A Case of Spontaneous Regression of Primary Tumor after Adrenalectomy for Primary Lung Cancer with Synchronous Adrenal Metastasis
Hisaya Chikaraishi, Ryu Kanzaki, Hironobu Samejima, Masao Kobayashi, Julian Horiguchi, Tomohiro Maniwa, Hidetoshi Satomi, Keiichiro Honma, Jiro Okami

TL;DR
A patient with lung cancer and adrenal metastasis showed spontaneous regression of the primary tumor after surgery for the adrenal lesion.
Contribution
This case report documents a rare instance of spontaneous regression of non-small cell lung cancer following adrenalectomy.
Findings
The primary lung tumor was pathologically absent after surgical removal of the adrenal metastasis.
Postoperative imaging showed a reduction in the size of the primary tumor.
The patient remained recurrence-free for 5 months after surgery.
Abstract
Adrenal metastasis from primary lung cancer is relatively common, occurring in approximately 5%–10% of clinical cases. Long-term survival can be achieved through surgical resection of adrenal metastases in addition to primary lesions. Spontaneous regression of cancer is defined as the partial shrinkage or complete disappearance of cancer following no treatment or treatment considered ineffective against cancer. Spontaneous regression of non-small cell lung cancer (NSCLC) is rare. Here, we describe a case of NSCLC with adrenal metastasis, in which the primary tumor exhibited spontaneous regression and was pathologically absent following surgical treatment of the metastatic lesion. A 59-year-old male patient was referred to our department with elevated carcinoembryonic antigen levels and an abnormal opacity on chest CT. Contrast-enhanced CT revealed a 2-cm lesion in the right upper lobe…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
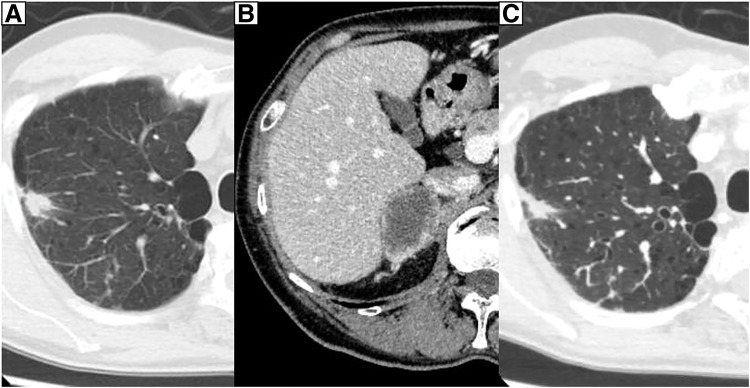 Fig. 1
Fig. 1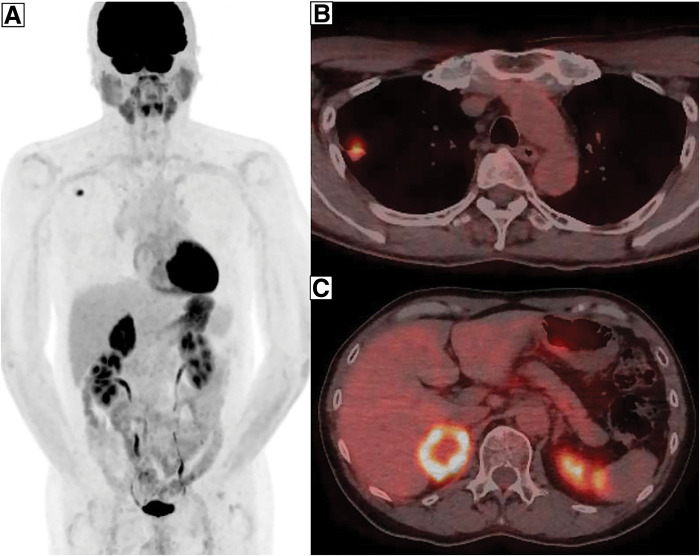 Fig. 2
Fig. 2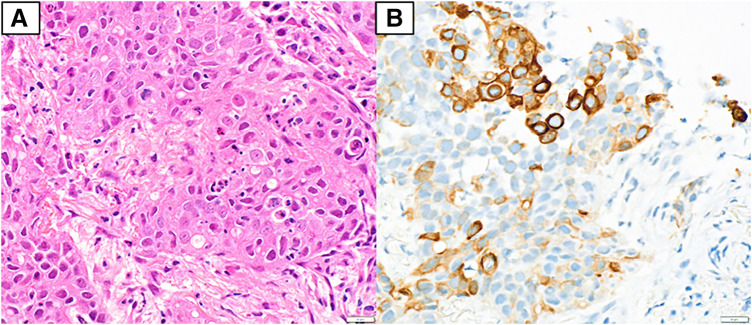 Fig. 3
Fig. 3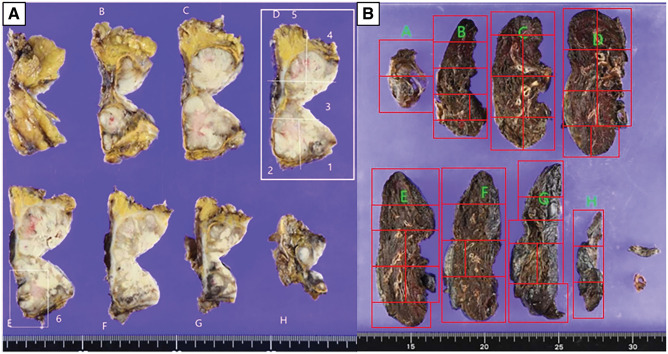 Fig. 4
Fig. 4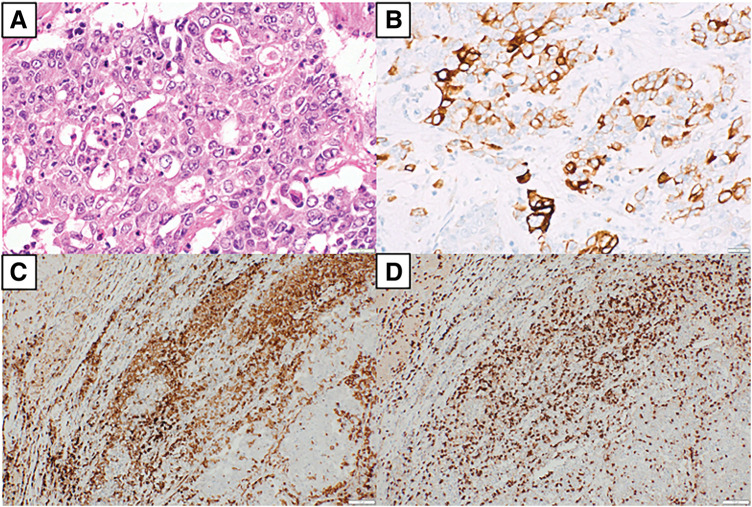 Fig. 5
Fig. 5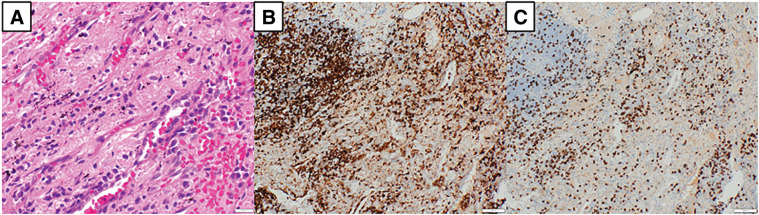 Fig. 6
Fig. 6| Author | Year | Age/gender | Histology | c-Stage | p-Stage | Cause of spontaneous regression | |
|---|---|---|---|---|---|---|---|
| 1 | Mizuno et al. | 2011 | 62/Male | NSCLC | cT1aN0M0 | pT0N0M0 | Biopsy |
| 2 | Furukawa et al. | 2011 | 56/Male | SCC | N/A | pT1N0M0 | Uncertain |
| 3 | Tomizawa et al. | 2015 | 85/Female | LCNEC | cT1cN0M0 | pT4N0M0 | Uncertain |
| 4 | Matsui et al. | 2018 | 56/Female | SCC | cT1bN2M0 | pT1aN2M0 | Biopsy |
| 5 | Uchida et al. | 2019 | 20/Female | N/A | cT1bN0M0 | pT1bN0M0 | Uncertain |
| 6 | Yamamoto et al. | 2022 | 69/Male | SCC | N/A | pT0N0M0 | Biopsy |
| 7 | Schiavon et al. | 2022 | 74/Male | Adeno | cT2aN0M0 | pT0N0M0 | Aspiration pneumonia or biopsy |
| 8 | Koike et al. | 2024 | 76/Male | SCC | cT1bN0M0 | pT1bN0M0 | Uncertain |
| 9 | Present case | 2025 | 59/Male | NSCLC | cT1bN0M1b | pT0N0M0 | Biopsy or surgery for metastases |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Research and Treatments · Cancer, Hypoxia, and Metabolism · Adrenal and Paraganglionic Tumors
Abbreviations
ALK anaplastic lymphoma kinase BRAF B-rapidly accelerated fibrosarcoma factor CD4 cluster of differentiation 4 CD8 cluster of differentiation 8 CEA carcinoembryonic antigen CK19 cytokeratin 19 CK7 cytokeratin 7 EGFR epidermal growth factor receptor FDG ^18^F-fluorodeoxyglucose HER2 human epidermal growth factor receptor 2 MET mesenchymal–epithelial transition NSCLC non-small cell lung cancer PD-L1 programmed cell death ligand 1 RET rearranged during transfection ROS1 c-ros oncogene 1, receptor tyrosine kinase SF-1 steroidogenic factor 1 SUVmax maximal value of standardized uptake value TPS tumor proportion score
INTRODUCTION
Adrenal metastases are recognized manifestations of advanced lung cancer and may occasionally present as a solitary lesion.^1)^ In carefully selected patients with a limited metastatic burden—referred to as oligometastatic disease—aggressive local treatment, including surgical resection, may be considered.^2–6)^ Spontaneous regression of malignancy, defined as partial or complete tumor reduction in the absence of effective therapy, is rare, particularly in NSCLC.^7,8)^ Although isolated reports have been documented, cases with pathological confirmation of complete tumor disappearance are exceedingly uncommon. This report describes a rare case of NSCLC with synchronous adrenal metastases in which the primary tumor underwent spontaneous regression, ultimately culminating in pathological disappearance following adrenalectomy.
CASE PRESENTATION
On March X, a 59-year-old male patient was referred to the department due to elevated serum CEA levels identified during a routine medical checkup. The patient had no significant past medical history and no regular use of supplements or medications. Blood count and biochemical analyses revealed no abnormalities. Tumor marker testing showed elevated CEA (128.3 ng/mL) and CK19 fragment (5.3 ng/mL) levels. The levels of progastrin-releasing peptide, squamous cell carcinoma-associated antigen, and neuron-specific enolase were within normal limits. Chest radiography showed no obvious abnormalities. Contrast-enhanced CT of the thorax and abdomen identified a 2.0-cm irregular nodular lesion with spiculated margins located just beneath the pleura of the dorsal segment (S2) of the right upper lobe. The tumor measured 1.5 cm in perpendicular diameter on CT scan (Fig. 1A). No apparent lymphadenopathy was noted. Additionally, a 4.5-cm mass was detected in the right adrenal gland (Fig. 1B). FDG-PET/CT demonstrated increased uptake in the lung lesion, with an SUVmax of 7.2 (Fig. 2A and 2B). Hypermetabolic activity was also observed in the adrenal mass, with an SUVmax of 11.6 (Fig. 2A and 2C). MRI of the head showed no evidence of brain metastases. A bronchoscopic biopsy was performed, and a neoplastic lesion was suspected. However, the atypia of the clustered cells was relatively mild, and neither irregular keratinization nor well-defined glandular structures were observed. Therefore, immunohistochemical evaluation was required to establish a definitive diagnosis of adenocarcinoma. Careful differentiation from benign lesions, such as inflammatory pseudotumors or infectious diseases, was also necessary. Based on the cellular morphology and positive immunostaining for CK7—which is known to be positive in primary lung cancer but negative in primary adrenal tumors (Fig. 3A and 3B)—the lesion was diagnosed as non-small cell carcinoma. In addition, the negativity of SF-1 and Melan-A, which are often positive in primary adrenal tumors, also supported the conclusion that the adrenal lesion was a metastatic tumor. Immunohistochemical analysis revealed a PD-L1 TPS of 10%, with no clear histological features indicative of poor differentiation. These findings led to a diagnosis of NSCLC (cT1bN0M1b, cStage IVA). Given the presence of a solitary adrenal metastasis, the disease was considered oligometastatic. Therefore, surgical resection of the adrenal mass was prioritized for definitive diagnosis and biomarker evaluation, with resection of the primary tumor planned subsequently if no further metastases were identified during follow-up.
Contrast-enhanced CT of the thorax and abdomen. CT shows an irregular 2-cm-sized nodular shadow with spicules just below the dorsal segment (S2) pleura of the right upper lobe (A), and a 4.5-cm mass was observed in the right adrenal gland (B). On CT following adrenalectomy, the perpendicular diameter of the primary lesion had decreased to 1.0 cm (C).
FDG-PET scans. FDG-PET scans show abnormal uptake (A) in the lung nodule (B, SUVmax = 7.2) and in the adrenal mass (C, SUVmax = 11.6).FDG, 18F-fluorodeoxyglucose; SUVmax, maximal value of standardized uptake value
Bronchoscopic biopsy. The specimen from the bronchoscopic biopsy shows that the nodule of the right lung appears to be NSCLC (A, hematoxylin and eosin stain, ×400 original magnification), and the cells were positive for CK7 (B) (×400).CK7, cytokeratin 7; NSCLC, non-small cell lung cancer
On May X, 34 days after bronchoscopic biopsy, a laparoscopic right adrenalectomy was performed (Fig. 4A). The size of the resected specimen was generally consistent with the preoperative CT findings. Histopathological analysis confirmed adrenal metastasis originating from NSCLC, based on morphological similarity and consistent CK7 immunoreactivity between the adrenal specimen and the bronchoscopic biopsy of the lung lesion (Fig. 5A and 5B). Infiltration by inflammatory cells was noted, with immunohistochemistry demonstrating the presence of CD4- and CD8-positive lymphocytes (Fig. 5C and 5D). Biomarker testing using the Oncomine Dx Target Test Multi-CDx System (Thermo Fisher Scientific, Waltham, MA, USA) revealed no detectable mutations in BRAF, EGFR, or HER2. The test results for ALK, ROS1, RET, and MET were inconclusive. Immunohistochemical analysis revealed a PD-L1 TPS of 10%, as well as an absence of histological features suggestive of poor differentiation, both consistent with the findings in the primary tumor. The CEA level measured at 5 weeks after adrenalectomy showed a marked decrease to 10.0 ng/mL, although it remained mildly elevated. Additionally, on CT following adrenalectomy, the maximum diameter of the primary lesion remained unchanged; however, the perpendicular diameter showed a slight reduction to 1.0 cm (Fig. 1C). As no new metastases were identified following adrenal resection, surgical removal of the primary lung tumor was carried out as planned.
Photographs of surgical specimens. Adrenal gland (A) and the right upper lobe (B).
Histological findings. (A) Lesion of the adrenal mass appears to be adrenal metastasis of NSCLC (hematoxylin and eosin stain, ×400 original magnification), and the cells were positive for CK7 (B) (×400). It shows inflammatory cell infiltration, and the cells were positive for CD4 (C) and CD8 (D) (×100).CD4, cluster of differentiation 4; CD8, cluster of differentiation 8; CK7, cytokeratin 7; NSCLC, non-small cell lung cancer
Operative findings
On August X, 78 days after adrenalectomy, robot-assisted right upper lobectomy was performed. Upper mediastinal node dissection followed the upper lobe resection, and the procedure was completed successfully. The operation duration was 316 min, and blood loss was minimal.
Histopathological findings
Specimens were evenly sectioned, and all sections underwent sampling. To assess lesion localization as anticipated preoperatively (Fig. 4B), additional deep sectioning was performed near the lesion, including re-embedding to prepare sections from the specimen’s reverse side and further processing of remaining tissue as appropriate. The nodule suspected as the primary tumor corresponded to nodular atelectasis with calcification and anthracosis. No pathological evidence of malignancy was identified (Fig. 6A). Inflammatory cell infiltration was present in the same area; immunostaining revealed predominance of CD4-positive lymphocytes alongside CD8-positive lymphocytes (Fig. 6B and 6C). The extent of inflammatory cell infiltration was comparable to that observed in the adrenal metastatic lesion.
Histological findings. (A) Lesion of the lung shows no malignant cells but is infiltrated by inflammatory cells (hematoxylin and eosin stain, ×400 original magnification), and the cells were positive for CD4 (B) and CD8 (C) (×100).CD4, cluster of differentiation 4; CD8, cluster of differentiation 8
Postoperative clinical course
The final diagnosis was NSCLC, pT0N0M1b, pStage IVA. The postoperative course was uneventful, and the patient was discharged without complications. Regarding postoperative adjuvant therapy, given the insufficient evidence supporting adjuvant treatment for oligometastatic disease, the patient was thoroughly informed of the potential benefits and risks. Based on this discussion and the patient’s preference, adjuvant therapy was not administered. The CEA level has normalized, and no evidence of recurrence or metastasis has been observed. The patient remains alive and recurrence-free at 8 months following lung resection.
DISCUSSION
Adrenal metastasis from primary lung cancer is common, followed by lung, liver, bone, and brain, with a frequency of 5%–10% in clinical cases.^1)^ Chemotherapy is usually administered to patients with NSCLC and distant metastases. The European consensus defines synchronous oligometastatic NSCLC as up to 5 metastases in no more than 3 organs, with mandatory staging using FDG-PET/CT and brain MRI or CT, and eligibility for radical treatment with acceptable toxicity.^9)^ Several reports have suggested that when distant metastases are deemed oligometastatic, local treatment of both the primary tumor and metastatic sites, including adrenalectomy, can improve long-term outcomes.^2–4)^ In particular, it has been reported that resection of adrenal metastases on the same side as the primary tumor has a better prognosis than resection of adrenal metastases on the opposite side. This is because metastasis from the lung to the ipsilateral adrenal gland is not hematogenous but is localized by lymphatic flow in the retroperitoneal route.^5,6)^ These reports suggest that resection of both the primary lung tumor and the adrenal metastases may offer long-term recurrence-free survival. In the present case, the tumor was diagnosed as an adrenal metastasis of lung cancer based on the morphological features of the tumor cells and immunoreactivity for CK7, SF-1 and Melan-A. Accordingly, a favorable prognosis was anticipated in this patient.
According to Cole and Everson, spontaneous regression of cancer is a pathological condition in which cancer shrinks or disappears spontaneously without or with treatment that is not supposed to be effective against cancer.^7)^ Spontaneous regression of NSCLC is considered to be extremely rare.^8)^ Since 2011, there have been 8 reported cases of surgical treatment for primary NSCLC that showed spontaneous regression (Table 1).^10–17)^ Seven of these cases were reported in Japan, consistent with previous reports showing that spontaneous regression of primary NSCLC is relatively common in Japan.^18)^ Mizuno et al. reported the first case of complete pathological disappearance due to spontaneous regression,^10)^ and only 2 cases have since been reported.^15,16)^ This is the 4th reported case of pathologically proven complete disappearance of NSCLC due to spontaneous regression. None of the 3 previously reported cases involved distant metastasis, and this is the first case in which complete disappearance due to spontaneous regression of primary NSCLC with distant metastasis was pathologically proven.
To assess the therapeutic efficacy of adrenalectomy, we monitored the perioperative changes in serum CEA levels. The serum half-life of CEA is generally estimated to be approximately 3–7 days. In patients with preserved hepatic function, CEA levels are expected to decrease to near-normal levels within 4–6 weeks postoperatively, corresponding to approximately 5 half-lives.^19)^ In the present case, liver function was preserved, suggesting that any CEA changes attributable to adrenalectomy would be reliably reflected by 6 weeks postoperatively. However, in this case, CEA was measured approximately 5 weeks after adrenalectomy. Therefore, the elevated preoperative serum CEA level was considered to have been primarily attributable to the metastatic lesions in the adrenal gland.
Various hypotheses have been proposed regarding the mechanisms of spontaneous regression. Clinically, it is often triggered by surgery, invasive procedures, or infections, suggesting immune activation against tissue invasion.^20,21)^ Infiltration of CD8- and CD4-positive T cells into tumor tissue has been implicated in tumor shrinkage.^22–24)^ In our case, both cell types were observed in the primary lung tumor and adrenal metastases, suggesting that the immune response may have played a key role. To understand the involvement of the immune response in tumor regression, it is important to assess the degree of infiltration by CD4- and CD8-positive lymphocytes. In the present case, although quantitative or semi-quantitative evaluation was challenging due to the presence of necrotic tissue in the adrenal lesion and marked, heterogeneous fibrosis in the primary tumor, no substantial difference in the degree of lymphocyte infiltration was observed between the 2 lesions. It remains unclear whether these lymphocytes are tumor-specific, and further case studies are needed to elucidate this mechanism. Previous reports have suggested that spontaneous regression in NSCLC may be associated with high PD-L1 expression and poorly differentiated histological features.^25)^ However, in the present case, PD-L1 expression was 10% in both lesions, and there were no definitive histopathological findings indicative of poor differentiation. Further accumulation of cases is necessary to establish a clearer understanding of the relationship between PD-L1 expression, tumor differentiation, and spontaneous regression. In our case, adrenalectomy and bronchoscopic biopsy may activate the immune system. In previous reports, biopsy of the metastases caused spontaneous regression of the primary tumor,^26,27)^ and adrenalectomy may have caused the spontaneous regression in this case. However, the presence of inflammatory cell infiltration in the metastases suggests that the bronchoscopic biopsy performed prior to adrenalectomy may have caused spontaneous regression.
Of the primary and metastatic lesions, both of which showed inflammatory cell infiltration, only the primary lesion showed spontaneous regression, suggesting that, in addition to the mechanism proposed above, other factors may have contributed to the spontaneous regression in this case. The relationship between metastatic and primary tumors is bidirectional, and the presence of metastatic tumors causes primary tumors to grow and further disseminate.^28)^ Therefore, in our case, adrenalectomy performed during the ongoing spontaneous regression triggered by bronchoscopic biopsy may have further enhanced the regression by boosting the immune response and removing metastatic support from the primary tumor. Evidence supporting local therapy for oligometastatic disease remains limited, and the concomitant use of systemic chemotherapy should be carefully considered. Although chemotherapy was not administered in the present case, close follow-up is warranted.
Limitation
Reporting cases of spontaneous regression of cancer inherently involves certain limitations. One of the main concerns is the possibility of overdiagnosis at the initial evaluation, particularly in small lesions, as well as the potential for misdiagnosis of benign conditions such as inflammatory pseudotumors or infectious lesions. In the present case, the diagnosis of malignancy was confirmed by histopathological examination of a bronchoscopic biopsy specimen, with immunohistochemical findings supporting the diagnosis of non-small cell lung carcinoma. Furthermore, comprehensive clinical, radiological, and pathological evaluations were conducted to support the diagnosis of spontaneous regression. These efforts aimed to minimize the likelihood of misdiagnosis and ensure the validity of the observed spontaneous regression.
CONCLUSIONS
This report highlights a case of primary lung cancer with adrenal metastasis in which the primary tumor showed spontaneous regression and completely disappeared after surgical treatment of the metastasis.
ACKNOWLEDGMENTS
The authors thank Editage (https://www.editage.jp) for the English language review of the manuscript.
DECLARATIONS
Funding
Not applicable.
Authors’ contributions
H. Chikaraishi analyzed and interpreted the patient data and was a major contributor to writing the manuscript.
All the authors have read and approved the final version of the manuscript.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Written informed consent was obtained from the patient for publication of this report and its accompanying images.
Competing interests
The authors have no competing interests associated with this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sandler MA Pearlberg JL Madrazo BL Computed tomographic evaluation of the adrenal gland in the preoperative assessment of bronchogenic carcinoma. Radiology 1982; 145: 733–6.7146405 10.1148/radiology.145.3.7146405 · doi ↗ · pubmed ↗
- 2Kim SH Brennan MF Russo P The role of surgery in the treatment of clinically isolated adrenal metastasis. Cancer 1998; 82: 389–94.9445197 · pubmed ↗
- 3Porte H Siat J Guibert B Resection of adrenal metastases from non-small cell lung cancer: a multicenter study. Ann Thorac Surg 2001; 71: 981–5.11269485 10.1016/s 0003-4975(00)02509-1 · doi ↗ · pubmed ↗
- 4Iwanami T Uramoto T Baba T Guidelines for thoracic surgery: treatment recommendations for adrenal metastasis of non-small cell lung cancer. Jpn J Thorac Surg 2010; 63: 1101–8. (in Japanese)21174656 · pubmed ↗
- 5Raz DJ Lanuti M Gaissert HC Outcomes of patients with isolated adrenal metastasis from non-small cell lung carcinoma. Ann Thorac Surg 2011; 92: 1788–93; discussion 93.21944257 10.1016/j.athoracsur.2011.05.116 · doi ↗ · pubmed ↗
- 6Károlyi P. Do adrenal metastases from lung cancer develop by lymphogenous or hematogenous route? J Surg Oncol 1990; 43: 154–6.2314102 10.1002/jso.2930430306 · doi ↗ · pubmed ↗
- 7Cole WH Everson TC. Spontaneous regression of cancer: preliminary report. Ann Surg 1956; 144: 366–83.13363274 10.1097/00000658-195609000-00007 PMC 1465423 · doi ↗ · pubmed ↗
- 8Kumar T Patel N Talwar A. Spontaneous regression of thoracic malignancies. Respir Med 2010; 104: 1543–50.20580882 10.1016/j.rmed.2010.04.026 · doi ↗ · pubmed ↗