, 5 ng/mL sodium selenite, 100 IU/mL penicillin, and 100 μg/mL streptomycin at 37 °C in a 5% CO_2_ atmosphere.
For tumor induction, 1 × 10^5^ ID8 cells suspended in 20 μL of serum-free medium were injected intraperitoneally into 8–10 week old female C57BL/6 mice. Four months post-injection, animals were euthanized. At necropsy, the peritoneal cavity was systematically examined and all visible tumor nodules were carefully dissected. Total tumor burden was quantified by measuring the combined weight of all excised tumors. Cardiac puncture was performed immediately post-euthanasia to collect blood samples, which were centrifuged at 4000× g for 30 min at 4 °C to obtain serum. Serum aliquots were stored at −80 °C until analysis. All animal procedures were approved by the Institutional Animal Care and Use Committee of Tzu Chi University (Protocol 112-30).
2.7. Statistical Analysis
GraphPad Prism (ver.8.0c) (GraphPad Software, San Diego, CA, USA) was applied to perform unpaired Student’s t-tests which were used to analysis the AIG count, and linear correlations were done by the Pearson correlation coefficient. p values less than 0.05 were defined as significant.
3. Results
3.1. Characteristics of TY Cells
After immortalization with E6/E7 and hTERT, the established TY cells at passage 90 exhibit a predominantly cobblestone epithelial morphology, with a minor fibroblast-like subpopulation (Figure 1A,B). All cells expressed the epithelial marker EpCAM (Figure 1C). Immunoblot analysis confirmed stable expression of E6 and E7 oncoproteins (Figure 1D). Karyotype analysis at passage 28 revealed two different polyploidic karyotypes. One karyotype was 44, XX, -2,-22 and the other was 44, XX, 5p-, -19, -21, -22, +ring chromosome (Figure 1E).
3.2. Optimization of Transformation Detection Capacity
Through systematic evaluation of multiple passages, we identified passage 96 TY cells as exhibiting optimal responsiveness to transformation signals. This determination was based on their enhanced ability to discriminate between the known transforming FF (from 8 follicles) and control serum (from 8 female and 8 male donors, Table 1). FF, which we previously demonstrated possesses strong transformation potential (16), induced robust AIG in TY cells. Comparing TY cells at different passages, the difference between FF and normal serum was significantly higher for passage 91 to passage 115 than that observed in earlier and later passages (Figure 2A,B). Importantly, these cells showed comparable responsiveness to sera from 8 stage I breast cancer patients (Table S1) (39.89 ± 9.2 colonies) versus FFs (34.93 ± 11.22 colonies), while maintaining minimal background activity with normal donor sera (male: 5.81 ± 4.33; female: 4.0 ± 2.5 colonies) (Figure 2C,D). The results indicated TY cells at passage 96 exhibit the highest ability to detect malignant signals from cancer sera.
3.3. Comparative Evaluation of Transformation Detection Across Cell Lines
We conducted comprehensive comparisons of transformation detection capacity across various established cancer cell lines (A549 lung cancer, MDA-MB-231 triple-negative breast cancer, HCT116 colon cancer) and ovarian cancer-relevant lines (OVSAHO high-grade serous ovarian cancer, FT282-CCNE1, and TY fallopian tube epithelial cells) (Figure 3). FT282-CCNE1 cells—which carry both TP53 and CCNE1 alterations—as well as all tested cancer cell lines, displayed constitutive AIG activity irrespective of serum source. Notably, TY cells showed the most pronounced differential response between normal (n = 16) and stage 1 breast cancer (n = 8) sera (Figure 3). Quantitative analysis revealed that TY cells formed 17.50 ± 3.54 colonies with normal male serum, 22.50 ± 3.54 with normal female serum, and 57.50 ± 3.55 with breast cancer serum—approaching the positive control response to FF (68.50 ± 2.12 colonies). This superior discriminative capacity highlighted TY cells’ unique suitability for serum-based cancer detection.
3.4. Diagnostic Performance in Clinical Ovarian Cancer Detection
In clinical validation studies using serum samples from ovarian cancer patients and non-cancer controls (demographics in Table 1 and Table 2), TY cells exhibited significantly higher AIG colony formation with cancer sera (37.06 ± 18.03, range: 15.00–66.50 colonies) compared to control sera (4 ± 2.5 colonies, range: 1.00–8.50 colonies) (Figure 4A). This transformation activity showed strong positive correlation with serum CA125 levels (r = 0.73, p = 0.03; Figure 4B), suggesting that the AIG assay captures clinically relevant malignant features. Receiver operating characteristic (ROC) analysis demonstrated superior diagnostic performance of the TY-AIG assay (AUC = 0.87, p = 0.003) compared to CA125 alone (AUC = 0.75, p = 0.12) (Figure 4C,D), indicating its potential as a more accurate diagnostic tool.
3.5. Correlation with Disease Burden in Preclinical Models
To evaluate the assay’s ability to reflect disease progression, we employed an ID8 syngeneic mouse model of ovarian cancer peritoneal dissemination [18]. Four months post-injection, all mice developed characteristic peritoneal metastases, predominantly in the omentum with smaller deposits in the mesentery and adnexa (Figure 5A). Serum from tumor-bearing mice induced significantly higher TY cell AIG (57.0 ± 13.56 colonies) compared to normal mouse serum (22.0 ± 2.83 colonies; Figure 5B,C). Most importantly, AIG counts showed remarkable correlation with total tumor weight (r = 0.95, p < 0.01) and metastatic burden at specific sites (Figure 5D and Figure S1), suggesting the assay’s potential for disease monitoring.
3.6. Mechanistic Insights into Transformation Signaling
Investigation of the molecular mechanisms underlying serum-induced transformation revealed critical roles for HGF/c-MET and IGF/IGF-1R pathways. Using pooled human and murine ovarian cancer sera, we observed that pharmacological inhibition of c-MET (AMG337) and IGF-1R (PPP) significantly attenuated AIG colony formation (Figure 6A). Western blot analysis demonstrated that cancer serum induced 2.8-fold and 2.5-fold activation of IGF-1R and c-MET autophosphorylation, respectively, with corresponding downstream AKT phosphorylation. These activation patterns were reduced by 30–50% with pathway-specific inhibitors (Figure 6B), confirming these receptors as key mediators of the observed transformation activity.
4. Discussion
The present study establishes the TY-AIG assay as a sensitive and specific biotest for detecting cancer-associated transforming activity in serum, offering a novel approach to ovarian cancer diagnosis by measuring anchorage-independent growth (AIG), a hallmark of malignancy.
4.1. Development and Optimization of TY Cells
TY cells, generated through sequential transduction of fallopian tube epithelial cells with HPV16 E6/E7 and hTERT, exhibited progressive genomic instability [13], culminating in heightened sensitivity to cancer serum-derived transforming signals. Notably, passage 96 TY cells demonstrated optimal discriminative capacity, forming significantly more AIG colonies in response to cancer sera (68.50 ± 2.12) compared to normal female (17.50 ± 3.54) and male (22.50 ± 3.54) sera (Figure 2B). Beyond passage 123, TY cells lost specificity, responding excessively even to normal sera, underscoring the importance of passage number standardization for diagnostic consistency. Table 1 showed AIG count of non-cancer female and male. Comparative testing of other precancerous and cancerous cell lines (e.g., A549, MDA-MB-231, FT282V-CCNE1) revealed that most either failed to discriminate cancer sera or exhibited constitutive AIG activity. In contrast, TY cells uniquely distinguished cancer from normal sera, supporting their utility as a selective biosensor.
4.2. Advancing Cancer Diagnostics Beyond Traditional Biomarkers
Serum tests for solid tumors (e.g., ovarian cancer CA125) rely on indirect markers with limited early-stage sensitivity and specificity due to interference from benign conditions. This contrasts with hematologic malignancies like multiple myeloma, where secreted proteins (e.g., M-proteins [4]) serve as direct indicators. The TY-AIG assay bridges this gap by quantifying functional transforming activity—a direct malignancy readout. Clinically, TY-AIG correlated significantly with CA125 (r = 0.73, p = 0.03) and outperformed it in ROC analysis (AUC 0.87 vs. 0.75), achieving 75% sensitivity and 81% specificity at a cutoff of 23.75 colonies. Critically, the induction of AIG by sera from ovarian and breast cancer patients (Figure 3B) and ovarian cancer mice (Figure 5C) indicates that systemic release of oncogenic factors is a conserved feature of cancer across species.
4.3. Mechanistic Basis of TY-AIG: HGF/c-MET and IGF/IGF-1R Signaling
Early mechanistic studies identified key receptor tyrosine kinase (RTK) pathways—specifically IGF2/IGF-1R, HGF/cMET, and EGFR signaling—as mediators of follicular fluid (FF)-induced transformation in fallopian tube epithelial cells [13,14,15]. Building on this, the present study demonstrates the critical role of cMET and IGF-1R signaling in cancer serum-induced anchorage-independent growth (AIG). This finding aligns with established clinical evidence in ovarian cancer: elevated serum HGF levels decrease upon chemotherapy [19], and tumor tissues exhibit a three-fold increase in IGF2 expression compared to normal tissue, correlating with poorer prognosis [20]. The broader oncological relevance of IGF and HGF signaling is well-documented [21,22]. For instance, circulating IGF2 levels associate with increased risk of ER-positive breast cancer [23], while tissue HGF overexpression correlates with lymph node metastasis and serves as a prognostic indicator in breast cancer [24]. Collectively, these observations suggest that the systemic release of AIG-promoting growth factors is a common feature of malignancy. The TY-AIG assay quantitatively measures this transforming activity, positioning it as a promising diagnostic tool with potential prognostic applications across cancer types.
4.4. Limitations and Future Directions
Although the TY cell AIG assay demonstrates considerable diagnostic potential, several limitations should be noted. First, the modest sample size of both cancer and control cohorts, combined with the hospital-based case–control design, may limit the generalizability of our findings to broader populations. Second, potential confounding factors such as menstrual cycle phase, endometriosis associated tissue injury, or other physiological stressors were not accounted for in the current study, and their potential influence on AIG measurements remains to be determined. These limitations highlight the need for: (1) larger-scale, population-based validation studies; (2) systematic investigation of physiological variables affecting assay performance; and (3) standardization of testing protocols across multiple research centers to establish reproducibility.
5. Conclusions
In conclusion, we have developed a novel TY cell-based bioassay that sensitively detects malignant transformation activity in human serum through quantification of AIG. The strong correlation between AIG activity and both established biomarkers (e.g., CA125) and actual tumor burden substantiates the clinical utility of this approach. Mechanistically, the assay captures fundamental oncogenic processes mediated by IGF and HGF signaling pathways. These features, combined with the assay’s robust performance characteristics, suggest it may have broad applicability for cancer detection beyond ovarian cancer, pending further validation. Future studies should focus on expanding its clinical implementation while addressing the current technical and methodological limitations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Safaeian M. Solomon D. Castle P.E. Cervical Cancer Prevention—Cervical Screening: Science in Evolution Obstet. Gynecol. Clin. N. Am.20073473976010.1016/j.ogc.2007.09.004PMC 276235318061867 · doi ↗ · pubmed ↗
- 2Doubeni C.A. Corley D.A. Quinn V.P. Jensen C.D. Zauber A.G. Goodman M. Johnson J.R. Mehta S.J. Becerra T.A. Zhao W.K. Effectiveness of Screening Colonoscopy in Reducing the Risk of Death from Right and Left Colon Cancer: A Large Community-Based Study Gut 20186729129810.1136/gutjnl-2016-31271227733426 PMC 5868294 · doi ↗ · pubmed ↗
- 3Stewart C. Ralyea C. Lockwood S. Ovarian Cancer: An Integrated Review Semin. Oncol. Nurs.20193515115610.1016/j.soncn.2019.02.00130867104 · doi ↗ · pubmed ↗
- 4Szabo A.G. Klausen T.W. Abildgaard N. Gregersen H. Silkjær T. Pedersen P.T. Pedersen R.S. Helleberg C. Hermansen E. Schnack B.I. Incidence and Clinical Characteristics of Multiple Myeloma with Low M-Protein Levels and Normal Values of Hemoglobin, Creatinine, Calcium, and Serum Free Light Chain Ratio Blood Cancer J.2021117010.1038/s 41408-021-00460-033828079 PMC 8027460 · doi ↗ · pubmed ↗
- 5Hilgers R.D. Lewis J.L.Jr. Gestational Trophoblastic Neoplasms Gynecol. Oncol.1974246047510.1016/0090-8258(74)90055-94376997 · doi ↗ · pubmed ↗
- 6Abelev G.I. Alpha-Fetoprotein in Ontogenesis and Its Association with Malignant Tumors Adv. Cancer Res.19711429535810.1016/s 0065-230x(08)60523-04107670 · doi ↗ · pubmed ↗
- 7Wang H. Liu P. Xu H. Dai H. Early Diagnosis of Ovarian Cancer: Serum HE 4, CA 125, and ROMA Model Am. J. Transl. Res.202113141411414835035759 PMC 8748147 · pubmed ↗
- 8Menon U. Gentry-Maharaj A. Burnell M. Singh N. Ryan A. Karpinskyj C. Carlino G. Taylor J. Massingham S.K. Raikou M. Ovarian Cancer Population Screening and Mortality After Long-Term Follow-Up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A Randomised Controlled Trial Lancet 20213972182219310.1016/S 0140-6736(21)00731-533991479 PMC 8192829 · doi ↗ · pubmed ↗