Risk Factors for Long-Term Delayed Gastric Emptying and Its Impact on the Quality of Life After Laparoscopic Pylorus-Preserving Gastrectomy in Patients with Gastric Cancer: Secondary Analysis of the Prospective Multicenter Trial KLASS-04
Young Shick Rhee, Sang Soo Eom, Bang Wool Eom, Dong-eun Lee, Sa-Hong Kim, Hyuk-Joon Lee, Young-Woo Kim, Han-Kwang Yang, Do Joong Park, Sang Uk Han, Hyung-Ho Kim, Woo Jin Hyung, Ji-Ho Park, Yun-Suhk Suh, Oh Kyoung Kwon, Wook Kim, Young-Kyu Park, Hong Man Yoon, Sang-Hoon Ahn

TL;DR
This study found that patients without prior abdominal surgery are at higher risk for long-term delayed gastric emptying after a specific type of stomach cancer surgery, which negatively affects their quality of life.
Contribution
The study identifies previous abdominal surgery as a novel protective factor against long-term delayed gastric emptying after pylorus-preserving gastrectomy.
Findings
Patients without previous abdominal surgery had a 32% incidence of DGE compared to 4.8% in those with prior surgery.
DGE was associated with more symptoms like nausea, vomiting, constipation, and dry mouth.
DGE significantly reduced the quality of life for patients despite avoiding known risk factors.
Abstract
Delayed gastric emptying (DGE) is a well-known complication of laparoscopic pylorus-preserving gastrectomy (LPPG). Patients who underwent LPPG in the KLASS-04 trial showed an unneglectable incidence—21/124 patients (16.3%)—of long-term DGE compared to those who underwent laparoscopic distal gastrectomy. This study aimed to identify the multifactorial risk factors associated with DGE and analyze the quality of life (QoL) of patients with DGE following LPPG. Patients without previous abdominal surgery had a higher incidence of DGE in the univariate (32% vs. 4.8%, p = 0.011) and logistic regression analyses (odds ratio: 0.106, 95% confidence interval: 0.014–0.824, p = 0.032). Patients with DGE reported more symptoms of nausea and vomiting (p = 0.004), constipation (p = 0.04), and a dry mouth (p = 0.005). No clinicopathological or surgical factors, other than the absence of a previous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
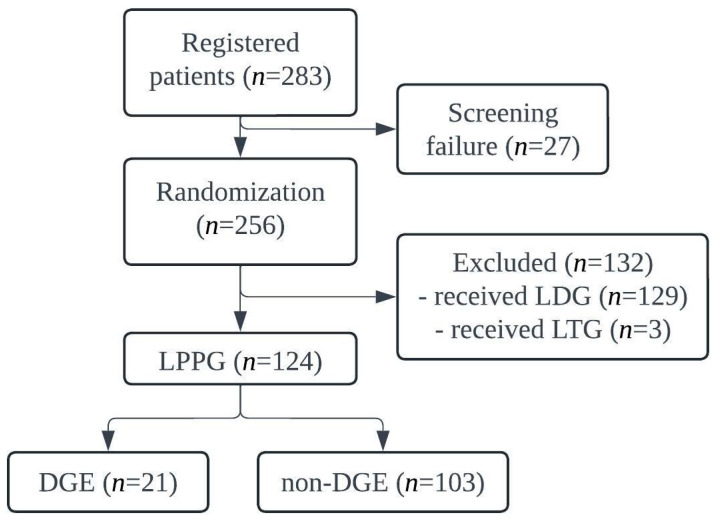 Figure 1
Figure 1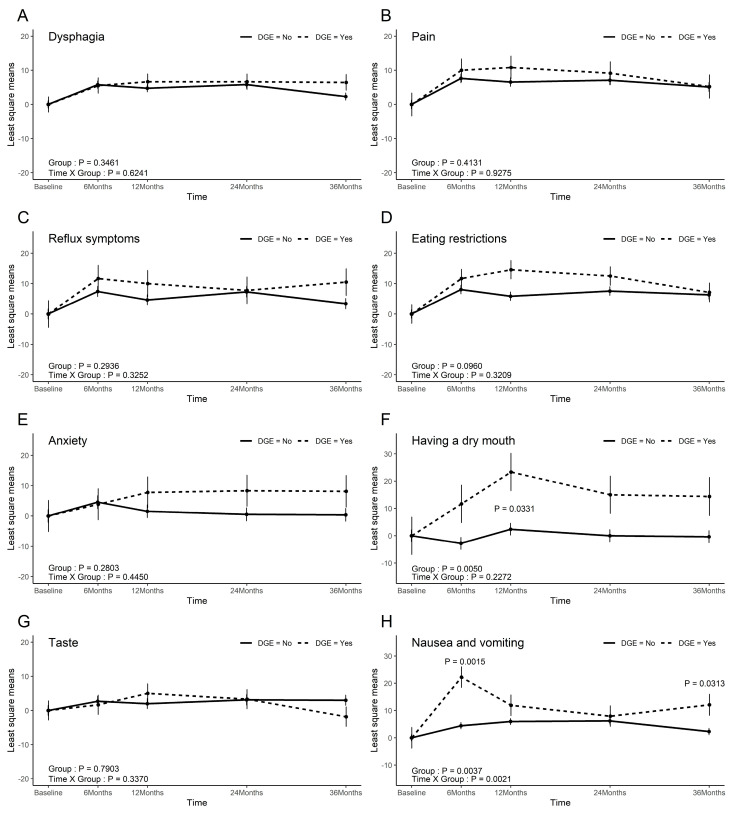 Figure 2
Figure 2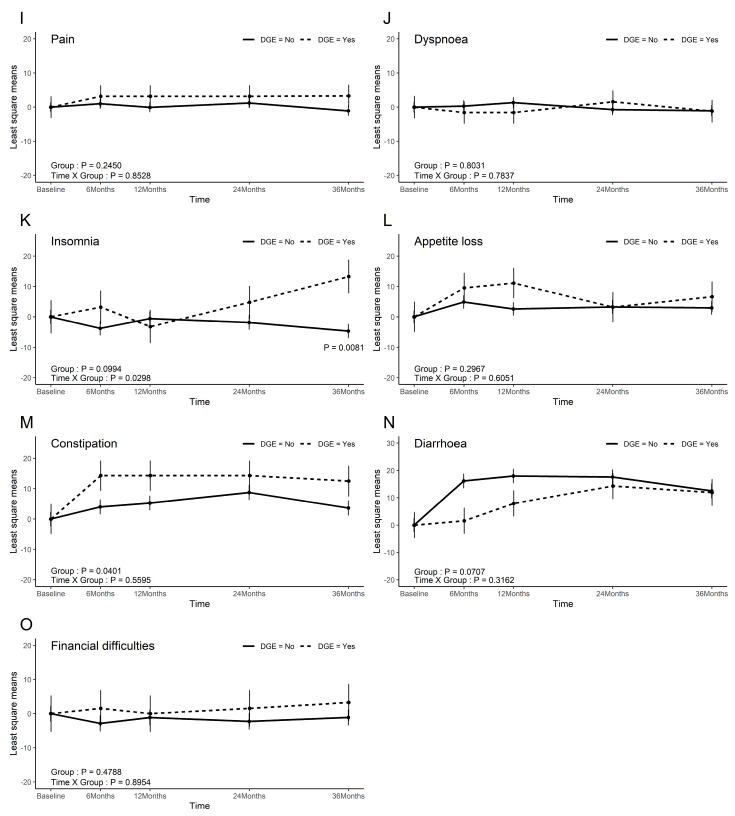 Figure 3
Figure 3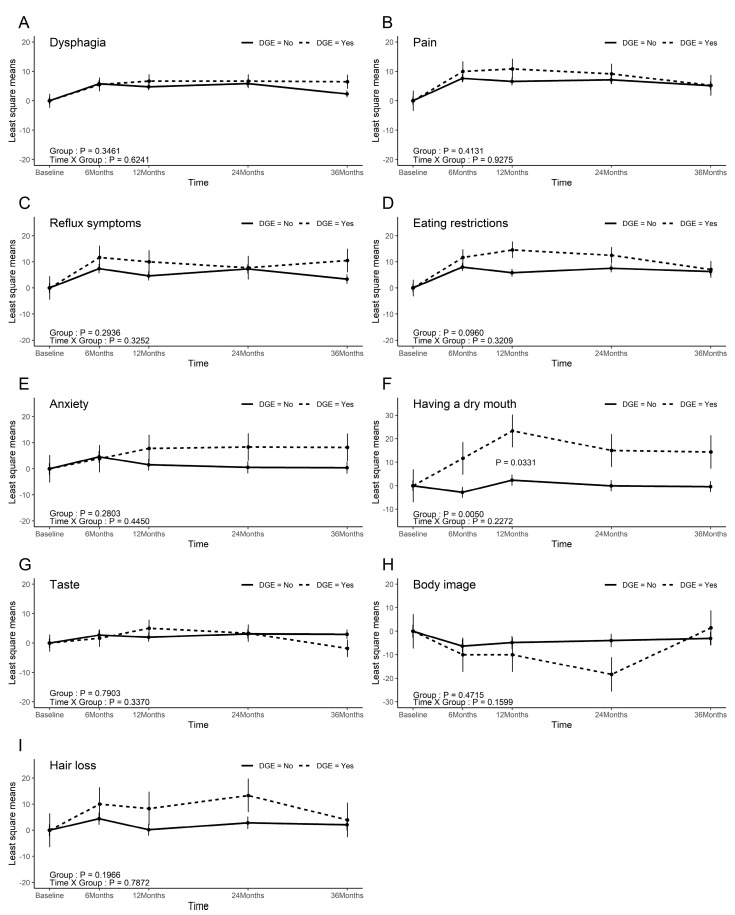 Figure 4
Figure 4- —National Cancer Center of the Republic of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Helicobacter pylori-related gastroenterology studies · Metastasis and carcinoma case studies
1. Introduction
Gastric cancer is the fifth most common cancer worldwide, and was the fourth most common cancer in Korea as of 2021, accounting for 10.6% of all cancers [1,2]. The national screening programs for gastric cancer are well organized in Korea and Japan because of the high incidence rate of gastric cancer in these countries; consequently, most gastric cancers are diagnosed at an early stage, with EGC accounting for 63.1% of all diagnoses in Korea in 2023 [3].
Since the survival rate of surgically treated early gastric cancer (EGC) is >90%, several surgical options are currently being investigated to improve the quality of life (QoL) of patients, which is impaired after standard gastrectomy, such as when postgastrectomy syndrome occurs [4]. Pylorus-preserving gastrectomy (PPG), initially devised for the treatment of peptic ulcer disease, is currently endorsed as an alternative surgical approach for clinical T1N0 EGC located in the middle third of the stomach, provided that a minimum distance of 4 to 5 cm is maintained above the pylorus. This recommendation is supported by the guidelines of the Korean Gastric Cancer Association, the Japanese Gastric Cancer Association, and the Chinese Society of Clinical Oncology, with the expectation of preserving the function of the pylorus. The KLASS-04 trial, a prospective multicenter randomized control trial (RCT) comparing the outcomes of laparoscopic PPG (LPPG) and laparoscopic distal gastrectomy (LDG) for cT1N0M0 gastric cancer in the mid-portion of the stomach, showed that LPPG has more favorable outcomes in terms of nutritional status, gallstone formation, and bile reflux compared to LDG, but has the pitfalls of delayed gastric emptying (DGE) and esophageal reflux [5].
DGE, a well-known drawback of PPG, can mostly be treated with diet modification and conservative medical treatment; however, it not only impairs the QoL of patients, but it also sometimes requires additional interventions for management. Several individual risk factors for DGE have been reported, such as damage to the hepatic branch of the vagus nerve (HBVN) [6], infrapyloric artery (IPA) [7], infrapyloric vein (IPV) [8], and short antral cuff [9]; however, these factors interact with one another, and cannot be attributed to a single factor. These well-known factors were considered in the study protocol, and the surgical procedure was well controlled to prevent DGE in the KLASS-04 trial.
In this study, the KLASS-04 trial data underwent secondary analysis to determine the multifactorial risk factors for DGE, evaluate its impact on patient QoL, and improve surgical outcomes after LPPG. Patients who underwent LPPG were categorized into DGE and non-DGE groups.
2. Materials and Methods
2.1. Study Design and Patients
The patient inclusion criteria for the KLASS-04 trial were the following: (1) an age between 20 and 80 years, with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; (2) histologically confirmed gastric adenocarcinoma; (3) a preoperative diagnosis of cT1N0M0 using gastroscopy, endoscopic ultrasound, and abdominal computed tomography; and (4) a tumor proximal/distal margin of at least 5 cm from the gastroesophageal junction/pylorus.
Patients with a history of other cancers, synchronous EGC or adenoma of the antrum, previous gastric surgery—including gastrojejunostomy—or the presence of other malignancies within the previous 5 years (except for cured basal cell carcinoma or in situ cervical cancer) were excluded.
Surgeon qualification was determined based on the following criteria: (1) a minimum of 50 surgeries performed for both LDG and open distal gastrectomy; (2) experience with at least five cases of LPPG; and (3) affiliation with an institution performing a minimum of 80 gastrectomy procedures annually.
The surgical procedure of LPPG was standardized as detailed below.
Dissection of the #6 lymph nodes was carried out meticulously to preserve the infrapyloric vessels. Dissection of the #5 lymph nodes was omitted, and the right gastric artery arcade was ligated at a point 3 cm proximal to the pylorus. Gastro-gastrostomy was performed using an extracorporeal hand-sewn anastomosis technique.
In accordance with the KLASS-04 criteria, DGE was defined as “nearly normal diet residue” at least once in the endoscopic follow-up at 1, 2, and 3 years after the surgery [5].
The primary hypothesis was that there would be differences in the clinicopathological features and surgical outcomes between the two groups. The secondary hypothesis was that the QoL would be worse in the DGE group than in the non-DGE group.
The clinicopathological features analyzed included age, sex, body mass index (BMI), ECOG, diabetes mellitus (DM), history of a previous abdominal operation, tumor location, tumor size, pathological stage and final stage, lymph node (LN) dissection level, and surgical outcomes—including the operation time, intraoperative bleeding amount, IPA type and injury, HBVN injury, length of the remaining antral cuff, distance of the distal margin to the pylorus, proximal and distal margin of the tumor, preservation of the celiac branch of the vagus nerve, number of resected #6 LNs and total LNs, and overall morbidity.
QoL analysis was performed using the EORTC C30 and STO22 questionnaire surveys, which were administered preoperatively and at 6 months, 1, 2, and 3 years after the surgery.
2.2. Statistical Analysis
To compare the distribution based on the presence of DGE, the Chi-square test or Fisher’s exact test was performed for categorical variables, and the Wilcoxon rank sum test was used to analyze continuous variables. Logistic regression analysis was performed to identify the factors affecting DGE and to estimate the odds ratios (ORs) with 95% confidence intervals (CIs). Generalized linear mixed models were used for the QoL analysis. The primary index of the QoL analysis was the group p-value rather than the group × time interaction p-value, since the primary objective was to evaluate the differences in QoL scores between the groups across all time points, rather than differences in temporal trends. The analysis was conducted by comparing the changes in QoL at each time point with the baseline. Statistical significance was set at p < 0.05, and statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and R version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Patient Recruitment
A total of 283 patients were enrolled in the KLASS-04 trial. After excluding 27 screening failures, 256 patients were randomized to the LDG or LPPG arm. After excluding 129 patients who underwent LDG and three patients who underwent laparoscopic total gastrectomy, 124 patients who underwent LPPG were included in the secondary analysis. Among them, 21 were diagnosed with DGE, while 103 exhibited no endoscopic findings indicative of DGE (Figure 1).
3.2. Clinicopathological Features
Patients without a history of surgery showed a higher incidence of DGE (32% vs. 4.8%, p = 0.013; Table 1). The BMI and presence of underlying DM did not differ significantly between the two groups (23.5 vs. 23.6, p = 0.8964 and 8.7% vs. 4.8%, p = 0.468, respectively). No significant differences were observed in either the pT classification or the pathological stage of the disease (p = 0.853, p = 0.504).
3.3. Surgical Outcomes
No significant differences in operative details were found between the two groups (Table 2).
The previously known risk factors for DGE after LPPG, namely injury to the HBVN, IPA, and IPV and antral cuff length, showed no difference between the two groups (2% vs. 4.8%, p > 0.99; 1% vs. 0%, p > 0.99; 3.9% vs. 0%, p > 0.99; 4 vs. 4, p = 0.9194, respectively). The number of resected LNs, including #6 LNs, #9 LNs, and total LNs, also showed no significant differences (6 vs. 5, p = 0.526; 2 vs. 2.5, p = 0.471; 49 vs. 39, p = 0.113). Intraoperative bleeding did not differ significantly between the groups (31.5 mL vs. 50 mL, p = 0.2475). The mean operation time demonstrated a nearly significant difference, with the DGE group exhibiting shorter operation times compared to the non-DGE group (190 min vs. 199 min, p = 0.08).
3.4. Logistic Regression Analysis
Univariate logistic regression was performed to determine whether clinicopathological characteristics and surgical factors affected DGE (Table 3). Patients with a history of previous abdominal surgery showed a lower tendency for DGE in both the univariate and multivariate analyses (OR: 0.106, 95% CI: 0.014–0.824, p = 0.032; OR: 0.094, 95% CI: 0.012–0.757, p = 0.026, respectively). The operative time and number of resected LNs showed marginal tendencies toward DGE in the univariate analysis. The operative time was slightly shorter in the DGE group than in the non-DGE group, while the number of resected LNs was slightly higher (OR: 0.989, 95% CI: 0.977–1.002, p = 0.093; OR: 1.029, 95% CI: 0.997–1.061, p = 0.074, respectively).
3.5. QoL
In the EORTC C30, patients with DGE exhibited more nausea and vomiting (p = 0.004) and constipation (p = 0.04). Insomnia exhibited nearly-significant differences between the groups (p = 0.099), and the time × group interaction analysis indicated a trend toward worsening insomnia in the DGE group compared with the non-DGE group (p = 0.03). There were no significant differences in the other scales (Figure 2).
In the EORTC STO22, aside from dry mouth (p = 0.005), no significant differences were observed between the two groups. While the eating restriction score demonstrated a marginally significant difference between the groups (p = 0.096), no significant differences were noted at the 3-year follow-up (Figure 3).
4. Discussion
The design of the LPPG surgical protocol considered previously identified individual risk factors, including injury to the HBVN, IPA, and IPV and a short antral cuff length, as well as the qualifications of the operating surgeon. Despite these considerations, the incidence of DGE was significantly higher in the LPPG cohort than in the LDG group, with rates of 16.3% and 3.9%, respectively (p = 0.001). This study was performed to identify the multifactorial risk factors for DGE and analyze the impact of DGE on the QoL of patients who underwent LPPG in the KLASS-04 trial. Although novel risk factors were not identified, except for a previous history of abdominal surgery, this study demonstrates the negative effect of DGE on patient QoL. This is the first comprehensive analysis using data from a prospective RCT of DGE after LPPG.
Because patients with prior gastric surgeries were excluded from the study, the history of previous abdominal surgeries primarily involved colonic or gynecological procedures, which likely had a minimal direct impact on LPPG. None of the patients underwent pancreatic or hepatic surgery. The absence of previous surgeries, along with shorter operation times, was associated with a higher incidence of DGE with marginal statistical significance in the univariate analysis, suggesting that less radical surgical interventions may be correlated with long-term DGE outcomes.
Despite high BMI being implicated as a risk factor for DGE [10], our analysis revealed no significant difference in BMI between the DGE and non-DGE groups, possibly attributable to the lower prevalence of overweight individuals in the Korean population. Furthermore, DM, which is recognized as a risk factor for general gastroparesis [11], did not increase the risk of DGE after LPPG. The lack of significant differences in previously established individual risk factors between patients who did and did not develop DGE suggests that adherence to the initial surgical protocol was maintained throughout the study. Future investigations are warranted to elucidate the pathophysiological mechanisms underlying DGE following LPPG to improve surgical outcomes.
In the QoL analysis, patients with DGE experienced more nausea and vomiting and constipation. Given the relatively young average age of patients undergoing LPPG (55.7 years), the risk of aspiration due to vomiting was lower; however, the high incidence of DGE associated with LPPG, which is correlated with increased vomiting, makes this procedure less advisable for older patients.
In the KLASS-04 study, only 2 out of the 21 patients with endoscopic evidence of food retention were clinically diagnosed with DGE at the same time. Furthermore, 14 out of the 16 patients that were clinically diagnosed with DGE did not exhibit “nearly normal food residue” on concurrently performed endoscopy. This discrepancy is consistent with the results of previous studies, wherein the presence of residual food during endoscopy does not reliably correlate with clinical DGE [12]. Nevertheless, this does not negate the utility of endoscopy as a diagnostic modality for DGE, as patients with endoscopically defined DGE experience several statistically significant or near-significant DGE-related symptoms, including nausea and vomiting, constipation [13], and eating restrictions, as evidenced by the QoL analysis.
Among the 21 patients who demonstrated endoscopic evidence of food retention, 17 cases were observed in the first year of follow-up, 10 cases in the second year, and only one case was noted in the third years. This decreasing trend is consistent with previous studies [14], suggesting that DGE typically improves over time.
Our study has several limitations. First, DGE was not defined based on clinical symptoms corroborated by gastric scintigraphy, but was rather defined through endoscopic findings. Gastric scintigraphy requires several hours to perform and precise timing, which poses challenges in an outpatient setting. Therefore, endoscopy—a routine follow-up examination after gastric cancer surgery—was utilized as the diagnostic tool. Second, the surgical protocol for LPPG in the KLASS-04 trial involved extracorporeal anastomosis, following earlier studies reporting higher rates of DGE with intracorporeal anastomosis [15]. However, more recent evidence suggests that intracorporeal anastomosis demonstrates outcomes comparable to those obtained with extracorporeal techniques [16], and it is increasingly being adopted as a standard practice. Third, the sample size of 124 patients was insufficient to achieve a statistical power of 80% for this analysis. This limitation may have contributed to the negative findings of the study. Therefore, further research with a larger cohort is warranted to validate these results.
5. Conclusions
Despite the strict surgical protocol and procedure, considering well-known individual risk factors for DGE and surgeon qualifications, the LPPG group of the KLASS-04 trial exhibited a considerable incidence of DGE. No clinicopathological or surgical factors, other than the absence of a previous surgical history, were identified as multifactorial risk factors for DGE; however, given the negative impact of DGE on patient QoL, further research is necessary to develop strategies to improve outcomes in DGE following LPPG.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Park S.H. Kang M.J. Yun E.H. Jung K.W. Epidemiology of Gastric Cancer in Korea: Trends in Incidence and Survival Based on Korea Central Cancer Registry Data (1999–2019)J. Gastric Cancer 20222216016810.5230/jgc.2022.22.e 2135938363 PMC 9359882 · doi ↗ · pubmed ↗
- 3Kim D.J. Song J.H. Park J.H. Kim S. Park S.H. Shin C.M. Kwak Y. Bang K. Gong C.-S. Oh S.E. Korean Gastric Cancer Association-Led Nationwide Survey on Surgically Treated Gastric Cancers in 2023 J. Gastric Cancer 20252511513210.5230/jgc.2025.25.e 839822171 PMC 11739641 · doi ↗ · pubmed ↗
- 4Mc Call M.D. Graham P.J. Bathe O.F. Quality of life: A critical outcome for all surgical treatments of gastric cancer World J. Gastroenterol.2016221101111310.3748/wjg.v 22.i 3.110126811650 PMC 4716023 · doi ↗ · pubmed ↗
- 5Lee H.J. Kim Y.W. Park D.J. Han S.U. Ryu K.W. Kim H.H. Hyung W.J. Park J.-H. Suh Y.-S. Kwon O.-K. Laparoscopic Pylorus Preserving Gastrectomy versus Distal Gastrectomy for Early Gastric Cancer; A Multicenter Randomized Controlled Trial (KLASS-04)Ann. Surg.202428157358110.1097/SLA.000000000000650339219553 · doi ↗ · pubmed ↗
- 6Nunobe S. Sasako M. Saka M. Fukagawa T. Katai H. Sano T. Symptom evaluation of long-term postoperative outcomes after pylorus-preserving gastrectomy for early gastric cancer Gastric Cancer 20071016717210.1007/s 10120-007-0434-717922094 · doi ↗ · pubmed ↗
- 7Shibata C. Saijo F. Kakyo M. Kinouchi M. Tanaka N. Sasaki I. Aikou T. The Society for the Study of Postoperative Morbidity After Gastrectomy Current Status of Pylorus-Preserving Gastrectomy for the Treatment of Gastric Cancer: A Questionnaire Survey and Review of Literatures World J. Surg.20123685886310.1007/s 00268-012-1491-622350486 · doi ↗ · pubmed ↗
- 8Kiyokawa T. Hiki N. Nunobe S. Honda M. Ohashi M. Sano T. Preserving infrapyloric vein reduces postoperative gastric stasis after laparoscopic pylorus-preserving gastrectomy Langenbeck’s Arch. Surg.2017402495610.1007/s 00423-016-1529-627815708 · doi ↗ · pubmed ↗