Efficacy and Cost-Effectiveness of MDM2 Fluorescence In Situ Hybridization (FISH) in Morphologically Atypical Spermatic Cord Lipomas
Zobash Noor, Shaymaa Hegazy, Rana Naous

TL;DR
This study shows that MDM2 FISH testing can help distinguish rare liposarcomas from benign lipomas in spermatic cord tissue during hernia repairs.
Contribution
The study evaluates the diagnostic accuracy and cost-effectiveness of MDM2 FISH in atypical spermatic cord lipomas.
Findings
Only 2.3% of atypical spermatic cord lipomas tested positive for MDM2 amplification, indicating liposarcoma.
97.7% of cases had reactive-type atypia with negative FISH results, confirming benign lipomas.
The authors suggest using FISH testing for lesions larger than 10 cm to avoid misdiagnosis.
Abstract
Background: Spermatic cord lipomas originate from preperitoneal adipose tissue within the internal spermatic fascia and are found in 20%-70% of all inguinal hernia repairs. Morphologically, spermatic cord lipomas may harbor some atypical features, including increased stromal cellularity with thickened fibrous bands, occasional lipoblasts, and stromal nuclear atypia or hyperchromasia, raising concern for well-differentiated liposarcoma (WDLS) versus reactive-type atypia. Fluorescence in situ hybridization (FISH) for MDM2 amplification would be the gold standard test in such cases. The aim of this study was to evaluate the efficacy and cost-effectiveness of MDM2 FISH in diagnostically discrimination morphologically atypical spermatic cord lipoma cases at our institution. Methods: All cases with “specimen type” labeled as “spermatic cord lipoma” between 2018 and 2023 were retrospectively…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
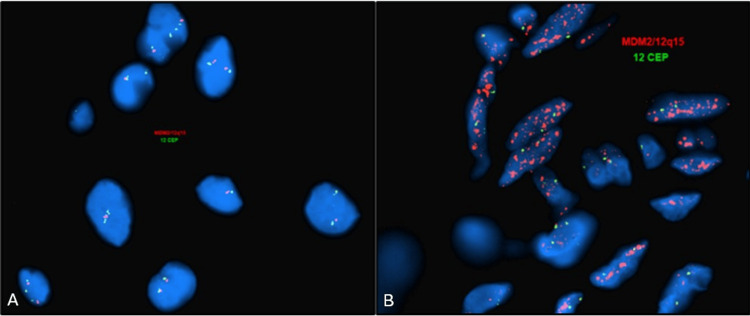 Figure 1
Figure 1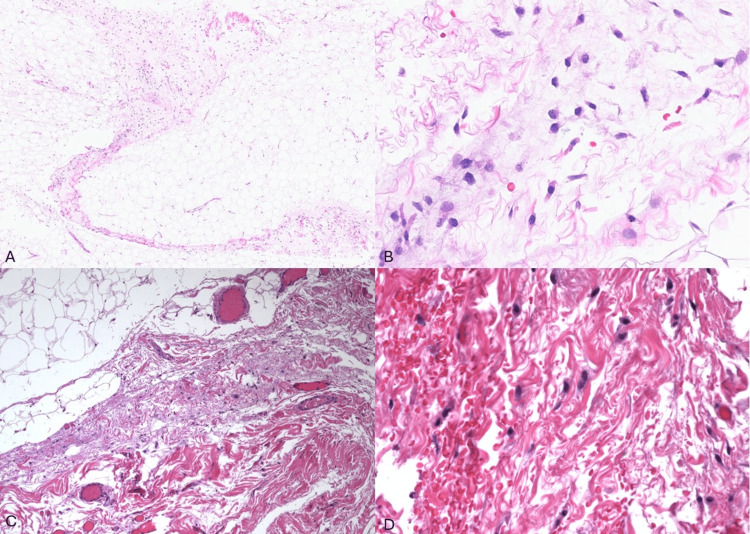 Figure 2
Figure 2| Case # | Age | Laterality | Size (cm) | MDM2 FISH | Final Diagnosis |
| 1 | 72 | Left | 5 | Negative | Reactive atypia |
| 2 | 59 | Right | 7.7 | Negative | Reactive atypia |
| 3 | 59 | Right | 20 | Negative | Reactive atypia |
| 5 | 73 | Right | 6.2 | Negative | Reactive atypia |
| 6 | 58 | Right | 6.3 | Negative | Reactive atypia |
| 7 | 61 | Left | 6.7 | Negative | Reactive atypia |
| 8 | 77 | Left | 6.5 | Negative | Reactive atypia |
| 9 | 63 | Left | 3.7 | Negative | Reactive atypia |
| 10 | 69 | Left | 14.8 | Negative | Reactive atypia |
| 11 | 46 | Left | 3.9 | Negative | Reactive atypia |
| 12 | 78 | Right | 6 | Negative | Reactive atypia |
| 13 | 58 | Right | 9.7 | Negative | Reactive atypia |
| 14 | 72 | Right | 29.2 | Negative | Reactive atypia |
| 15 | 47 | Right | 6.4 | Negative | Reactive atypia |
| 16 | 67 | Bilateral | 16 | Negative | Reactive atypia |
| 18 | 46 | Left | 10.8 | Negative | Reactive atypia |
| 19 | 66 | Left | 10.8 | Negative | Reactive atypia |
| 20 | 25 | Left | 5.2 | Negative | Reactive atypia |
| 21 | 63 | Left | 6.5 | Negative | Reactive atypia |
| 22 | 54 | Left | 6.7 | Negative | Reactive atypia |
| 23 | 81 | Left | 13.3 | Negative | Reactive atypia |
| 24 | 64 | Left | 5.7 | Negative | Reactive atypia |
| 25 | 87 | Left | 9.8 | Negative | Reactive atypia |
| 26 | 77 | Left | 6.5 | Negative | Reactive atypia |
| 27 | 57 | Left | 4.7 | Negative | Reactive atypia |
| 28 | 65 | Left | 5.5 | Negative | Reactive atypia |
| 29 | 65 | Left | 6.6 | Negative | Reactive atypia |
| 31 | 47 | Right | 7.6 | Negative | Reactive atypia |
| 32 | 63 | Right | 3.8 | Negative | Reactive atypia |
| 33 | 78 | Left | 7.2 | Negative | Reactive atypia |
| 34 | 67 | Left | 4.2 | Negative | Reactive atypia |
| 35 | 63 | Right | 3.8 | Negative | Reactive atypia |
| 36 | 63 | Left | 7 | Negative | Reactive atypia |
| 37 | 53 | Left | 8.6 | Negative | Reactive atypia |
| 38 | 69 | Right | 5.4 | Negative | Reactive atypia |
| 39 | 65 | Left | 6 | Negative | Reactive atypia |
| 40 | 45 | Right | 2.1 | Negative | Reactive atypia |
| 41 | 88 | Right | 6.5 | Negative | Reactive atypia |
| 42 | 63 | Right | 9.3 | Negative | Reactive atypia |
| 43 | 72 | Right | 11 | Positive | Well-differentiated liposarcoma |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrologic and reproductive health conditions · Testicular diseases and treatments · Renal and related cancers
Introduction
Spermatic cord lipomas originate from preperitoneal adipose tissue within the internal spermatic fascia and are found in 20%-70% of all inguinal hernia repairs [1]. Morphologically, spermatic cord lipomas may harbor some atypical features, including increased stromal cellularity with thickened fibrous bands, occasional pseudolipoblasts, and stromal nuclear atypia or hyperchromasia, raising concern for well-differentiated liposarcoma versus reactive-type atypia. Fluorescence in situ hybridization (FISH) for MDM2 gene amplification would be the gold standard test [2] in such cases to help determine the nature of such atypical spermatic cord lipomas. The aim of this study was to evaluate the efficacy of MDM2 FISH in diagnostically discriminating morphologically atypical spermatic cord lipoma cases at our institution, as well as assessing its cost-effectiveness by evaluating its clinical utility in comparison to testing burden.
Materials and methods
All cases with “specimen type” labeled as “spermatic cord lipoma” between 2018 and 2023 were retrospectively retrieved from our institutional archives. Cases with a prior history of spermatic cord well-differentiated liposarcoma with positive MDM2 amplification were excluded. Cases with atypical features, including increased stromal cellularity with thickened fibrous bands, presence of occasional lipoblasts, and stromal nuclear atypia or hyperchromasia that had MDM2 FISH performed, were included in the study group. Patient age, specimen size, specimen laterality, MDM2 gene amplification status, and corresponding final diagnosis were recorded.
For MDM2 FISH testing, three 4-µm-thick tissue serial sections were cut from formalin-fixed paraffin-embedded (FFPE) tissue blocks for tissue adequacy evaluation and fluorescence in situ hybridization (FISH) studies analysis. The slides for the tissue adequacy assessment were stained with hematoxylin and eosin and reviewed by two pathologists. The hybridization was performed using commercially available dual-color probes: MDM2/SE12 12q15/12p11.1q11.1; MDM2 (orange spectrum) (Kreatech Biotechnologies, Amsterdam, Netherlands) and the SE12 (green spectrum) probes (Kreatech Biotechnologies, Amsterdam, Netherlands). MDM2 FISH analysis was manually performed and quantitatively assessed by analysis of a minimum of 60 cells in the targeted region of interest circled by an expert pathologist along with a screen outside the region of interest. These areas are reviewed by at least two technologists with minimal discrepancy. Positive results of MDM2 gene amplification by FISH are defined by a ratio gene/chromosome greater than two, while negative results are defined by a gene/chromosome ratio less than two.
Results
Three hundred twenty spermatic cord lipoma specimens were retrieved. Forty-three out of 320 cases had atypical features corresponding to thickened fibrous septate with variable increase in cellularity, stromal nuclear atypia, and/or occasional pseudolipoblasts. The patient’s demographics including age, specimen laterality, size of the spermatic cord lipoma cases, and MDM2 FISH amplification status are summarized in Table 1.
All patients were identified as males per their medical record and presented with clinical and/or radiologic impression of inguinal hernia/cord lipoma. The results showed that one out of 43 (2.3 %) cases demonstrated MDM2 amplification by FISH (Figures 1A, 1B) with a gene/chromosome ratio of 30.9 corresponding to a diagnosis of well-differentiated liposarcoma.
MDM2 FISH gene amplification results.A: Negative FISH for MDM2 gene amplification in an atypical spermatic cord lipoma case compatible with reactive atypia. B: Positive FISH for MDM2 gene amplification in an atypical spermatic cord lipoma case compatible with a diagnosis of well-differentiated liposarcoma. FISH: fluorescence in situ hybridization, CEP: Centromere Enumeration Probe.
The patient was a 72-year-old man presenting for an inguinal hernia repair surgery. The size of his “lipoma of cord” specimen was 11 cm in maximum dimension (11 x 6 x 1.3 cm). Due to the diagnosis of well-differentiated liposarcoma in the setting of inguinal hernia repair, the patient subsequently underwent a right orchiectomy which showed a small focus of residual well-differentiated liposarcoma with no areas of dedifferentiation and negative margins (slides not available). Currently, the patient is undergoing close clinical follow-up with no recurrences to date. The remaining 42 (97.7%) cases, although had overlapping morphologic features with our well-differentiated liposarcoma case, were negative for MDM2 gene amplification by FISH with a corresponding final diagnosis of spermatic cord lipomas with reactive-type atypia (Figures 2A-2D).
Similar histomorphologic features of atypical spermatic cord lipoma and well-differentiated liposarcoma.A-B: Atypical spermatic cord lipoma case demonstrating, on low- and high-power magnification, thickened fibrous septate with increase in cellularity, stromal nuclear atypia with variation in nuclear size, and occasional hyperchromasia (hematoxylin and eosin (H&E); 10× and 40×). C-D: Well-differentiated liposarcoma case demonstrating similar morphologic features to the atypical spermatic cord lipoma case with variably cellular fibrous septae and stromal atypia (H&E; 10× and 40×).
Discussion
A lipoma of the cord is herniated fat that appears to originate from the preperitoneal fat outside and posterior to the internal spermatic fascia and protrudes through the internal ring lateral to the cord [1]. Although it is commonly found in inguinal hernia repair procedures, it is not always sent for histopathology evaluation. Lipomas may rarely undergo sarcomatous transformation and evolve into a liposarcoma. Liposarcomas are locally aggressive malignancies with a high incidence of local recurrence and variable prognosis depending on their dedifferentiation status and histologic grade [2]. Complete excision of liposarcomas of the cord is particularly important as local recurrence of these tumors is likely a consequence of incomplete excision with positive surgical resection margins, which can possibly promote tumor seeding through the operative site [3].
According to clinicopathological and molecular genetic characteristics, liposarcomas are grouped per the World Health Organization (WHO) into three categories, namely atypical lipomatous tumor or well-differentiated liposarcoma (ALT-WDLPS)/dedifferentiated liposarcomas, myxoid/round cell liposarcoma, and pleomorphic liposarcoma. Based on histology, a well-differentiated liposarcoma, in particular, the lipoma-like variant, can mimic fatty tissue or a benign lipoma [4]. In this study, we have studied the use of MDM2 amplification by FISH to differentiate a benign lipoma of cord from well-differentiated liposarcoma, as this difference is crucial in prognosis and treatment. In lipomas of the spermatic cord, the presence of fibrous septa containing atypical cells with enlarged hyperchromatic nuclei can mimic a well-differentiated liposarcoma, and MDM2 gene amplification by FISH can be a cost-effective and efficient method in such cases to avoid missing a well-differentiated liposarcoma of the spermatic cord.
The murine double minute (MDM2) oncogene is important in controlling the cell cycle by binding to TP53 and promoting its degradation. Well-differentiated and dedifferentiated liposarcomas share amplifications in the chromosomal region 12Q13-15. These amplifications constantly affect MDM2 and can be detected by FISH [5]. Multiple studies have assessed the utility of immunohistochemical methods to evaluate for MDM2 amplification [6]. Most of these studies have shown a lower sensitivity for immunohistochemical stains (45%) compared to FISH testing in assessing for MDM2 gene amplification. In a study by Kashima et al., the sensitivity and specificity of MDM2 amplification by FISH reached 93.5% and 100%, respectively [7]. Therefore, MDM2 DNA amplification by FISH remains the gold standard for evaluating lipomatous tumors [8].
At the current time, there are no radiologic features that can reliably differentiate between atypical spermatic cord lipomas and well-differentiated liposarcomas, making histologic confirmation essential. Increased awareness and consideration of well-differentiated liposarcoma in the differential of atypical spermatic cord lipoma is essential when evaluating inguinal hernia repairs in order to facilitate accurate diagnosis and appropriate management.
During histological evaluation of a lipoma of spermatic cord specimen and using WHO criteria for assessing atypia in lipomatous lesions, increased stromal cellularity with thickened fibrous bands, occasional pseudolipoblasts, proliferation of spindle or epithelioid cells or stromal nuclear atypia or hyperchromasia can either be evidence of a disguised well-differentiated liposarcoma of cord or just a manifestation of benign reactive atypia. These reactive atypical histologies in a lipoma of cord are most commonly seen secondary to irritation in cases of an obstructed or incarcerated hernia or in long-standing hernias. Accurate recognition in such cases is essential to avoid misdiagnosis; however, it is worth noting that evaluation of such atypical features may be affected by interobserver variability assessment among pathologists. Fluorescence in situ hybridization (FISH) for MDM2 gene amplification can be used to distinguish between benign reactive atypical cells and atypical lipomatous tumor/well-differentiated liposarcoma and would be the gold standard test in such cases [9,10].
Our one case out of 43 (2.3 %) spermatic cord lipoma cases that showed *MDM2 *gene amplification by FISH compatible with well-differentiated liposarcoma occurred in an older male, 72 years old, and had a size larger than 10 cm (11 cm in maximum dimension). Morphologically it showed similar features to the remaining 42 spermatic cord lipoma cases within our cohort and harbored some increase in stromal cellularity with thickened fibrous bands, some myxoid change, mild nuclear atypia with variation in nuclear size, and occasional hyperchromasia. There were no other distinguishing features that could set it apart from the remaining 42 FISH negative cases with no evidence of overtly and diffusely hyperchromatic stromal cells or true lipoblasts with hyperchromatic indented nuclei and cytoplasmic lipid vacuoles that are characteristically seen in well-differentiated liposarcomas. Review of our cohort revealed that eight out of the 43 cases had a specimen size larger than 10 cm with corresponding patient ages ranging from 46 to 81 years old. In a study by Clay et al., the authors recommended MDM2 FISH testing for lipomatous cases with equivocal atypia, lipomatous lesions of the retroperitoneum/pelvis/abdomen, and deep extremity lesions that are >10 cm in patients over 50 years of age [11]. Extrapolating from these criteria, we propose performing MDM2 FISH testing on atypical spermatic cord lipomas greater than 10 cm to avoid potential diagnostic pitfalls.
Although the one positive MDM2 FISH result among our 43 cases may not be statistically significant, the value of MDM2 FISH testing in morphologically atypical spermatic cord lipomas becomes more accentuated when comparing the minor FISH testing costs to the major costs of misdiagnosis leading to surgical re-operation or even delayed patient presentation with metastasis given that evaluation for MDM2 gene amplification status is of therapeutic importance as amplified neoplasms are amenable to targeted therapy [12], and the patient would have missed the opportunity of targeted treatment. Additionally, since FISH testing has a low false negative rate with 93.5% sensitivity and 100% specificity for detecting MDM2 gene amplification [7], this gold standard testing modality further emphasizes its reliability in diagnostically discriminating morphologically atypical spermatic cord lipoma specimens.
To our knowledge, there has not been any study in the literature regarding the use of MDM2 gene amplification by FISH for differentiating atypical cells and increased stromal cellularity in lipomas of spermatic cord from well-differentiated liposarcoma. Although atypical spermatic cord lipoma can mimic well-differentiated liposarcoma, it can be confidently distinguished through FISH for MDM2 gene amplification. Including well-differentiated liposarcoma in the differential diagnosis of atypical spermatic cord lipoma is important to ensure accurate diagnosis and prevent misdiagnosis.
One limitation in our study is the low sample size of 43 atypical spermatic cord lipomas. This may be attributed to the fact that the majority of spermatic cord lipomas in our practice and in general are commonly classic cord lipomas that are characterized by bland fibroadipose tissue and minimal to no atypical features. More studies with increased sample size are necessary to be able to reach definitive cutoff criteria for MDM2 FISH testing on spermatic cord lipomas with atypical features.
Conclusions
In conclusion, our results indicate that 2.3% of morphologically atypical specimens labeled as spermatic cord lipoma at our institution are in fact well-differentiated liposarcomas. Despite this low yield, these findings prove the efficacy of MDM2 FISH in diagnosing well-differentiated liposarcoma in the setting of atypical spermatic cord lipoma specimens. Although 97.7% of our spermatic cord lipomas harbored reactive-type atypia with negative FISH results, which argues against the cost-effectiveness of such testing, we propose performing FISH analysis in cases greater than 10 cm in size to avoid misdiagnosis and ensure optimal patient care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lipomas of the cord and round ligament Ann Surg Lilly MC Arregui ME 58659023520021192361610.1097/00000658-200204000-00018 PMC 1422475 · doi ↗ · pubmed ↗
- 2Fluorescence in situ hybridization for MDM 2 gene amplification as a diagnostic tool in lipomatous neoplasms Mod Pathol Weaver J Downs-Kelly E Goldblum JR 9439492120081850026310.1038/modpathol.2008.84 · doi ↗ · pubmed ↗
- 3Liposarcoma of the spermatic cord: diagnostic and therapeutic issue Acta Clin Croat JeremićD Maletin M Vojinov S Levakov I GrbićD LakićT Trivunić Dajko S 505460202110.20471/acc.2021.60.01.07PMC 830535934588721 · doi ↗ · pubmed ↗
- 4Atypical lipomatous tumor/well differentiated liposarcoma and related mimics with updates. When is molecular testing most cost-effective, necessary, and indicated?Hum Pathol Kilpatrick SE 829114720243813506210.1016/j.humpath.2023.12.005 · doi ↗ · pubmed ↗
- 5Reviving the guardian of the genome: small molecule activators of p 53Pharmacol Ther Nguyen D Liao W Zeng SX Lu H 9210817820172835171910.1016/j.pharmthera.2017.03.013PMC 5601031 · doi ↗ · pubmed ↗
- 6Diagnostic utility of p 16, CDK 4, and MDM 2 as an immunohistochemical panel in distinguishing well-differentiated and dedifferentiated liposarcomas from other adipocytic tumors Am J Surg Pathol Thway K Flora R Shah C Olmos D Fisher C 4624693620122230149810.1097/PAS.0b 013e 3182417330 · doi ↗ · pubmed ↗
- 7Sensitivity of MDM 2 amplification and unexpected multiple faint alphoid 12 (alpha 12 satellite sequences) signals in atypical lipomatous tumor Mod Pathol Kashima T Halai D Ye H 138413962520122269951810.1038/modpathol.2012.90 · doi ↗ · pubmed ↗
- 8MDM 2 FISH testing criteria in adipose tissue tumors with mature adipocytic morphology: a resection case-based study Pathol Res Pract Li L Yue P Du Q Zhang H Song Y 15503925320243813483810.1016/j.prp.2023.155039 · doi ↗ · pubmed ↗