Partial prosthesis detachment early after open atrial transcatheter mitral valve replacement: could an artificial intelligence–based modified mitral valve model make the difference?
Aureliano Ruggio, Gabriella Locorotondo, Andrea Campea, Riccardo Marano, Eleonora Moliterno, Francesca Graziani, Cristina Aurigemma, Faustino Pennestrì, Antonella Lombardo, Francesco Burzotta

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
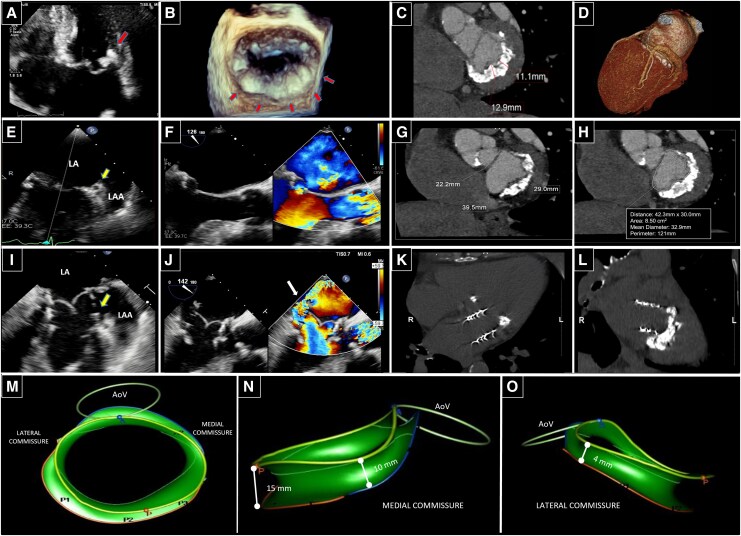 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac and Coronary Surgery Techniques
A 75-year-old woman with severe mitral annular calcification (MAC) and significant mitral regurgitation, considered unsuitable for either surgery or transcatheter mitral valve (MV) replacement (TMVR) (Figure 1A–H), underwent open-transatrial TMVR with a 29-mm Sapien-3 Ultra aortic transcatheter heart valve (THV) implantation in another institution. Five months later, partial prosthesis detachment at the lateral commissure and severe paravalvular leak (PVL) (Figure 1I–L; Supplementary data online, Video S1) resulted in cardiogenic shock.
In patients with MAC and severe MV dysfunction, representing a high-risk subset strongly needing improvement in management, TMVR using balloon-expandable aortic THVs, through percutaneous or hybrid approaches, has emerged as a feasible option. Potential life-threatening complications, such as PVL and THV detachment, that occurred in our patient, can be predicted by a multi-slice computed tomography (MSCT)–based MAC score, which describes the circumferential and radial extent of MAC.
To assess anatomical contributors to failure, a retrospective analysis of our MAC case by an artificial intelligence (AI)–based 3D-modified MV model (Figure 1M–O; Supplementary data online, Video S2) revealed anatomical details not evident on pre-operative MSCT scan: a nearly preserved saddle-shaped annulus (thus not ideally suited to a circular THV) and an asymmetric cranio-caudal calcium distribution along the mitral annular circumference (with a lower thickness at the lateral commissure, exactly where the PVL occurred). Both these 3D-derived parameters could represent potential imaging predictors of PVL and THV embolization.
Our case highlights a potential complementary role of an AI-enhanced 3D-modified MV model in the pre-operative screening of MAC patients by providing additional anatomical details as compared with CT-based MAC score alone, to personalize surgical planning.
Further studies are needed to confirm whether the integration of this model may improve patient selection, prediction of THV embolization risk, or even the futility of the procedure.
Supplementary Material
qyaf096_Supplementary_Data