Last-minute cancellation of elective lung cancer surgery is associated with poorer survival
Marco Nardini, Nilanjan Chaudhuri, Joshil Lodhia, Richard Milton, Peter Tcherveniakov, Elaine Teh, Alessandro Brunelli

TL;DR
Last-minute cancellations of lung cancer surgery are linked to worse long-term survival, especially when cancellations are due to patient-related issues.
Contribution
This study identifies a link between last-minute cancellations of lung cancer surgery and poorer survival, particularly for patient-related cancellations.
Findings
12% of lung cancer surgeries were cancelled last-minute, with 79% due to process-related and 21% to patient-related reasons.
Patient-related cancellations were strongly associated with poorer 5-year survival compared to non-cancelled surgeries.
Process-related cancellations had a less significant impact on survival than patient-related cancellations.
Abstract
Previous studies have highlighted the negative impact on patients’ and relatives’ psychological status following last-minute cancellations (LMCs) [1] and its relationship with poorer prognosis [1–5]. Our objective was to assess the incidence and reason of last-minute cancellations before surgery for lung cancer and their association with outcomes. Retrospective analysis on all consecutive patients booked for elective lung cancer surgery from January 2017 through December 2022 in a single centre. Last-minute cancellation: a cancellation occurring within the last 24 h from the planned operation. Cancellation categories: process-related and patient-related. The short-term and long-term outcomes of patients who experienced a last-minute cancellation were analysed. 197 patients of 1587 (12%) had a last-minute cancellation: 156 (79%) were process-related and 41 (21%) were patient-related.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
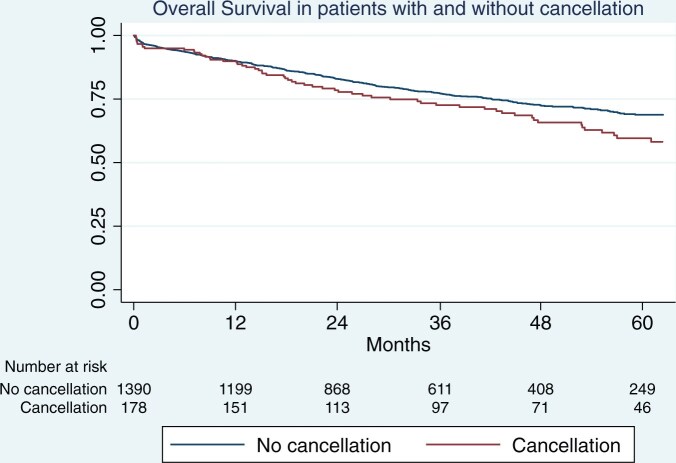 Figure 1
Figure 1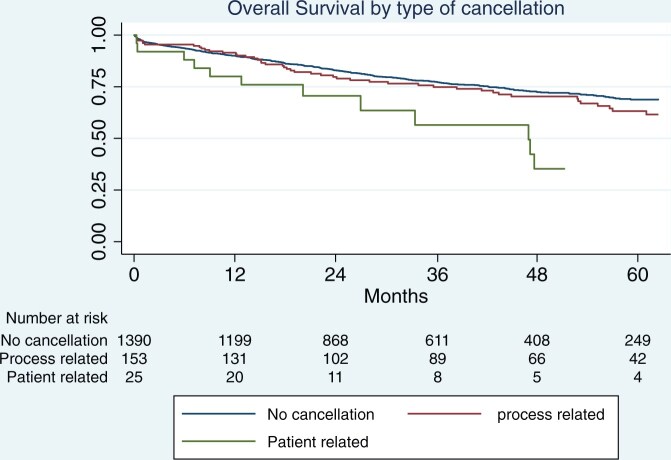 Figure 2
Figure 2| No cancellation (no. 1390) | Process-related (no. 156) | Patient-related (no. 41) | ANOVA | |
|---|---|---|---|---|
| Age | 69.0 (9.0) | 68.8 (10.9) | 69.2 (8.3) | 0.96 |
| Gender (male), | 643 (46%) | 66 (42%) | 21 (51%) | 0.51 |
| BMI (kg/m2) | 27.2 (5.3) | 26.7 (5.2) | 26.6 (5.0) | 0.50 |
| FEV1% | 90.3 (21.1) | 89.0 (22.1) | 84.0 (20.0) | 0.09 |
| DLCO% | 75.8 (18.8) | 73.7 (18.9) | 73.4 (16.5) | 0.31 |
| CCI > 1 (n,%) | 367 (26%) | 49 (31%) | 14 (34%) | 0.24 |
| ASA > 2 (n,%) | 318 (23%) | 63 (40%) | 22 (54%) | <0.001 |
| CAD (n,%) | 145 (10%) | 15 (9.6%) | 3 (7.3%) | 0.78 |
| Diabetes | 180 (13%) | 19 (12%) | 3 (7.3%) | 0.60 |
| PS > 1 | 125 (9.0%) | 18 (12%) | 4 (9.7%) | 0.58 |
| CVD | 53 (3.8%) | 4 (2.6%) | 3 (7.3%) | 0.33 |
| No. patients (%) | |
|---|---|
| Hospital-related cancellations | |
| ICU/HDU bed unavailable | 40 (26%) |
| Ward bed unavailable | 21 (14%) |
| Urgent case took priority | 16 (10.5%) |
| Theatre overran | 42 (27.5%) |
| Management change | 7 (4.5%) |
| Staff unavailable | 23 (15%) |
| Theatre ventilation failure | 3 (1.9%) |
| Admin error | 1 (0.6%) |
| Patient-related cancellations | |
| Deemed unfit for surgery | 26 (65%) |
| Patient’s decision | 8 (20%) |
| Additional tests required | 6 (15%) |
| Variables | HR |
| 95% CI |
|---|---|---|---|
| Age | 1.03 | <0.001 | 1.02–1.05 |
| Gender male | 1.51 | <0.001 | 1.23–1.86 |
| DLCO | 0.98 | <0.001 | 0.97–0.98 |
| Clinical T stage > 1 | 1.64 | <0.001 | 1.31–2.05 |
| Open approach | 1.83 | <0.001 | 1.42–2.37 |
| Process-related cancellation (ref. no cancellation) | 1.22 | 0.17 | 0.91–1.63 |
| Patient-related cancellation (ref no cancellation) | 1.87 | 0.043 | 1.02–3.42 |
| No cancellation (no. 1390) | Process-related (no. 156) | Patient-related (no. 41) |
| |
|---|---|---|---|---|
| Rescheduled surgery, | 151 (97%) | 25 (61%) | <0.001 | |
| Days till surgery, median (IQR) | 12 (5-21) | 16 (10-35) | 0.012 | |
| 30-day deaths | 48 (3.4%) | 5 (3.2%) | 2 (4.9%) | 0.87 |
| 1-year deaths | 138 (9.9%) | 13 (8.3%) | 5 (12%) | 0.70 |
| 3-year deaths | 276 (20%) | 35 (22%) | 9 (22%) | 0.66 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Lung Cancer Diagnosis and Treatment · Gastric Cancer Management and Outcomes
INTRODUCTION
Previous studies have highlighted the negative impact on patients’ and relatives’ psychological status following last-minute cancellations (LMCs) [1] and its relationship with poorer prognosis [1–5]. As practising surgeons, we have direct empirical experiences of the potentially devastating consequences of a LMC on our patients, who lose trust in the process, feel unsafe going home without having received treatment and experience the uncertainty of future rescheduling. In addition, cancellations have severe negative effect on the institution itself, with resources waste (i.e. operating room underutilization), increasing waiting list and additional costs (i.e. need for repeating out-of-date investigations) [4–6]. Finally, the cancellations of elective procedures have an impact on the training of the surgical residents: in the context of a public healthcare system where the increasing service provision demands, and the scrutiny of working hours have already reduced the number of procedures performed by the individual trainee by the end of her/his training [5], the patient’s cancellation is a missed training opportunity.
Despite these considerations and despite Wong et al. [3] describing a high rate of overall surgery cancellation in the British National Health System, as high as 13.9%, there are no recognized standard operating procedures to prevent a surgical cancellation and to investigate it when it happened.
Therefore, we set this study with the objective to analyse the prevalence of LMCs, specific to curative-intent surgery for lung cancer at our institution, to investigate the causes of the cancellations and finally to discover their association with patients’ prognosis. The main rationale was to generate new evidence to ultimately raise awareness in our specialty and generate additional studies to inform standard operative procedure to investigate and prevent surgical cancellations [6–10].
PATIENTS AND METHODS
Study design
This is a single centre, retrospective, observational cohort study. We retrospectively analysed consecutive patients booked for elective lung cancer curative-intent resections.
Ethical statement
The Institution Review Board of Leeds Teaching Hospitals reviewed this study and considered it as service evaluation not requiring formal review by the research ethics committee, and individual patient’s consent for this retrospective analysis was waived.
Patients
Patients’ data were gained by searching the bespoke database of the Department of Thoracic Surgery, St James’s University Hospital, Leeds, UK, from 1 January 2017 and until 31 December 2022. Patients booked for procedures other than lung cancer resections with curative intent were excluded. Within this group (patients who were admitted to the department to receive lung cancer curative-intent surgery), we identified patients who sustained a LMC; this was defined as a cancellation occurring within the last 24 h from the planned operation time as per Scheenstra et al. [2].
These patients were identified from the operating theatre list records, and the reason for cancellation was specified in the theatre list, and/or on the bespoke electronic system, and/or in the patient records.
The following variables were retrieved and analysed along with the presence and type of cancellation: gender, age, body mass index, forced expiratory volume in 1 s expressed in percentage of predicted for age and gender, carbon monoxide lung diffusion capacity %, history of coronary artery disease and cerebrovascular disease, Eastern Cooperative Oncology Group Performance score, American Society of Anesthesiology score, clinical staging, surgical access (open versus minimally invasive), extent of resection (wedge, segmentectomy, lobectomy, pneumonectomy). Most of the variables were complete. Carbon monoxide lung diffusion capacity was missing in 2 patients. The missing value was replaced with the mean of the non-missing values. For every cancellation, it was investigated whether the surgery was rescheduled or not; the incidence of rescheduling in each cancellation category was reported. For every rescheduled procedure, the delay between cancellation and rescheduling was evaluated in every cancellation category. Ninety-day mortality and the 5-year overall survival (OS) were investigated and relation with cancellation were reported. The follow-up started from the date of cancellation only for those patients who were not rescheduled.
Categories of cancellation
The recorded reasons for cancellation were analysed and were then grouped into 2 main categories: process-related (PR) and patient-related (PTR) cancellation. PR cancellation was attributed when the leading factor that led to the cancellation was related to a hospital process problem. PTR was attributed when the leading factor that triggered the cancellation was a medical reason or patient’s choice, i.e. patient’s new condition, change in treatment plan, etc.
Statistical analysis
A descriptive statistic was performed to report the prevalence of LMCs, and their reasons were reported. Numeric variables with normal distribution were compared between categories using the unpaired Student’s t-test, while those without normal distribution were compared using the Mann–Whitney U-test. Categorical variables were compared between groups using the Chi-squared test or the Fisher’s exact test (in case the number of observations was <10 in at least 1 cell). Follow-up information was obtained by data retrieved from the hospital electronic clinical information system. All patients were followed up through October 2023. No patient was lost at follow-up. OS was measured from the date of surgery to the date of death from any cause and censored at the date of data retrieval for survivors.
Survival end-points were characterized with the use of the Kaplan–Meier estimator. A log-rank test was used to estimate the P-value for testing differences between the category of cancellations, modified with Bonferroni correction.
Hazard ratios and their confidence intervals (CIs) were estimated with the use of Cox proportional hazards models with robust indicators. A stepwise backward elimination of variables was performed with P < 0.1 set as threshold for variable retention in the final regression model. Along with the presence and type of cancellation, the following variables were initially used as independent co-variates in the regression model based on their clinical relevance: age sex, body mass index, forced expiratory volume in 1 s, carbon monoxide lung diffusion capacity, clinical T stage, clinical N stage, presence of coronary artery disease, ASA score, Charlson’s comorbidity index, surgical access (open versus minimally invasive) extent of operation (wedge resection, segmentectomy, lobectomy, pneumonectomy), no surgical treatment. Patients who did not receive surgery after being cancelled were still included in the analysis, and a co-variate was created to indicate their definitive treatment (surgery versus no surgery) to adjust the analysis accordingly, as not having surgery may have influenced the outcome within those who had a cancellation.
The surgical delay predictor was tested for a possible association with survival using three-knots restricted cubic splines in a Cox proportional hazard model.
All tests were performed using the Stata 15.0 statistical software (Stata Corp, College Station, TX, USA).
RESULTS
Patients’ characteristics and reasons for cancellation
Between January 2017 and December 2022, 1587 patients were scheduled for thoracic surgery with the indication of pulmonary malignancy curative-intent surgery. One-hundred and ninety-seven patients of 1587 (12%) sustained a LMC; 156 (79.1%) were PR and 41(20.8%) were for PTR cancellations.
Twenty-one (11%) of the cancelled patients never received surgery; 3% (5/156) of PR cancelled patients did not receive surgery and 39% (16/41) of those cancelled for PTR reasons did not receive surgery, P < 0.0001.
Comparison of patients’ characteristics is summarized in Table 1. There were no significant baseline differences between the 3 groups (non-cancelled, PR and PTR). There were no significant differences in patients’ comorbidities, fitness test and performance status. The American Society of Anesthesiologists score was higher in the patients who were cancelled: ASA was higher than 2 in 318/1390 (23%) in the non-cancelled group, in 63/146 (40%) in PR and 22/41 (54%) in PTR group.
The detailed reasons for cancellation per group are shown in Table 2. The most frequent reason for cancellation in the PR group was theatre unavailability due to previous cases overrun in 42/156 patients (27.5%). The 2nd most important reason in this group was hospital beds unavailability in 40 cases (26%) followed by staff unavailability (surgeons, nurses or anaesthesiologists) in 23 cases (15%).
In the PRT group, we identified only 3 themes for cancellation: the patient was deemed unfit on the day by surgeon or by the anaesthesiologist in 26 cases/41 (65%), the patient changed mind regarding her/his own treatment in 8 cases (20%) and additional tests were requested in 6 cases (15%).
Patients’ outcomes
The 90-day mortality rate was similar between cancelled and non-cancelled patients: 9/197 (4.6%) vs 66/1390 (4.7%), P = 1. The 90-day mortality rate of those patients who were cancelled for PTR reasons was 4.9% (2/41) vs 4.5% (7/156) in those cancelled for PR reasons (P = 1).
Fifty of 197 (25%) cancelled patients were T upstaged from T1 to >T1 (vs 243/1390, 17% of non-cancelled patients) (P = 0.007). Fifty-eight of 197 (29%) cancelled patients were N upstaged from N0 to N1 or N2 (vs 277/1390, 20% of non-cancelled patients, P = 0.002).
The follow-up index in all 3 groups was 1 as we did not have any patient lost to follow-up. Median follow-up in patients without cancellation was 41 months (IQR 10–83). It was 48 months (IQR 9–82) and 38 months (IQR 14–81) in those with a PR and PTR cancellation, respectively. Five-year OS in patients without cancellation was 69% (95% CI 66–71) vs 58% (95% CI 49–66) among those who had a cancellation (Fig. 1). The difference in survival between these 2 groups was statistically significant (P = 0.022). In particular, the 5-year OS of those cancelled for organizational reason was 61% (95% CI 52–60) vs 35% (95% CI 14–58) in those cancelled for PTR reasons (adjusted P value for multiple comparisons = 0.14). On the other hand, there was no difference in survival between patients without cancellation (69%, 95% CI 66–71) and those with PR cancellation (63%, 95% CI 54–71) (adjusted P value for multiple comparisons = 0.33). The survival of patients with PTR cancellation was significantly poorer than those without cancellation (adjusted P value for multiple comparisons = 0.0072) (Fig. 2).
Overall survival in patients with and without cancellations.
Overall survival by type of surgical cancellation.
The median survival for those with process-based cancellation was 74 months versus 48 months in those with PTR cancellations.
Cox regression analysis showed that surgery cancellation within the last 24 h for PTR (hazard ratio 1.87, 95% CI 1.02–3.42, P = 0.043) reasons remained a factor associated with poorer OS after adjusting for clinical stage, type of operation, and PTR variables (Table 3).
Outcomes by treatment’s delays and cancellation status
The median delay from cancellation to surgery was 12 days (5–21 days range) for process-based cancellations and 16 days (10–35) for PTR reasons, P = 0.012 (Table 4). The median overall delay was 13 days.
The surgical delay from cancellation was not associated with poorer OS when tested in a Cox proportional hazard model using three-knots restricted cubic splines. Table 4 reports the outcomes according to cancellation status. We were not able to find any difference in 30-day, 1- or 3-year mortality between groups.
DISCUSSION
As previously published literature suggested that LMC is associated with poorer clinical outcome, the main objective of this study was to investigate if this applies to lung cancer surgery. Consequently, we aimed to identify modifiable risk factors (PTR or hospital-related) for cancellation that demands systems’ implementation.
Main findings
The OS difference was statistically significant between cancelled patient and non-cancelled patient, and it was also significant between hospital-related cancellation and PTR cancellation. There was no difference in age, gender, respiratory function tests or performance status in the 3 groups (no cancellation, PR and PTR cancellations). ASA score was higher in cancelled patients, but we could not identify other independent risk factors for cancellation, unlike other studies [2].
The PTR cancellation group is associated with poorest prognosis. The main reason for cancellation, in this group, was that patient was deemed unfit for general anaesthetics or surgery on the day (26 patients/41, 65%). Within the reason of being unfit, ongoing infection, anaemia, neutropenia and new symptoms being recurrent themes. The 2nd most relevant group within the PTR cancellation, that accounted to 20%, are patients who cancelled themselves. These 2 types of events may be mitigated by an additional review, closer to the date of surgery, and more extensive pre-habilitation and lung surgery pre-operative counselling, respectively [8, 11, 12].
There was statistically significant difference in the rescheduling rate of patients between the 2 groups of PR and PTR cancellations: operations that were cancelled for PR reasons were rescheduled in 96.7% of the cases and with a median of 12 days delay.
Operations that were cancelled for medical reasons were only rescheduled in 60.9% with a longer delay (Table 2) P < 0.0001. In the patients who were rescheduled, there was not statistically significance in the delay time between the 2 groups.
During 30 days of follow-up, 48 deaths (3.4%) occurred in the non-cancellation group, 5 (3.2%) occurred in the PR group and 2 (4.9%) deaths occurred in the PTR group and these were not statistically significant, P = 0.87. PR-related cancellations were mainly related to operating theatre availability (previous case overrun), staff shortages/bed availability and emergencies who took priority.
System implementations are required for better theatre list scheduling [13] as the previous case overrun was a recurrent theme and was potentially preventable. A proportion of complex cases that may require a longer procedure can be identified in advance, hence discussed at high-risk multidisciplinary meetings. Planning of anaesthetic intervention and dual specialist attendance may be cost-effective measures if they result in lower cancellation rate of the subsequent scheduled procedures and need to be further evaluated [14, 15].
The 2nd main theme in PR cancellation is bed availability. An expansion of inpatient beds is complex but maximizing the outpatient procedures and the day cases services would create more bed availability, while segregation of elective and urgent services would ring-fence both theatre access and bed availability for scheduled patients [16].
Limitations
Our study was an observational, retrospective patients’ cohort study and therefore the reason for cancellations was sometimes associated with limited recorded information. However, the main reason for cancellation could be identified in all cases. As currently there are no standard operative procedures in place to prevent or investigate a cancellation, the records on reason for cancellation were heterogeneous and subjective.
This study was also a single-centre cohort, executed in a large tertiary academic referring centre that performs a large volume of lung cancer surgeries per year. Therefore, this study may be a good representation of similar thoracic surgery unit within the country or within similar public health care system (National Health System) but may not represent the reality of substantially different health care systems.
It may be probable that the study was underpowered to detect clinically relevant differences between categories of cancellation. This is especially considering the small number of patients in the PTR group. This should be considered when interpreting the results.
Finally, the interval between clinic consultation and surgery was not recorded; this may significantly correlate to PTR cancellations, as a longer interval may allow more times for clinical changes to happen while awaiting surgery.
CONCLUSION
Unanticipated LMCs of elective lung cancer surgery are common and are associated with poorer oncologic outcomes. We believe that our results may contribute to raise awareness on this problem and on its impact on outcome. Our findings would assist in the implementation of patients’ workflow with a view to minimize surgery cancellation, mitigate their negative impact on cancer prognosis, and optimize hospital resources. Prospective studies will be required following implementation of clinical and structural processes.
FUNDINGS
No funding was available for this study.
Conflict of interest: Dr Alessandro Brunelli received consultancy fees for speaker honoraria and advisory Board roles with Astra Zeneca, BMS, Ethicon, MSD and Roche. No conflicts of interest disclosed by other authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ivarsson B , Larsson S, Sjoberg T. Postponed or cancelled heart operations from the patient’s perspective. J Nurs Manag 2004;12:28–36.15101453 10.1111/j.1365-2834.2004.00400.x · doi ↗ · pubmed ↗
- 2Scheenstra B , Princée AMA, Imkamp MSV, Kietselaer B, Ganushchak YM, Van’t Hof AWJ et al Last-minute cancellation of adult patients scheduled for cardiothoracic surgery in a large Dutch tertiary care centre. Eur J Cardiothorac Surg 2021;61:225–32.34021310 10.1093/ejcts/ezab 246PMC 8715847 · doi ↗ · pubmed ↗
- 3Wong DJN , Harris SK, Moonesinghe SR; SNAP-2: EPICCS Collaborators; Health Services Research Centre, National Institute of Academic Anaesthesia; Study Steering Group. Cancelled operations: a 7-day cohort study of planned adult inpatient surgery in 245 UK National Health Service hospitals. Br J Anaesth 2018;121:730–8.30236235 10.1016/j.bja.2018.07.002 · doi ↗ · pubmed ↗
- 4Tezel C , Derdiyok O, Evman S, Kanbur S, Demir M, Alpay L et al Prospective study of last-minute cancellations of thoracic surgery operations and preventive measures. Eur Res J 2018;52(Suppl 62):PA 3166.
- 5Dimitriadis PA , Iyer S, Evgeniou E. The challenge of cancellations on the day of surgery. Int J Surg 2013;11:1126–30.24035905 10.1016/j.ijsu.2013.09.002 · doi ↗ · pubmed ↗
- 6Haana V , Sethuraman K, Stephens L, Rosen H, Meara JG. Case cancellations on the day of surgery: an investigation in an Australian paediatric hospital. ANZ J Surg 2009;79:636–40.19895520 10.1111/j.1445-2197.2009.05019.x · doi ↗ · pubmed ↗
- 7Derdiyok O , Tezel C, Tezel Y. Last minute cancellation in Thoracic Surgery Education Research Hospital. J Public Health Dis Prev 2020;3:105.
- 8Hovlid E , Bukve O, Haug K, Aslaksen AB, von Plessen C. A new pathway for elective surgery to reduce cancellation rates. BMC Health Serv Res 2012;12:154.22686475 10.1186/1472-6963-12-154PMC 3465216 · doi ↗ · pubmed ↗