Respiratory outcomes of adrenergic beta-antagonists in patients undergoing tracheal extubation: a systematic review and meta-analysis of randomized controlled trials
Lucas Cael Azevedo Ramos Bendaham, Altair Pereira de Melo Neto, Hilária Saugo Faria, André Richard da Silva Oliveira Filho, Carlos Henrique de Oliveira Ferreira, Marcela da Silva Kazitani Cunha, Victor Gonçalves Soares, Ocílio Ribeiro Gonçalves, Milene Vitória Sampaio Sobral

TL;DR
This study finds that beta-blockers reduce cough and hypertension during tracheal extubation after anesthesia, with no significant increase in bronchospasm or bucking.
Contribution
A systematic review and meta-analysis showing beta-blockers' effectiveness in reducing peri-extubation complications.
Findings
Beta-blockers significantly reduced moderate/severe cough compared to placebo.
Hypertension risk was also significantly lower in the beta-blocker group.
No significant differences were found in bronchospasm or bucking between groups.
Abstract
Tracheal extubation after general anesthesia may cause hemodynamic and respiratory complications, with no established strategies to prevent them. We conducted a meta-analysis to evaluate the safety and efficacy of beta-blockers in patients undergoing tracheal extubation. We searched the MEDLINE, EMBASE and CENTRAL databases for randomized controlled trials up to 2024 comparing beta-blockers to placebo in patients undergoing tracheal extubation. Primary outcome: cough intensity; secondary: bronchospasm, bucking, hypertension. Risk Ratios (RR) with 95% Confidence Intervals (95% CI) were computed. Leave-one-out sensitivity and meta-regression analyses were performed for outcomes with high heterogeneity. We included 31 randomized studies, comprising 1,803 patients, of whom 965 received beta-blockers. The risk of moderate/severe cough (RR = 0.21; 95% CI 0.13 to 0.34; p < 0.001; I2 = 0%)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
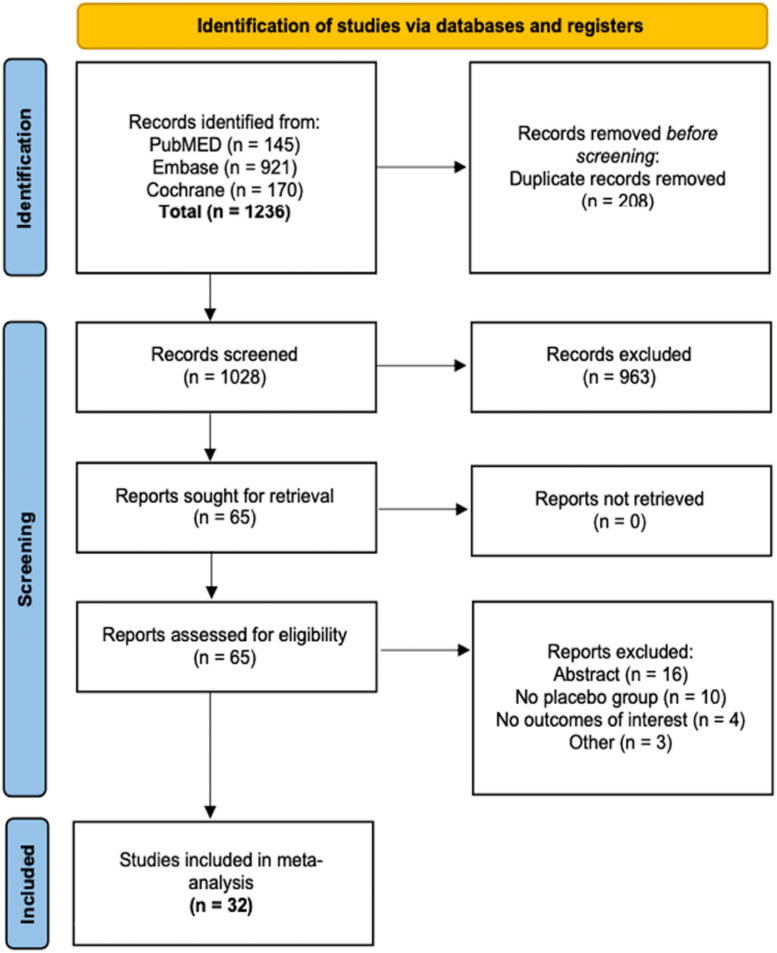 Figure 1
Figure 1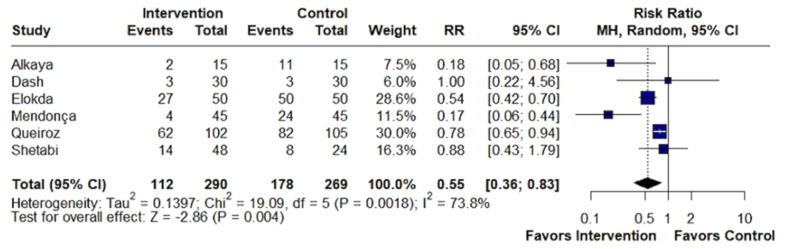 Figure 2
Figure 2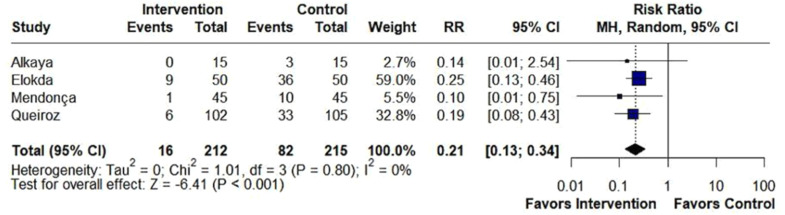 Figure 3
Figure 3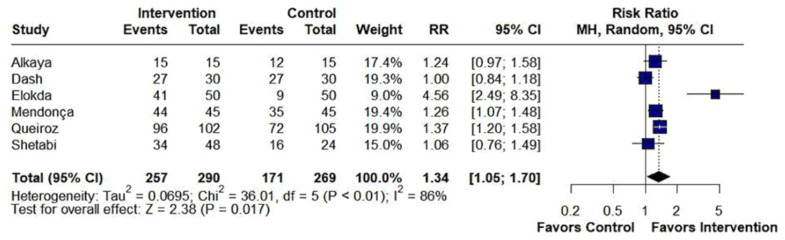 Figure 4
Figure 4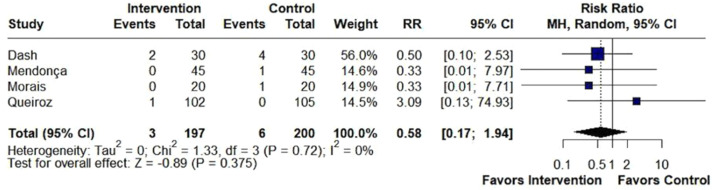 Figure 5
Figure 5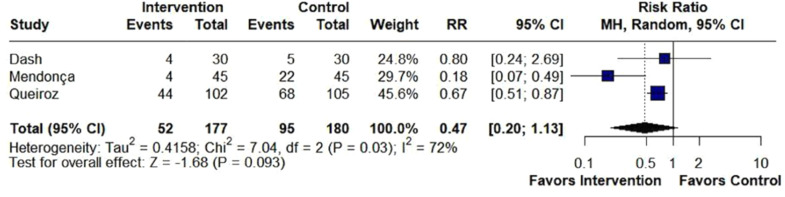 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Family and Patient Care in Intensive Care Units · Respiratory Support and Mechanisms
Introduction
Extubation is a procedure frequently used in surgeries performed under general anesthesia. Complications from this procedure may affect more than one-third of patients. Cough is a common complication, mainly due to the activation of irritant receptors in the tracheal mucosa, causing a contraction of the smooth muscle in the airways and consequently triggering the cough reflex and bronchospasm.1^,^2 As a result, there may be an exacerbated hemodynamic responses, leading to cardiovascular and respiratory decompensations.3, 4, 5 This occurs due to the stimulation of the sympathoadrenal reflex, with a concomitant increase in plasma catecholamine levels and activation of alpha and beta-adrenergic receptors.6 The development of this response necessitates immediate interventions to reduce the risk of potentially fatal complications such as acute myocardial infarction, arrhythmias, congestive heart failure, and other target organ damage.6^,^7
Despite these concerns, pharmacological guidelines to control cardiovascular and respiratory decompensations during the peri-extubation period have not yet been developed. In this context, recent studies are investigating the potential use of prophylactic beta-blockers to reduce cardiovascular and respiratory responses and the risk of complications after the procedure.8 By counteracting sympathetic activation during acute stress through their antagonistic action on beta-1 receptors, these medications may prevent a hyperdynamic state throughout the tracheal extubation phase without prolonging the recovery phases.9, 10, 11, 12
The efficacy and safety of beta-blockers during tracheal extubation remain uncertain.12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42 Individual trials lack sufficient power to detect significant differences in outcomes and adverse events. To address these limitations, this meta-analysis pools data from multiple Randomized Controlled Trials (RCTs) to enhance statistical power and provide robust conclusions on the efficacy and safety of beta-blockers in tracheal extubation.
Material and methods
This systematic review and meta-analysis were conducted in accordance with the Cochrane Collaboration and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines and followed the methodological recommendations outlined in the Cochrane Handbook for Systematic Reviews of Interventions.43^,^44 The protocol of this study was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42024542103).
Search strategy and data extraction
We systematically searched in databases of MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to April 25^th^, 2024, with the search terms presented in Supplementary Table 1. The titles and abstracts were first reviewed. Studies that did not satisfy the inclusion criteria were excluded, and all abstracts deemed potentially eligible were obtained in full text and assessed to confirm their inclusion. The entire screening process was conducted independently by two authors (L.B. and A.N.), followed by a comparison of decisions. Any discrepancies in decisions were resolved by a third independent author. Four authors (A.F., M.C., H.F. and C.F.) independently organized and extracted the data, using standardized tables for accuracy, following predefined search criteria and quality assessment. Disagreements were resolved by consensus between the authors.
Eligibility criteria
We included studies that fulfilled the following eligibility criteria: (1) Randomized Controlled Trials (RCTs) published in the indexed databases; (2) Studies comparing adrenergic beta-antagonists with placebo; (3) trials involving patients undergoing tracheal extubation; and (4) Studies assessing extubation-related complications using validated clinical scales or predefined hemodynamic parameters. We excluded studies based on the following criteria: (1) Lack of a control group; (2) Overlapping patient populations; (3) Trials not involving patients undergoing tracheal extubation; and (4) Administration of the drug solely during anesthetic induction, with no relevance to tracheal extubation outcomes.
Outcomes and subgroups
Primary outcomes were the incidence of cough and its severity, classified as no/mild cough, and moderate/severe cough. Secondary outcomes included Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Mean Arterial Pressure (MAP), Mean Heart Rate (MHR), risk of bronchospasm, hypertension, hypotension, tachycardia, bradycardia, postoperative nausea or vomiting, and bucking, defined as a situation in which a patient is trying to cough and strain on an endotracheal tube and has violent expiratory contraction of skeletal muscles secondary to endotracheal tube stimulation of the tracheal mucosa.
Sub-analyses included data restricted to the time of outcome measurement after extubation (at extubation, 1-minute, 2 minutes, 5 minutes, 10 minutes, and 15 minutes or more).
Quality assessment
Quality assessment of RCTs was performed using the Cochrane Collaboration’s tool for assessing the risk of Bias in Randomized trials (RoB-2). Studies were scored as high, low, or unclear risk of bias in 5 domains: selection, performance, detection, attrition, and reporting biases.45 Bias risk assessment was conducted independently by two authors (A.N and O.G.). Discrepancies were resolved through consensus among the authors. Publication bias was assessed with contour-enhanced funnel plot analysis46 and Egger’s test47 of efficacy endpoints and evaluation for symmetrical distribution of trials with similar weights, using the Pustejovsky and Rodgers48 approach when the standardized mean difference was used for the outcome of interest.
Statistical analysis
Treatment effects were compared for binary outcomes using Risk Ratios (RR) with 95% Confidence Intervals (95% CI). Mean Differences (MD) with 95% CI were used to compare the treatment effects for continuous endpoints. Given the expected heterogeneity between studies, we adopted the DerSimonian and Laird random-effects model for all outcomes reported. We used the Cochrane Q test and I^2^ statistics to assess heterogeneity; p-values inferior to 0.1 and I^2^ > 40% were considered significant for heterogeneity.43 The p-values inferior to 0.05 were considered statistically significant. Funnel Plots with Egger’s test was used to address publication bias in every outcome and subgroup that had at least 10 studies. R version 4.4.0 and the “meta” extension package was used for all analyses.49
Sensitivity analysis
We performed a pre-specified sensitivity analysis for primary endpoints with (1) A leave-one-out approach to ensure that results were not dependent on a single study and to evaluate studies that had high contributions to the heterogeneity on primary endpoints when I^2^ ≥ 40; (2) Several univariable meta-regression analyses to assess any interactions with some covariates (time of drug administration; type of adrenergic beta-antagonist; age; American Society of Anesthesiologists physical status classification; type of surgery; preanesthetic medication; type of general anesthesia; baseline SBP, DBP, MAP, and MHR; duration of surgery and anesthesia) for the continuous outcomes reported by at least 9 studies. A multivariable meta-regression was not conducted to assess the robustness and validity of the findings due to the limited number of included studies and lack of statistical significance of multiple covariates. Current methodological guidelines recommend a minimum of 10 studies per covariate to ensure reliable estimates in multivariable meta-regression analyses.43
Results
Study selection and characteristics
As outlined in Figure 1, this study included 31 RCTs with a total of 1,803 patients, of whom 965 (53.5%) were assigned to the beta-blockers group and 838 (46.5%) to the placebo group.12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42 Among the interventions, 21 studies used esmolol, 4 labetalol, 3 used metoprolol, 1 landiolol, 1 atenolol, and 1 propranolol. The mean age of patients across studies ranged from 31.2 to 69 years, and the percentage of female patients ranged from 14.28% to 100%. At baseline, MAP ranged from 30.05 to 124.20 and MHR ranged from 52.74 to 98.76. Detailed baseline characteristics of the included studies can be found in Table 1. Given the heterogeneity in pharmacologic properties and clinical application of these agents, we present in Supplementary Table 2 a descriptive summary of their key characteristics and relevance in the context of tracheal extubation based on the studies included in this meta-analysis.Figure 1PRISMA flow diagram of study screening and selection.Figure 1. Table 1Baseline characteristics of included studies.Table 1:StudyCountryInterventionPatients, n (I/C)Female, % (I/C)Agea, Y (I/C)Follow-upASA classificationPreanesthetic medicationWeight. Kga (I/C)Queiroz 2024BrazilMetoprolol (5 mg/20 mL)102/10552 / 5843.6 (15.1) / 47.1 (17)120 min after extubationI. II or IIIIntravenous midazolam (0.05 mg.kg^-1^)72.6 (14.6) / 69.8 (12.8)Mendonça 2023BrazilEsmolol (2 mg.kg^-1^)45/4553.3 / 64.449.2 (12.8) / 44.2 (15.1)10 min after extubationI. II or IIIIntravenous midazolam (0.05 mg.kg^-1^)68.9 (10.3) / 68.7 (9.7)Alkaya 2014USAEsmolol (0.2 μg.kg^-1^.min^-1^)15/1543.7 / 43.839.4 (10.7) / 45.0 (13.3)10 min after extubationI or IIIntravenous midazolam (0.05 mg.kg^-1^)NAArar 2007USALabetalol (0.15‒0.3 mg.kg^-1^)40/4057.5 / 6057.4 (8.0) / 59.2 (9.9)NAINA70.0 (15.3) / 70.6 (10.2)Hosseinzadeh 2013IranEsmolol (infusion at 0.5 mg.kg^-1^ 4 min before the extubation. followed by an infusion at 0.15 mg.kg^-1^.min^-1^ for 10 min after extubation)30/3050/7046.0 (16.2) / 49.0 (17)15 min after extubationI or IINA73.2 (10.3) / 71.6 (12.0)Chia 2004TaiwanEsmolol (0.2 μg.kg^-1^.min^-1^)49/48NA48.5 (30–79) / 49.8 (27–75)bPO + 72 hI or IINA57.4 (7.2) / 61.3 (10.6)Grillo 2003FranceEsmolol (0.3 mg.kg^-1^.min^-1^)15/15NA52 (10) / 47 (15)60 min after anesthesia with esmololI or IINA65 (10) / 68 (16)O'Dwyer 1993UKEsmolol (500 ng.kg^-1^ over l min followed by 100 ng.kg^-1^.min^-1^)7/7NA59.7 (5) / 58.8 (3.5)10 min after extubationNAEtomidate (fentanyl 5 μg. kg^-1^) and midazolam74.4 (3) / 82.8 (5.6)Kawaguchi. 2010JapanLandiolol (0.125 mg.kg^-1^.min^-1^ followed by an infusion at 0.01–0.04 mg.kg^-1^.min^-1^)15/1526.7/2060 (10) / 59 (8)10 min after extubationNANA58 (9) / 60 (9)Elokda 2015Arabi SauditaEsmolol (1 mg.kg^-1^ over 30 s followed 100 μg.kg^-1^.min^-1^)50/5055/6060 (3) / 62 (4)10 min after extubationI or IIBromazepam (3 mg) and ranitidine (150 mg)82.6 (6) / 85 (10)Kshama 2022IndiaEsmolol (0.5 mg.kg^-1^ and 1 mg.kg^-1^)40/2015/4039.3 (8.4) / 38.7 (11.9)10 min after extubationNANA62.8 (9.3) / 61.3 (7.9)Song 2021ChinaEsmolol (0.5 mg.kg^-1^ and 1.0 mg.kg^-1^)84/4138/3956 (10.9) / 56.9 (8.9)5 min after extubationI. II or IIINA67.4 (9.7) / 70.9 (10.6)Shetabi 2023IranLabetalol (0.1 mg.kg^-1^ or 0.2 mg.kg^-1^)48/2458.3/79.231.8 (10.7) / 33 (14.7)10 min after extubationI or IINA72.0 (8.3) / 69.9 (9.8)Dash 2023IndiaEsmolol (1 mg.kg^-1^)30/3053.3/46.637.1 (12.0) / 38.9 (12.5)30 min after extubationI or IINA61.5 (11.4) / 65.4 (10.9)Lim 2000SingaporeEsmolol (500 μg. kg^-1^. followed by esmolol infusions at 100 μg.kg^-1^.min^-1^ or 200 μg.kg^-1^.min^-1^)24/1245.8/66.7NA5 min after extubationI or IINANAMaharjan 2005NepalPropranolol (1 mg or 0.5 mg)42/2119.0/14.344.9 (15.8) / 35.8 (11.0)PO + 6 hI or IIDiazepam (5 mg), ranitidine (150 mg), and metoclopramide (10 mg)56.9 (8.9) / 60.9 (9.9)Morais 2020BrazilEsmolol (0.5 mg.kg^-1^ bolus followed by an infusion at 15 μg.kg^-1^.min^-1^)20/2085/8535.8 (10.9) / 33.2 (8.7)PO + 24 hII or IIIDipyrone (2 mg) and parecoxib (40 mg)105.6 (20.2) / 109.8 (11.2)Radwan 2016EgyptLabetalol (infusion in a rate of 0.5 mg.kg^-1^.hr^-1^)25/2544/3744 (6) / 40 (11)PO + 4 hI or IIRanitidine (50 mg), metoclopropramide (10 mg), and dexamethasone (0.15 mg.kg^-1^)80 (10) / 79 (11)Sohn 1995South KoreaEsmolol (1 mg.kg^-1^)30/3043.3/4036.3 (15.1) / 39.4 (16.4)4 min after extubationI or IIMidazolam (0.05 mg.kg^-1^)58.6 (6.9) / 58.5 (8.3)Felding 1994DenmarkMetoprolol (0.07 mg.kg^-1^)10/10NA56 (10) / 54 (12)PO + 180 min after extubationNADiazepam (0.2 mg.kg^-1^)NAVelayutham 2020IndiaAtenolol (50 mg)25/2524/3239 (11) / 38 (7)PO + 12 hI. II or IIIDiazepam (10 mg)61 (7) / 63 (5)Vandenberg 1997Saudi ArabiaEsmolol (4 mg.kg^-1^)20/2045/5068/64NAI. II or IIITemazepam (10 mg) VO64/63Unal 2008TurkeyEsmolol (0.1 mg.kg^-1^.min^-1^ or 0.2 mg.kg^-1^.min^-1^)30/1546.7/53.349.2 (16.4) / 50.3 (12.2)30 min after extubationI or IINA165.8(9.3) / 77.5(9.3)Ersin 2005TurkeyEsmolol (bolus dose at 1.5 mg.kg^-1^ for 30 seconds)15/1560/6041.7 (12.8) / 38.5 (12.2)10 min after extubationI or IINA72.5(11) / 68.7(13.3)Yorugloku 1999TurkeyMetoprolol (0.02 mg.kg^-1^)15/15NA46 (6) / 41 (6)5 min after extubationI or IIIntramuscular atropine and pethidine77(9) / 70(8)Amar 1991USALabetalol (infusion at 0.15 mg.kg^-1^ intravenous. followed by 0.25‒0.3 mg.kg^-1^ every 3 min as needed)8/8100/10043.9 (6.7) / 35.9 (10.3)NAIIntravenous midazolam (0.5 mg)70.0 (15.3) / 70.6 (10.2)Zhang 2017ChinaEsmolol (continuous perfusion at a dose of 50 μg.kg^-1^.min^-1^ during operation and infusion at a dose of 0.3 mg.kg^-1^ 3 min before tracheal intubation)30/3040/43.369.3 (5.4) / 66.1 (12.5)30 min after extubationI or IINA60.7(6.7) / 60.3(7.2)Kurian 2008United KingdomEsmolol (infusion of esmolol at 0-300 μg.kg^-1^.min^-1^)31/3719.3/10.860.2 (6.7) / 61.1 (7.5)180 min after extubationNALorazepam (2‒3 mg)82.5 (13.8) / 86.0 (14.1)Nam 1996South KoreaEsmolol (infusion at 1.5 mg.kg^-1^ 2 min before tracheal extubation)20/20NA31.2 (9.6) / 33.2 (7.5)5 min after extubationIGlycopyrrolate (0.2 mg) and intramuscular triflupromazine HCL (15 mg)69.1(9.4) / 64.8(8.5)Zeng 2007ChinaEsmolol (bolus at 0.5 mg.kg^-1^ for 5 min. followed by an infusion at 50 μg.kg^-1^.min^-1^ until the end of surgery)20/2075/65NA5 min after extubationI or IINA58(13)/57(10)Lee 2010South KoreaEsmolol (bolus at 1.0 mg.kg^-1^ followed by an infusion of 10 μg.kg^-1^.min^-1^)30/3060/53.361.7 (6.3) / 58.6 (6.6)PO + 24 hI or IIGlycopyrrolate (0.2 mg)161.8 (6.6) / 160.4 (6.3)StudyType of general anesthesiaHeightc, cm (I/C)SBPc, mmHg (I/C)DBPc, mmHg (I/C)MAPc, mmHg (I/C)MHRc, beats/min (I/C)Duration of surgeryc, min (I/C)Duration of anesthesiac, min (I/C)Queiroz 2024Balanced anesthesia or total intravenous anesthesiaNANANA94.2/94.382.4/79.2NANAMendonça 2023Balanced anesthesia165 (10) / 167 (10)110.4 (15.1) / 108.0 (13.4)NANA77.8 (10.1) / 74.3 (10.2)NANAAlkaya 2014Balanced anesthesiaNA137/13785/85105/10580/85213.5 (78.2) / 220.9 (101.8)203.7 (78.5) / 211.1 (102.4)Arar 2007Balanced anesthesiaNA142.6 (15.5) / 140.7 (19.5)76.4 (11.3) / 74.0 (10.7)98.0 (10.2) / 96.6 (10.9)98.8 (10.5) / 96.7 (13.0)288 (43.6) / 298.2 (45.6)314.1 (47.2) / 329.6 (50.9)Hosseinzadeh 2013Balanced anesthesiaNA17.6 (109.7) / 14.9 (115.6)13.5 (69.7) / 13.1 (72.0)NANA184.6 (42.7) / 186.6 (62.6)NAChia 2004Balanced anesthesia153.6 (5.4) / 155.6 (4.4)NANA87.6 (6.1) / 84.8 (6.1)74.2 (7.8) / 71.6 (9.2)122 (54) / 138 (50)NAGrillo 2003Balanced anesthesia165 (6) / 168 (6)NANA95 (12) / 88 (15)76 (9) / 77 (7)NANAO'Dwyer 1993Balanced anesthesiaNA141 (10) / 135 (6.2)77.8 (4.1) / 79.8 (3)74.3 (5.2) / 89 (7.1)70 (2) / 69 (3.7)NANAElokda. 2015Balanced anesthesia165 (10) /166 (8)130/13173.0/71.562.1/30.081.2 / 81.260 (5) / 61.6 (8)65.8 (7) / 63 (8)Kshama 2022Balanced anesthesia158.55 (7.3) / 157.7 (6.6)136.7 (14.7) / 130 (16.2)86.0 (10.1) / 82.5 (12.9)103.7 (12.2) / 98.8 (13.2)96.3 (14) / 90.4 (10.1)NANAVandenberg 1997Balanced anesthesiaNANANANANA34/24NASong 2021Balanced anesthesia168.4 (7.4) / 170.0 (8.9)NANA104.9 (12.1) / 105.8 (11.3)52.7 (21.4) / 57.3 (24.2)216.3 (35.0) / 212.8 (26.1)NAShetabi 2023Balanced anesthesiaNA121.2 (9.6) / 122 (8.8)74.1 (6.2) / 77 (9.6)104.9 (4.0) / 106.2 (8.6)80.8 (9.2) / 85.6 (6.4)NANADash 2023Balanced anesthesia164.8 (9.9) / 163.8 (9.4)119.9 (8.0) / 122.5 (11.0)77.7 (6.0) / 75.7 (8.5)91.7 (4.7) / 91.3 (6.4)71.8 (4.5) / 75.2 (7.7)NANALim 2000Balanced anesthesiaNA131.5 (18.4) / 129 (15)NANA71.4 (7.4) / 70.8 (11.9)NANAMaharjan 2005Balanced anesthesiaNANANA102.5 (10.5) / 106.6 (12.7)89.4 (23.4) / 95.6 (12.3)72.7 (32.8) / 80.5 (19.2)81.4 (30.3) / 91.4 (22.2)Morais 2020Balanced anesthesia161.9 (8.0) / 164.4 (9.7)NANANANA104.3 (14.3) / 112.8 (12.5)NARadwan 2016Balanced anesthesia170 (8) / 164 (6)NANANANA247 (74) / 243 (69)NASohn 1995Balanced anesthesia58.5 (8.3) / 58.6 (6.9)125.2(15.76) / 130.25(19.2)NANA77.5 (9.1) / 82.7 (13.9)175.5 (84.9) / 182.8 (73.1)NAFelding 1994Balanced anesthesiaNANANA91 (17) / 93 (15)NANANAVelayutham 2020Balanced anesthesiaNANANA92 (6) / 94 (5)83 (9) / 81 (8)NANAUnal 2008Balanced anesthesia165.8 (9.3) / 168.3 (8.2)NANA124.2 (20.1) / 117.4 (9.4)82.5 (9.9) / 89.4 (10.0)134.1 (74.5) / 121.2 (62.8)156.9 (74.4) / 145.5 (69.4)Ersin 2005Balanced anesthesiaNA132.1 (9.2) / 133.1 (10.4)78.3 (7.6) / 79 (6.1)NA87.2 (7.2) / 86.8 (8.2)119.4 (5.7) / 117.4 (7.8)137.7 (6.1) / 136.2 (8.1)Yorugloku 1999Balanced anesthesiaNA126.96 (12.38) / 122.83 (12.38)75.3 (10) / 85 (12.1)89.7 (8.1) / 91.1 (8.4)92.2 (7.4) / 88.7 (10.5)88 (12) / 92 (6)NALee 2010Total intravenous anesthesia161.8 (6.6) / 160.4 (6.3)NANA89.8 (13.3) / 90.2 (12.2)71.6 (9.5) / 72.3 (11.2)42.5 (4.8) / 41.3 (7.2)57.5 (2.8) / 56.3 (5.2)Amar 1991Balanced anesthesiaNA130.23/124.2070.5/68.993.9 / 91.682.4 / 81.3120.0 (29.7) / 125.6 (50.0)160.6 (34.0) / 159.4 (51.8)Zhang 2017Total intravenous anesthesiaNANANA92.7 (7.7) / 95.9 (6.4)76.8 (6.5) / 73.7 (8.2)180.5 (16.5) / 180.3 (18.2)NAKurian 2008Balanced or Total Intravenous anesthesia170.7 (8.0) / 173.1 (7.8)119.56 (4.15) / 122.57 (3.53)NANA86.1 (2.2) / 95.3 (2.2)NANANam 1996Balanced anesthesiaNA121 (7.1) / 118 (6.2)77 (5.3) / 78 (4.3)NA79 (7.3) / 80 (5.9)45 (15.6) / 38 (20.4)NAZeng 2007Total intravenous anesthesia159 (8) / 160 (9)112.9 (9) / 117.8 (9.6)77.5 (7.1) / 78.4 (8)NA85 (6.6) / 88.8 (10.3)88 (3) / 74 (28)102 (31) / 92 (3)Kawaguchi 2010Balanced anesthesia159 (7)/ 162 (7)148 (19) / 150 (19)85 (11) / 85 (10)63.6 (6.3) / 64.1 (9.1)72 (11) / 70 (14)228 (82) / 251 (108)309 (83) / 331 (126)aMean (standard deviation).bMean (range); n, Number; y, Years; kg, Kilogram; mg, Miligram; n, Nanogram; μ, Microgram; mL, Militer; min: minutes; h, Hours; s, Seconds; ASA, American Society of Anesthesiologists classification; I/C, Intervention group/Control group; PO, Post-Operatory; NA, Not Available.cMean (standard deviation); cm, Centimeter; mmHg, Millimeter of mercury; min, Minutes; I/C, Intervention group/Control group; NA, Not Available; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; MAP, Mean Arterial Pressure; HR, Heart Rate.
Pooled analysis
Primary outcomes
Beta-blockers significantly reduced the incidence of cough (RR = 0.55; 95% CI 0.36 to 0.83; p < 0.01; I^2^ = 73%; Fig. 2). Also, beta-blockers significantly altered the distribution of cough severity during tracheal extubation, shifting the severity distribution from moderate/severe to none/mild. Specifically, they significantly reduced the incidence of moderate/severe cough (RR = 0.21; 95% CI 0.13 to 0.34; p < 0.01; I^2^ = 0%; Fig. 3), while simultaneously increasing the incidence of patients experiencing no/mild cough (RR = 1.34; 95% CI 1.05 to 1.70; p = 0.017; I^2^ = 86%; Fig. 4).Figure 2. Beta-blockers significantly reduced the incidence of cough in patients undergoing tracheal extubation compared with placebo. MH, Mantel-Haenszel; CI, Confidence Interval.Figure 2. Figure 3Beta-blockers significantly reduced the incidence of moderate/severe cough in patients undergoing tracheal extubation compared with placebo. MH, Mantel-Haenszel; CI, Confidence Interval.Figure 3. Figure 4Beta-blockers significantly increased the incidence of no/mild cough in patients undergoing tracheal extubation. MH, Mantel-Haenszel; CI, Confidence Interval.Figure 4
Secondary outcomes
There was no difference between groups in bronchospasm (RR = 0.58; 95% CI 0.17 to 1.94; p = 0.375; I^2^ = 0%; Fig. 5), bucking (RR = 0.47; 95% CI 0.20 to 1.13; p = 0.093; I^2^ = 72%; Fig. 6), hypotension (RR = 1.43; 95% CI 0.87 to 2.38; p = 0.161; I^2^ = 0%; Supplementary Fig. 1) and bradycardia (RR = 1.24; 95% CI 0.31 to 4.97; p = 0.759; I^2^ = 0%; Supplementary Fig. 2).Figure 5. There was no difference between groups in the incidence of bronchospasm in patients undergoing tracheal extubation. MH, Mantel-Haenszel; CI, Confidence Interval.Figure 5. Figure 6There was no difference between groups in the incidence of bucking in patients undergoing tracheal extubation. MH, Mantel-Haenszel; CI, Confidence Interval.Figure 6
The risk of hypertension (RR = 0.28; 95% CI 0.13 to 0.58; p < 0.001; I^2^ = 45%; Supplementary Fig. 3), tachycardia (RR = 0.20; 95% CI 0.08 to 0.51; p < 0.001; I^2^ = 71%; Supplementary Fig. 4), and nausea or vomiting (RR = 0.60; 95% CI 0.50 to 0.72; p < 0.001; I^2^ = 2%; Supplementary Fig. 5) was significantly reduced in the beta-blocker group compared with the placebo group in patients undergoing tracheal extubation.
Hemodynamic variables
SBP, DBP, MAP, and MHR were significantly lower in the beta-blockers group compared with the placebo group at tracheal extubation after 1, 2, 5, 10, and 15 or more minutes (Supplementary Table 2). However, there was no significant difference between groups for MAP and MHR at tracheal extubation after 15 minutes or more.
Sensitivity analyses
We conducted leave-one-out sensitivity analyses for the outcomes of bucking, hypertension, cough, no/mild cough, moderate/severe cough, and tachycardia due to high heterogeneity. The leave-one-out analysis of the outcome of bucking showed that omitting Mendonça (2023)12 led to a significantly lower incidence of bucking in the beta-blockers group compared with the placebo group, with no heterogeneity observed (I^2^ = 0%; Supplementary Fig. 6). For the outcome of hypertension, cough, and no/mild cough, no study was identified as driving the heterogeneity, all omissions remained with high heterogeneity, favoring beta-blockers (Supplementary Fig. 7; Supplementary Fig. 8; Supplementary Fig. 9). The leave-one-out sensitivity analysis for the outcome of tachycardia showed similar results in all scenarios with a lower heterogeneity when Shetabi (2023)35 is omitted (I^2^ = 18%; Supplementary Fig. 10).
Additionally, we performed a meta-regression analysis for the following outcomes: SBP, DBP, MAP, and MHR using the mean age and the mean values at baseline of SBP, DBP, MAP, and MHR as predictors. Results are presented in Supplementary Table 4. Our results showed that age was a significant predictor (QMp < 0.05) for MHR at tracheal extubation, with higher baseline age values resulting in more positive mean differences, favoring placebo over beta-blockers. SBP, DBP, MAP, and MHR were not significant predictors of any outcome. Significant heterogeneity remained after accounting for the moderator effects of the selected predictors.
Quality assessment
The individual RCT appraisal is reported in Supplementary Table 5. Sixteen studies [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22,25,32,34,39,41,50] were considered at moderate risk of bias. Twelve studies presented moderate bias in bias from randomization process, nine in bias due to deviations from intended interventions, three in bias in measurement of the outcomes and twenty-two in the selection of the reported result. Nine RCTs were considered at high risk of bias and the others were classified as low risk of bias.
Publication bias was investigated for the outcomes of SBP, DBP, MAP, and MHR for every subgroup that had at least 10 studies (Supplementary Fig. 11). The visual inspection of the funnel plots with enhanced contour showed no visible signs of the “small study effect” with symmetrical funnel plots for most of the subgroups. This finding is corroborated by the results of the Egger’s Test (Supplementary Table 6).
Discussion
In this systematic review and meta-analysis of 31 RCTs, including 1,803 patients, we compared the use of beta-blockers with placebo in preventing complications in patients undergoing tracheal extubation. The main findings from the pooled analysis were: (1) The use of beta-blockers was associated with a reduced risk and intensity of cough; (2) The risk of hypertension, tachycardia and nausea or vomiting was significantly reduced in the beta-blocker group compared with the placebo group.
About 70% of patients undergoing procedures requiring general anesthesia and tracheal intubation may experience coughing.51 Coughing during tracheal extubation can lead to significant complications for patients, such as hypertension, tachycardia, myocardial ischemia, surgical bleeding, laryngospasm, bronchospasm, and increased intracranial and intraocular pressure.5 There is evidence that beta-blocker reduce the incidence of coughing in these patients by blocking ion channels, particularly voltage-dependent sodium channels and L-type calcium channels, in unmyelinated C fibers of vagal afferent nerves that innervate the upper airway and proximal bronchioles, thereby reducing excitability during procedures such as orotracheal intubation and extubation.52, 53, 54, 55
This meta-analysis showed that approximately 11% of patients receiving beta-blocker experienced significant coughing (moderate/severe intensity) during the peri-extubation period, compared to an incidence of 36% among those who received placebo. These findings are consistent with individual data from RCTs that investigated the incidence of this outcome in the population in question.12^,^18^,^33 Thus, it is evident that beta-blockers may be a promising alternative to prevent cough and reduce complications during tracheal extubation.
Moreover, the effectiveness of beta-blockers in reducing bucking can be attributed to their ability to block the effects of the sympathetic nervous system, specifically by antagonizing beta-adrenergic receptors.56 This inhibition leads to a decrease in heart rate, blood pressure, and overall sympathetic output, which can calm reflexive responses, such as coughing or bucking, particularly during anesthesia or intubation.57 By reducing the surge of adrenaline, beta-blockers helps stabilize cardiovascular and respiratory functions, minimizing involuntary movements that could disrupt medical procedures.58 Queiroz (2024)33 and Mendonça (2023)12 showed significantly lower risk in the beta-blocker group, and Dash (2023)17 indicated lower risk but with no statistical difference, suggesting that the intervention may be effective in reducing bucking. However, the limited number of patients led to Queiroz's (2024)33 results dominating the analysis. Thus, more RCTs evaluating bucking are needed to reach a more robust conclusion.
Furthermore, cardioselective beta-blockers, such as metoprolol, block the β1-adrenoceptor, leaving the β2-adrenoceptor free in the adrenergic response during extubation, which may help to prevent bronchospasm in this group of patients.59 Our data indicated a slight trend toward a reduction in the incidence of bronchospasm in the beta-blocker group, with a 48% lower relative risk of this complication in patients who received beta-blocker compared to those who received placebo. However, neither the individual studies12^,^17^,^30^,^33 nor the pooled analysis results were statistically significant. Therefore, it is crucial to re-emphasize the need for more RCTs evaluating the impact of these medications on the incidence and severity of bronchospasm.
Additionally, the manipulation of the larynx and pharynx during the transition from “asleep” to “awake” at tracheal extubation triggers exaggerated neural responses, leading to hemodynamic instability (hypertension and tachycardia) in 10%‒50% of cases.60^,^61 In this meta-analysis, beta-blockers reduced the incidence of tachycardia and hypertension by 80% and 72%, respectively compared with placebo. This effect may be expected due to the inhibitory action of beta-blockers on adrenergic receptors, which counteracts the effects of sympathetic activation during acute stress, mitigating cardiovascular alterations and nocive events in tracheal extubation.11^,^12
Patients undergoing tracheal extubation experience a 10%‒30% increase in blood pressure and MHR lasting approximately 5‒15 minutes, which can precipitate various cardiovascular events such as myocardial infarction, arrhythmias, cerebral edema, hemorrhage, and other complications.17^,^61 Therefore, the use of beta-blockers emerges as a potential intervention to stabilize these hemodynamic parameters, given their ability to mitigate exaggerated sympathetic responses.11^,^12 This meta-analysis revealed a statistically significant reduction in SBP, DBP, MHR, and MAP with the use of beta-blocker compared to placebo, with the most pronounced mean differences observed within the first 5 minutes post-extubation. Recent RCTs have also demonstrated significant reductions in these hemodynamic outcomes in the intervention group compared to placebo, further supporting the findings of this analysis.12^,^62 Future studies should focus on optimizing beta-blocker dosing protocols to maximize efficacy while minimizing adverse effects, particularly in patients with preexisting cardiovascular conditions.
The mechanism underlying nausea or vomiting potentially involves the blockade of adrenergic receptors, which can disrupt the cascade of events leading to these adverse events. In some cases, the use of short-acting beta-blockers, such as esmolol, has been shown to effectively manage the hemodynamic fluctuations that can occur during extubation, thereby potentially reducing the incidence of nausea or vomiting.56 Our results revealed a 40% reduction in the incidence of nausea and vomiting in patients undergoing tracheal extubation who received beta-blocker compared to those given a placebo. These findings are consistent with previous research, which suggests that beta-blockers can positively impact in incidence of nausea or vomiting.57
Our study has some important limitations. Despite our findings showing that beta-blockers effectively reduce hemodynamic complications during extubation, previous studies have reported conflicting results. These discrepancies can be attributed to variations in study design, such as differences in drug dosage, timing of administration (pre-anesthesia vs. intraoperative), and the type of beta-blockers used (e.g., cardioselective vs. non-cardioselective). Additionally, the type of surgery and patient characteristics, such as comorbidities, may affect responses to beta-blockers, with more complex surgeries or patients with cardiovascular issues showing different results. The diversity in anesthetic protocols, particularly the use of pre-anesthetic medications, may also influence outcomes, either masking or enhancing the effects of beta-blockers. Furthermore, discrepancies in outcome measurement, particularly the distinction between “cough” and “bucking” could lead to inconsistent findings. Furthermore, it is important to emphasize that post-extubation cough may also be a consequence of airway manipulation during intubation, which, therefore, represents a limitation in establishing a definitive causal relationship between the observed events. Finally, the primary outcomes were under reported with a greater focus on secondary outcomes. Additionally, the use of univariate meta-regression may have limited the assessment of heterogeneity, as it does not account for potential interactions between covariates. Unfortunately, this limitation exceeds the capacity of the present study to resolve or accurately address. To resolve these inconsistencies, future studies should standardize beta-blocker protocols, patient inclusion criteria, and outcome definitions to provide clearer insights into their hemodynamic benefits during extubation.
Conclusion
This meta-analysis compared beta-blockers with placebo in 1,803 patients who underwent tracheal extubation. Beta-blockers were associated with lower cough intensity, nausea or vomiting, hypertension, and tachycardia compared with placebo, without significant side effects. These results suggest the potential protective use of these drugs during the peri-extubation period. In this context, their use may be considered to prevent cardiorespiratory responses upon emergence from anesthesia.
This meta-analysis supports the use of beta-blockers to mitigate peri-extubation hemodynamic and airway complications. Further research should focus on defining optimal dosing regimens and identifying patient subgroups who would benefit most from this intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hu S.Li Y.Wang S.Xu S.Ju X.Ma L.Effects of intravenous infusion of lidocaine and dexmedetomidine on inhibiting cough during the tracheal extubation period after thyroid surgery BMC Anesthesiol 192019663105456810.1186/s 12871-019-0739-1PMC 6500031 · doi ↗ · pubmed ↗
- 2Yang S.S.Wang N.N.Postonogova T.Intravenous lidocaine to prevent postoperative airway complications in adults: a systematic review and meta-analysis Br J Anaesth 12420203143233200097810.1016/j.bja.2019.11.033 · doi ↗ · pubmed ↗
- 3Asai T.Koga K.Vaughan RS.Respiratory complications associated with tracheal intubation and extubation Br J Anaesth 801998767775977130610.1093/bja/80.6.767 · doi ↗ · pubmed ↗
- 4Frutos-Vivar F.Esteban A.Apezteguia C.Outcome of reintubated patients after scheduled extubation J Crit Care 2620115025092137652310.1016/j.jcrc.2010.12.015 · doi ↗ · pubmed ↗
- 5Gonzalez R.M.Bjerke R.J.Drobycki T.Prevention of endotracheal tube-induced coughing during emergence from general anesthesia Anesth Analg 7941994792795794379410.1213/00000539-199410000-00030 · doi ↗ · pubmed ↗
- 6Lowrie A.Johnston P.L.Fell D.Robinson SL.Cardiovascular and plasma catecholamine responses at tracheal extubation Br J Anaesth 681992261263154704810.1093/bja/68.3.261 · doi ↗ · pubmed ↗
- 7Coriat P.Mundler O.Bousseau D.Response of left ventricular ejection fraction to recovery from general anesthesia: Measurement by gated radionuclide angiography Anesth Analg 6519865936003085550 · pubmed ↗
- 8Bosco F.Braz J.Beta-blockers in anesthesiology: clinical and pharmacological aspects Rev Bras Anestesiol 512001431447