Concomitant Surgical Ablation in Atrial Fibrillation Patients Undergoing Cardiac Surgery for Isolated Coronary and Aortic Valve Disease: A Multicentre Study from The Netherlands Heart Registration
M Agustina Bayón, Miriam A Scheurwater, Niels J Verberkmoes, Massimo A Mariani, Maaike M Roefs, Job van der Palen, Lukas R C Dekker, Yuri Blaauw, Thomas J van Brakel, S Bramer, S Bramer, R A F de Lind van Wijngaarden, B M J A Koene, J A Bekkers, G J F Hoohenkerk, A L P Markou

TL;DR
This study examines the outcomes of concomitant surgical ablation in patients with atrial fibrillation undergoing heart surgery in the Netherlands, finding longer surgical times but better survival and quality of life.
Contribution
The study provides new insights into the effectiveness of concomitant surgical ablation in non-mitral valve surgeries like CABG and AVR.
Findings
CSA patients had longer cardiopulmonary bypass and aortic cross clamping times.
CSA was associated with higher survival rates and improved mental quality of life.
CSA performance during CABG and AVR increased from 29.7% in 2018 to 44.4% in 2021.
Abstract
Concomitant surgical ablation (CSA) is recommended for atrial fibrillation (AF) patients undergoing cardiac surgery; however, its effects in non-mitral valve surgeries, specifically coronary artery bypass grafting (CABG) and aortic valve replacement (AVR), are less studied. This study aims to analyse outcomes and trends of CSA performance in the Netherlands. This nationwide multicentre study utilized data from the Netherlands Heart Registration. AF patients undergoing CABG or AVR between 2013 and 2021 were included. Temporal trends in CSA performance were analysed and a multivariable regression model adjusted for confounders when comparing CSA and non-CSA. A total of 3260 patients were included, of which 1081 underwent CSA. CSA patients showed longer cardiopulmonary bypass (CPB) (111 vs 80, mean difference between groups: 31 min [95% CI, 27-34, P < 0.001]) and aortic cross clamping…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
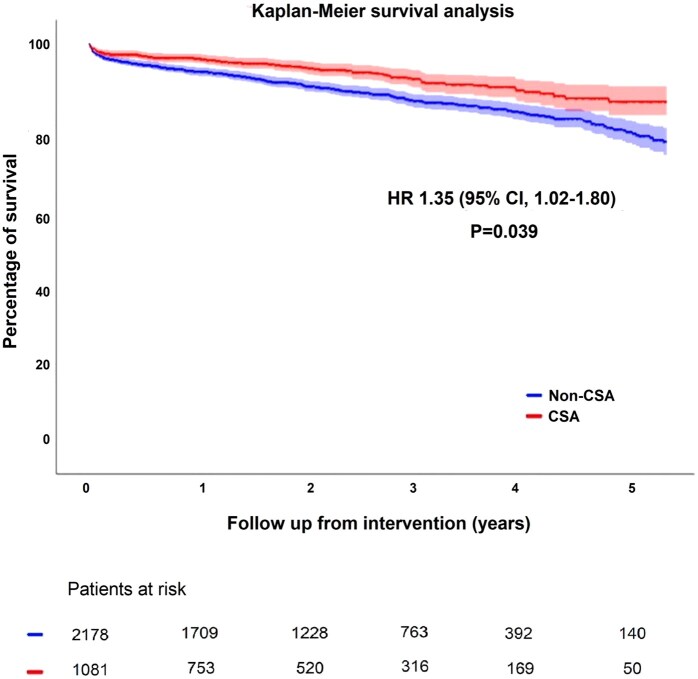 Figure 1
Figure 1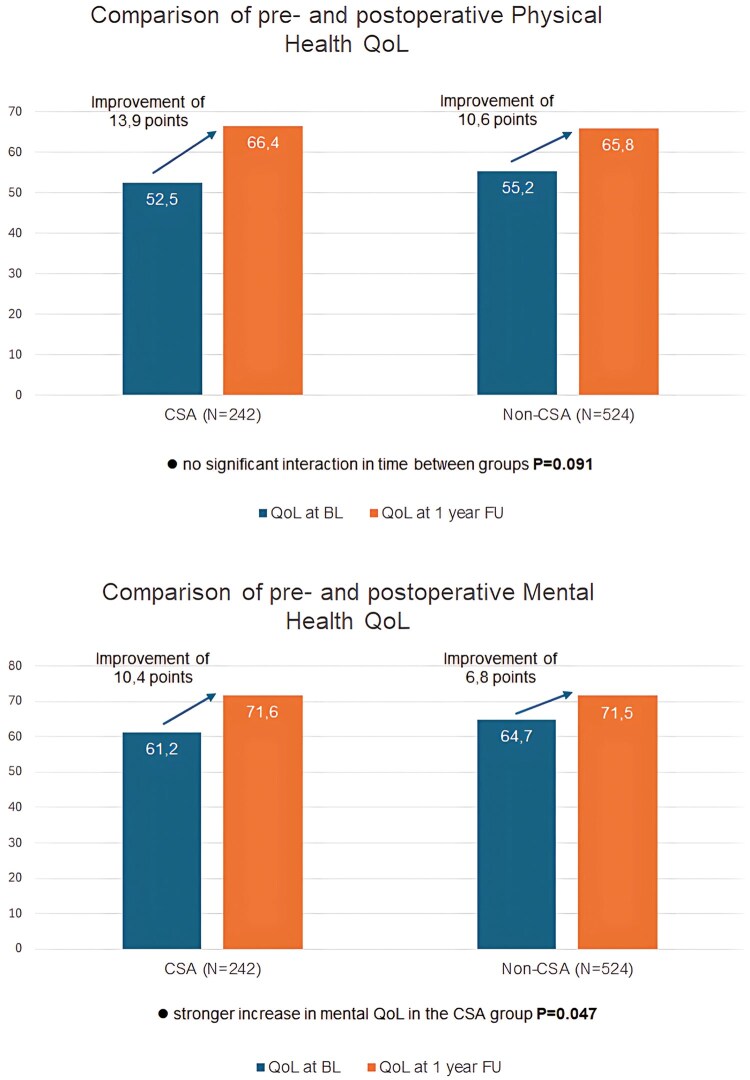 Figure 2
Figure 2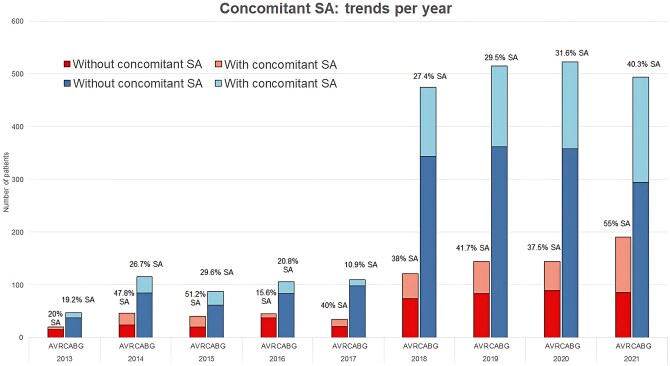 Figure 3
Figure 3| Non-CSA group N = 2179 | CSA group N = 1081 |
| |
|---|---|---|---|
| AVR, | 453 (20.79) | 334 (30.90) | <0.001 |
| CABG, | 1726 (79.21) | 747 (69.10) | <0.001 |
| Sex (males), | 1718 (78.8) | 873 (80.8) | 0.219 |
| Age (years), median [IQR] | 73 [67-77] | 71 [65-75] | <0.001 |
| BMI, median [IQR] | 27.4 [24.8-30.4] | 27.8 [25.2-30.6] | 0.024 |
| eGFR <50, | 394 (18.1) | 142 (13.2) | <0.001 |
| DM, | 642 (29.4) | 281 (26.0) | 0.041 |
| LVEF <30%, | 161 (7.4) | 62 (5.7) | 0.078 |
| PAH >40 mmHg, | 29 (1.3%) | 8 (0.7%) | 0.134 |
| Chronic lung disease, | 277 (12.7) | 126 (11.7) | 0.432 |
| PVD, | 302 (13.9) | 113 (10.5) | 0.005 |
| CVA, | 220 (10.1) | 110 (10.2) | 0.944 |
| EuroSCORE II, median [IQR] | 1.91 [1.27-3.19] | 2.28 [1.6-3.62] | <0.001 |
| Use of CPB, | 1893 (86.9) | 1033 (95.6) | <0.001 |
| Non-CSA group N = 2179 | CSA group N = 1081 |
| Delta | Adjusted | Delta after adjustment | |
|---|---|---|---|---|---|---|
| CPB time (min) | 80.4 (SD 45) | 111 (SD 50) | <0.001 | 31 | <0.001 | 18 |
| AoX time (min) | 52 (SD30) | 67 (SD 33) | <0.001 | 15 | <0.001 | 8 |
| Length of hospital stay (days) | 6.5 (SD 5.3) | 6.95 (7.9) | 0.419 | – | 0.255 | – |
| Postoperative outcomes | OR | 95% CI |
|
|---|---|---|---|
| In-hospital mortality | 0.76 | 0.43-1.34 | 0.350 |
| In-hospital CVA/TIA | 0.52 | 0.26-1.06 | 0.071 |
| In-hospital CVA | 0.50 | 0.22-1.18 | 0.116 |
| In-hospital TIA | 0.59 | 0.16-2.14 | 0.425 |
| Pneumonia | 0.71 | 0.47-1.09 | 0.118 |
| Urinary tract infection | 1.05 | 0.52-2.12 | 0.897 |
| ICU re-admission | 1.16 | 0.75-1.77 | 0.506 |
| Renal failure | 1.57 | 0.94-2.61 | 0.083 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Acute Myocardial Infarction Research
INTRODUCTION
Atrial fibrillation (AF) is the most common cardiac arrhythmia, associated with significant morbidity, mortality, and increased healthcare costs.1^,^2 For AF patients undergoing cardiac surgery, concomitant surgical ablation (CSA) is recommended, due to its association with more favourable outcomes. The 2024 ESC/ACTS guidelines and the 2023 ACC/AHA guideline for the diagnosis and management of atrial fibrillation3^,^4 recommend CSA for mitral valve surgery (class I, evidence level A) and non-mitral valve surgery (class IIa, evidence level B). However, CSA is not consistently performed in patients with AF.5
Previous research demonstrated that CSA can be performed safely6–9 and is associated with positive postoperative outcomes including maintenance of sinus rhythm, reduced stroke incidence and improved survival.6^,^7^,^9–11
Most studies, including those reflected in recent guidelines,3^,^4 have primarily focused on outcomes of CSA in patients undergoing mitral valve interventions, where AF is frequent and its pathophysiology and aetiology with mitral valve disease often overlap. In contrast, the outcomes of CSA in combination with non-mitral valve surgery, particularly coronary artery bypass grafting (CABG) or aortic valve replacement (AVR), remain unexplored.
This study aims to evaluate CSA’s performance, outcomes, safety, and trends in AF patients undergoing CABG and AVR, the most commonly performed non-mitral valve surgeries.
METHODS
Source of study data
Data from all patients undergoing cardiac surgery were obtained from the Netherlands Heart Registration (NHR), a prospective, nationwide, mandatory quality-control registry dedicated to collecting comprehensive data on cardiovascular diseases and (surgical) interventions in the Netherlands.12^,^13 The NHR collects data including demographics, intervention type, parameters concerning perioperative morbidity and mortality, and mid-term survival from all cardiac surgeries performed. To obtain reliable data, the NHR has an advanced, certified data quality control system in place to ensure data completeness and quality.14
All patient, surgeon, and centre data were anonymized. No problems were reported regarding the quality of the long-term follow-up data from the NHR.
Study design and population
The current study is a retrospective, multicentre cohort study of prospectively collected data from 16 cardiothoracic centres in the Netherlands. Included patients were aged 18 years and older, with a history of AF and undergoing isolated CABG or isolated AVR, with or without CSA, between 2013 and 2021. Exclusion criteria included: previous cardiac surgery, robotic or minimally invasive surgery, and other concomitant interventions. Follow-up closed in December 2021.
Study end-points
Primary end-points were (in-hospital) mortality, cerebrovascular accident (CVA) or transient ischaemic attack (TIA), and cumulative survival. Additionally, trends in CSA performance over time in the Netherlands were analysed.
Mortality data were obtained from municipal records and were complete for all patients.
Secondary end-points included length of hospital stay, cardiopulmonary bypass (CPB), and aortic cross clamping (AoX) times. Additional end-points included pneumonia, urinary tract infection, re-admission to the intensive care unit (ICU), and postoperative renal failure. Other end-points included quality of life (QoL) comparison at baseline and 1-year follow-up, from SF-12 or SF-36 questionnaires.
Missing values
The overall proportion of missing data was low (1.31%). All mandatory NHR variables were complete, but the EuroSCORE II had higher missing rates (9.0%).
Statistical analysis
Normality of continuous variables was assessed by skewness and kurtosis, and by visual inspection of histograms. Continuous data were presented as mean with standard deviation (SD), or median with interquartile range (IQR) for non-normally distributed data. Group comparisons were conducted using the Student’s t-test or Mann-Whitney U-test for continuous variables and the Chi-squared or Fisher’s exact test for categorical variables.
A multivariable Cox regression model was implemented to evaluate time to event outcomes and mortality between patients undergoing CSA or not, while adjusting for statistically significant confounders. The model corrected for age, CPB use, renal impairment, LVEF <30%, peripheral vascular disease (PVD), diabetes mellitus (DM), and EuroSCORE II. All variables contributed meaningfully to the model. Cumulative survival was analysed with Kaplan-Meier curves, with differences between groups assessed by the log-rank test. Hazard ratios (HR) with 95% confidence intervals (CI) were obtained. CABG and AVR were combined into one mixed group to increase the sample size. An interaction analysis was conducted to exclude that the type of intervention (CABG or AVR) would modify the effect of performing CSA or not.
Binary logistic regression based on the abovementioned model was applied to analyse categorical outcomes. Linear regression was used for analysing continuous outcomes when the data were normally distributed. For skewed data, a log-transformation was applied to obtain normality of the data. Nevertheless, for interpretation purposes, the non-transformed means (SD) are presented.
Mixed linear models (MLMs) were used to evaluate pre- and postoperative QoL scores with the main parameter of interest being the group (CSA, non-CSA) by time interaction. A subanalysis compared survival and QoL outcomes between CABG and AVR patients.
A P-value < 0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics 28 (SPSS Inc., Chicago, IL, USA) and RStudio 2023.12.1, Build 402.
Ethical statement
The study was approved by the institutional review board MEC-U (W19.270) and conducted in agreement with the principles of the Declaration of Helsinki. A waiver for informed consent for analysis with the data of the NHR data registry was obtained.
RESULTS
Baseline characteristics
The NHR database contained 3260 AF patients who underwent either CABG (N = 2473) or AVR (N = 787) between 2013 and 2021. Of these patients, 1081 (33.16%) received CSA. Patients undergoing AVR were more likely to undergo CSA than patients undergoing CABG (30.9% vs 20.8%, P < 0.001). Patients undergoing CSA were younger (71 [65-75] vs 73 [67-77] years old, P < 0.001) and had a higher BMI (27.8 [25.2-30.6] vs 27.4 [24.8-30.4], P = 0.024) and a higher EuroSCORE II (2.28 [1.6-3.62] vs 1.91 [1.27-3.19], P < 0.001). They were also less likely to have a history of renal impairment (13.2% vs 18.1%, P < 0.001), PVD(10.5% vs 13.9%, P = 0.005), and DM (26.0% vs 29.4%, P = 0.041). Baseline characteristics are summarized in Table 1.
Regression analyses
Mortality data were complete for all patients. A survival analysis was conducted (Figure 1; Supplementary Table S2), which showed higher cumulative survival rates in the CSA group over the follow-up period. The median follow-up time for the CSA group was 1.9 years (0.8-3.4) with a survival rate of 92.5%. For non-CSA patients, the median follow-up was 2.3 years (1.2-3.6) with a survival rate of 86.4%, HR 1.66 (95% CI, 1.30-2.13, P < 0.001).
Kaplan-Meier Survival Analysis. Adjusted P-value for age, CPB use, renal impairment, LVEF <30%, PVD, DM, and EuroSCORE II. Abbreviation: CSA = concomitant surgical ablation
A multivariable Cox regression model adjusted for the following significant confounders: age, CPB use, renal impairment, LVEF <30%, PVD, DM, and EuroSCORE II. An interaction term between the type of intervention (CABG or AVR) and the performance of CSA or not was tested to evaluate potential effect modification. This interaction was not statistically significant (P = 0.267) and did not improve model fit; therefore, it was excluded from the analysis.
After adjustment for confounders, the observations in the survival analysis became subtler but remained statistically significant, HR 1.35 (95% CI, 1.02-1.80, P = 0.039).
Linear regression analysis revealed longer CPB times in the CSA patients (111 vs 80 min with a difference of 31 min between groups [95% CI, 27-34, P < 0.001]). AoX times were also longer in the CSA group (67 vs 52 min, with a difference of 15 min [95% CI, 13-17, P < 0.001]). After correcting for confounders, the delta decreased to 18 (95% CI, 16-21, P < 0.001) and 8 (95% CI, 6-10, P < 0.001) min of CPB and AoX times, respectively.
The length of hospital stay did not differ between groups (6.5 vs 7.0 days, with a difference of 0.4 days [95% CI, 0.1-0.9, P = 0.255]).
Binary logistic regression analysis showed that CSA was not associated with postoperative complications: in-hospital mortality (OR= 0.76, 95% CI, 0.43-1.34, P = 0.350), in-hospital CVA/TIA (OR= 0.52, 95% CI, 0.26-1.06, P = 0.071), in-hospital CVA (OR = 0.50, 95% CI, 0.22-1.18, P = 0.116), in-hospital TIA (OR = 0.59, 95% CI, 0.16-2.14, P = 0.425), pneumonia (OR = 0.71, 95% CI, 0.47-1.09, P = 0.118), urinary tract infection (OR = 1.05, 95% CI, 0.52-2.12, P = 0.897), ICU re-admission (OR = 1.16, 95% CI, 0.75-1.77, P = 0.506), and renal failure (OR= 1.57, 95% CI, 0.94-2.61, P = 0.083). Peri- and postoperative outcomes are displayed in Tables 2 and 3.
Quality of life
MLM was conducted to evaluate physical and mental QoL. MLM enabled the inclusion of repeated measures and accounted for both fixed and random effects allowing the analysis of 766 patients. In the CSA group (N = 242), the mean physical health score improved from 52.5 to 66.4 during follow-up, with a difference of 13.9 points (95% CI, 10.7-17.1 P < 0.001), whereas in the non-CSA group (N = 524), the score went from 55.2 to 65.8 with a difference of 10.6 points (95% CI, 8.4-12.8, P < 0.001). MLM were applied to assess differences of improvement between groups over time, showing no significant difference (P = 0.091).
Mental health scores also improved in the CSA group from 61.2 to 71.6 with a difference of 10.4 points (95% CI, 7.5-13.5, P < 0.001) and in the non-CSA group from 64.7 to 71.5 with a difference of 6.8 points (95% CI, 4.7-8.8, P < 0.001). MLM showed a significant group by time interaction, indicating a stronger increase in mental QoL in the CSA group (P = 0.047) (Figure 2).
Comparison of Physical and Mental Health QoL Pre- and Postoperative. Abbreviations: BL: base line; CSA: concomitant surgical ablation; FU: follow-up; QoL: quality of life
Trends of performing CSA
Figure 3 shows the total volume per year of CABGs or AVRs performed in AF patients. From 2013 to 2017, we observed low proportions of patients operated per year. From 2018 to 2021, an increasing tendency of performing CSA was observed in the mixed population, from 29.7% in 2018 to 44.4% in 2021. The rates increased from 27.4% to 40.3% in CABG patients and from 38.8% to 55.0% in AVR patients.
Yearly Overview of CSA Performance, Showing the Percentage of Patients Who Received CSA. A significant increase in registered operations is observed from 2018 on, indicating underreporting of AF as preoperative characteristic and less accurate representation of the surgical trends before this year. Abbreviations: AVR: aortic valve replacement; CABG: coronary artery bypass grafting; SA: surgical ablation
CSA was more frequently performed in AVR patients compared to CABG patients, with stable proportions, except for a notable increase in 2021 when CSA became more common than non-CSA procedures.
Subanalysis per intervention group
The survival analysis of the different intervention types (CABG and AVR) showed no statistically significant difference between the CSA and non-CSA groups.
QoL scores improved postoperatively for both CABG and AVR patients, with no significant group by time interactions.
A detailed description of the subanalyses can be found in the Supplementary Material.
DISCUSSION
This study was conducted using a large national database from the NHR and aimed to evaluate the outcomes and safety of performing CSA in AF patients undergoing the most common non-mitral valve surgeries: CABG and AVR. We found that CSA patients presented longer CPB and AoX times, but no significant differences in postoperative complications such as in-hospital mortality, stroke, pneumonia, or renal failure. CSA was associated with improved survival and mental QoL compared to non-CSA.
Intra- and postoperative comparison
CSA patients had longer operation times. Specifically, the mean CPB-time in the CSA group was 18 min longer, while the AoX-time was 8 min longer than in the non-CSA group. However, these time extensions are clinically unlikely to be relevant, as supported by the findings of this study, which showed no significant differences in major postoperative outcomes, such as in-hospital mortality, stroke, pneumonia, or renal failure. Literature on these specific variables (CPB and AoX times) is limited, as they are often not reported. The PRAGUE-12 trial,8 a randomized multicentre study published in 2012, included 224 AF patients undergoing valve and/or coronary surgery, who were randomized to receive CSA or not, revealing that CPB was 28 min longer and AoX, 27 min longer in the CSA group. Although these values differ from our findings, a direct comparison is challenging due to the inclusion of more complex procedures in the PRAGUE-12 trial and its limited patient population. To our knowledge, no recent studies have specifically compared CPB- and AoX times in patients undergoing isolated CABG or AVR with or without CSA. Although in our data no information is available regarding the lesion set applied, this difference observed in operation times could suggest a less complex ablation such as pulmonary vein isolation.
A key finding is that early mortality and in-hospital CVA/TIA rates did not significantly differ between groups. This contrasts with the results of the STS database study,5 where CSA was associated with lower 30-day mortality and stroke, but aligns with observations from other studies.7^,^8 Future research should account for contemporary surgical strategies and consider the role of left atrial appendage (LAA) occlusion, as it may be a confounder for postoperative CVA/TIA, as demonstrated in the LAAOS III trial,15 which linked LAA occlusion to a reduced risk of ischaemic stroke.
Another interesting observation in our data was that a higher proportion of off-pump CABG was observed in the non-CSA group. This can suggest that CSA is generally less frequently performed when CPB is not used, maybe due to a more challenging technique or haemodynamic problems when ablating the pulmonary veins. Studies focused on evaluating off-pump CABG with CSA could offer insights into this topic and its potential consequences.
Follow-up
Regression analyses showed a statistically significant survival difference favouring CSA patients. This finding contributes to the limited and sometimes contradictory evidence regarding the mid- and long-term effects of CSA. However, our results align with a general trend observed by other studies16–18 which showed improved survival in CSA patients. The exact reasons for this survival advantages remain unclear, but evidence from randomized control trials (RCT), such as CASTLE-AF19 and EAST-AFNET 4,20 suggest that a more aggressive rhythm control strategy may reduce mortality and cardiovascular events in AF patients. Although the mechanisms driving these benefits are not yet fully understood, these findings emphasize the importance of future research to further investigate the impact of assertive rhythm control.
We also observed an improvement in QoL in both groups, with stronger effects in the CSA cohort. Improved QoL is often associated with freedom from AF and sinus rhythm maintenance,21 potentially related to reduced medication use and fewer hospital visits.
Trends
This study aimed to illustrate the frequency of CSA performance over the years. Prior to 2018, the number of surgical interventions reported was very limited when compared to 2018 onwards, likely reflecting underreporting of AF in the NHR. Consequently, the percentage of CSA before 2018 may be overestimated and trends from that period are not fully representative. Consequently, analysis of the trends should focus on data from 2018 until 2021. In these recent years, the increase in AF and CSA registration may relate to updated clinical guidelines emphasizing its beneficial effects, as seen in a recently published study from the USA,22 showing CSA rates increased from 2.1% to 17.4% after the STS guideline update.4
A multicentre study published in 2024 from Poland11 reported CSA (with or without LAA occlusion) in 10.26% of AF patients undergoing cardiac surgery, with comparable low rates for isolated CABG (9.6%) and AVR (11.3%). A previous Polish study9 found CSA in only 4.4% of AF patients undergoing CABG. In contrast, two STS studies18^,^23 reported higher CSA rates of 30.5% in AF patients undergoing CABG and 33.1% in AVR patients. In this study, the CSA rate reached 44.4% in the final study year. The rise in CSA procedures may reflect updated guidelines and research highlighting its potential benefits. As surgical strategies vary by country, presenting country-specific data is essential to refine techniques and outcomes.
Limitations
The NHR database was initially designed for quality-control rather than for research purposes. Therefore, certain key variables, such as AF type, left atrial dimensions, lesion set, energy source, LAA exclusion, or other long-term outcomes, are either missing or insufficiently documented, limiting specific analyses.
Additionally, AF registration before 2018 was incomplete, possibly leading to an overestimation of CSA rates in earlier years, which limits the analysis of trends.
Subanalyses of the AVR and CABG groups showed no significant survival differences within these subgroups, likely due to smaller sample sizes, highlighting the need for larger studies to assess specific intervention groups.
The reasons for not performing CSA remain unclear, with potential selection bias favouring patients with fewer comorbidities, smaller atria, or less advanced types of AF. While PSM adjusts for confounders, it does not replace randomization, so the results should be interpreted with caution.
CONCLUSION
This nationwide, retrospective multicentre registry based study in AF patients undergoing isolated CABG or AVR found that CSA was associated with improved survival and better postoperative mental QoL. While CSA was associated with slightly longer CPB- and AoX times, it showed no significant differences in major postoperative complications, including mortality, stroke, and renal failure. CSA rates increased from 29.7% in 2018 to 44.4% in 2021, reflecting significant progress and positioning Netherlands ahead internationally. While this is encouraging, there is significant room for further improvement through enhanced care implementation and ongoing research.
Supplementary Material
ezaf244_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schnabel RB , Yin X, Gona P, et al 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154-162.25960110 10.1016/S 0140-6736(14)61774-8PMC 4553037 · doi ↗ · pubmed ↗
- 2Tsao CW , Aday AW, Almarzooq ZI, et al; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147:e 93-e 621.36695182 10.1161/CIR.0000000000001123 PMC 12135016 · doi ↗ · pubmed ↗
- 3Van Gelder IC , Rienstra M, Bunting KV, et al ESC guidelines for the management of atrial fibrillation. Eur Heart J. 2024;45:ehae 176.
- 4Joglar JA , Chung MK, Armbruster AL, et al; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation. Circulation. 2024;149:e 1-e 156.38033089 10.1161/CIR.0000000000001193 PMC 11095842 · doi ↗ · pubmed ↗
- 5Badhwar V , Rankin JS, Ad N, et al Surgical ablation of atrial fibrillation in the United States: trends and propensity matched outcomes. Ann Thorac Surg. 2017;104:493-500.28669501 10.1016/j.athoracsur.2017.05.016 · doi ↗ · pubmed ↗
- 6Huffman MD , Malaisrie SC, Karmali KN. Concomitant atrial fibrillation surgery for people undergoing cardiac surgery. JAMA Cardiol. 2017;2:334-335.28196179 10.1001/jamacardio.2016.5404 · doi ↗ · pubmed ↗
- 7Mc Clure GR , Belley-Cote EP, Jaffer IH, et al Surgical ablation of atrial fibrillation: a systematic review and meta-analysis of randomized controlled trials. Europace. 2018;20:1442-1450.29186407 10.1093/europace/eux 336 · doi ↗ · pubmed ↗
- 8Budera P , Straka Z, Osmančík P, et al Comparison of cardiac surgery with left atrial surgical ablation vs. cardiac surgery without atrial ablation in patients with coronary and/or valvular heart disease plus atrial fibrillation: final results of the PRAGUE-12 randomized multicentre study. Eur Heart J. 2012;33:2644-2652.22930458 10.1093/eurheartj/ehs 290PMC 3485575 · doi ↗ · pubmed ↗