Skeletal Fluorosis: A Case Report of Rare Diagnosis of Computer-cleaner Toxicosis
Tiana Patriarca, Jessica Rivera Pescatore, William Rushton, Emily Sochovka, Julie Brown

TL;DR
A 46-year-old woman developed skeletal fluorosis from regularly inhaling a computer cleaner containing difluoroethane, highlighting the need for awareness of this rare condition.
Contribution
This case report highlights skeletal fluorosis as a rare but serious consequence of computer cleaner inhalation, emphasizing the importance of clinical awareness.
Findings
A patient with chronic inhalation of difluoroethane developed skeletal fluorosis with symptoms including myalgias and joint swelling.
Radiographic findings showed diffuse periosteal reactions consistent with fluorosis.
Discontinuation of inhalant use is recommended to prevent prolonged adverse effects.
Abstract
Skeletal fluorosis is a complication of excess fluoride, which may be associated with chronic inhalation or “huffing” of compressed air cleaners for keyboards and electronics. The rare presentation of this condition can lead to a missed diagnosis and lack of appropriate intervention. Clinicians should be aware of the potential development of fluorosis in patients reporting a history of inhalant abuse. We present a case of skeletal fluorosis in a 46-year-old female patient with a four-month history of daily inhalant use of computer cleaner containing difluoroethane (DFE). She presented to the emergency department after developing myalgias for approximately four months. The pain was alleviated by rest, heat therapy, and pain medication. She was noted to have diffuse bilateral swelling to upper and lower extremities, as well as interphalangeal joint swelling and non-mobile lesions to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1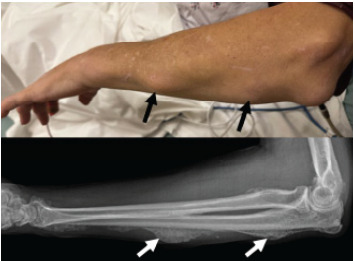 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFluoride Effects and Removal
INTRODUCTION
Inhalants are common substances of misuse, which are widely available and used primarily for their euphoric effects. They consist of hydrocarbon compounds found in a variety of products such as cleaners, dusters, paints, and fuels. These compounds produce their central nervous system effects via gamma-aminobutyric acid receptors similar to ethanol, which itself is an alcohol hydrocarbon derivative. In addition to their euphoric and intoxicating properties, inhalants have also been implicated in cases of cardiovascular toxicities including ventricular dysrhythmias, which likely lead to “sudden sniffing death.” Adolescents and children are particularly susceptible to inhalant misuse due to ease of access and relative affordability.
Halogenated hydrocarbons are hydrocarbon derivates containing an atom from group 17 of the periodic table, typically chlorine or fluorine. 1,1-diflouroethane (DFE) is a fluorinated hydrocarbon, commonly found in compressed air cleaners for keyboards and electronics. Chronic DFE inhalation can lead to toxicities such as acute kidney injury, hepatotoxicity, neurologic deficits, and cardiotoxicity.1 A rare consequence of chronic fluorinated hydrocarbon inhalation is a metabolic bone disorder known as skeletal fluorosis, which is characterized by osteosclerosis of the axial skeletal system, formation of osteophytes at joints and distal extremities, and ligament ossification.2 We present a case of skeletal fluorosis that developed within four months of chronic DFE inhalant use.
CASE REPORT
A 46-year-old female with a past medical history of anxiety, depression, and tobacco use presented to the emergency department (ED) with complaints of diffuse body swelling for approximately four months. She described pain in various joints that coincided with new-onset upper and lower extremity swelling. Three weeks prior, the patient had been evaluated at a separate ED and was diagnosed with skeletal fluorosis related to inhalation of compressed air cleaner for computer dust. She reported daily inhalant use of the cleaner for the previous four months, which she ceased using following her diagnosis at the outside hospital weeks prior.
Initial vital signs were heart rate 75 beats per minute, blood pressure 144/82 millimeters of mercury, temperature 98.6 ºFahrenheit, and oxygen saturation 100% on room air. Physical examination was remarkable for diffuse swelling to the bilateral upper and lower extremities, with right lower extremity swelling greater than that of the left lower extremity, interphalangeal joint swelling in bilateral hands (Image 1), and multiple non-mobile lesions on bilateral hands and left forearm (Image 2). Initial laboratory values from complete blood count, basic metabolic panel, and hepatic function panel were remarkable only for elevated alkaline phosphatase of 442 units per liter (L) (reference range: 44–147 units/L). Electrocardiogram showed sinus rhythm without evidence of ischemia.
CPC-EM Capsule What do we already know about this clinical entity?Skeletal fluorosis is a complication of excess fluoride which may be associated with chronic inhalation or “huffing” of compressed air cleaners.What makes this presentation of disease reportable?We present an uncommon and clinically noteworthy case of non-endemic skeletal fluorosis characterized by unique radiographic findings.What is the major learning point?Skeletal fluorosis is a rare and painful condition, which can have prolonged adverse effects and a lasting impact on quality of life.How might this improve emergency medicine practice?Increased awareness improves early recognition of skeletal fluorosis and emphasizes the importance of appropriate counseling on the risks of inhalant abuse.
Radiography revealed diffuse periosteal reaction throughout the hand (Image 1) and forearm (Image 2) suggestive of fluorosis. Chest radiograph and Doppler ultrasound of the right lower extremity showed no acute findings. Patient history, physical examination, and imaging results were highly consistent with a diagnosis of skeletal fluorosis. The patient was advised to continue to abstain from inhalant use and was scheduled for outpatient follow-up for continued monitoring and pain management.
At follow-up approximately two weeks later, she reported no improvement in symptoms since the ED visit. Pain in ankles, knees, and hands was described as sharp and constant, aggravated by movement and palpation and alleviated by rest, heat therapy, and pain medication. Swelling persisted to upper and lower extremities, which reportedly improved with rest. She was prescribed celecoxib for pain management and referred to rheumatology for elevated inflammatory markers and long-term management of skeletal fluorosis.
DISCUSSION
Skeletal fluorosis from inhalant abuse occurs when DFE is metabolized to free fluoride ions, which replace the hydroxyl ions in hydroxyapatite, converting it to fluorapatite in the bone.2 This leads to decreased bone turnover with increased osteoblast activity and greater resistance to breakdown by parathyroid hormone.2–3 Bones and bony protrusions become more brittle and susceptible to fracture, despite an overall normal or increased bone mineral density (BMD).4 Clinical manifestations of skeletal fluorosis may initially include joint and back pain or stiffness, eventually leading to loss of mobility and range of motion.2 Osteosclerosis, osteophytosis, and ligament ossifications are hallmark findings on skeletal fluorosis imaging.2 Furthermore, patients may develop secondary hyperparathyroidism with vitamin D and C deficiencies, which can be supplemented in treatment. Additional supplementation with vitamin E and methionine may also be considered to reduce skeletal fluoride accumulation.5
Skeletal fluorosis has historically been considered an endemic condition, occurring primarily in areas with fluorinated well water contaminated from nearby volcanic rock or industrial sources, and developing in patients over decades of exposure.2 Other causes of skeletal fluorosis have included exorbitant and chronic ingestions of fluorinated products such as teas made from Camellia sensis, toothpastes, mouthwashes, and drugs such as voriconazole.1,6 These non-endemic fluoride sources can have more rapid onset of the skeletal deformities and manifestations of fluorosis, developing over the course of months to years, likely due to higher fluoride concentrations.6
A review of non-endemic skeletal fluorosis case reports by Cook et al revealed that of patients with a known duration of use, five patients with tea exposures ingested anywhere from 14–74 mg of fluoride per day. These patients reported durations of use of anywhere from 17–37 years prior to initial presentation.7 One patient with an estimated daily toothpaste ingestion of 66 mg of fluoride presented after at least five years of exposure.7 In a systematic review of voriconazole-induced periostitis, it was found that skeletal symptoms developed after as little as six weeks to eight years of voriconazole treatment, with most reported voriconazole doses being 400 mg daily, an equivalent fluorine amount of 65 mg per day.8
Interestingly, inhalant use with DFE has also been linked with rapid onset of skeletal fluorosis in over a dozen cases (Table).1,3–7,9–14 Reports of use duration range anywhere from six months to five years in frequencies ranging from 2–7 cans weekly to 20–25 cans daily.5,9–10 Quantification of daily fluoride intake from DFE is difficult to determine due to varying product sizes and limited data on systemic absorption of the inhalant. Peicher et al and subsequently Chen et al estimated that exposure to 1–7 cans weekly for three years and 3–4 cans daily for 10–11 months resulted in total fluoride exposures of thousands of grams and approximately 147 kilograms, respectively.9,11
Our patient presented four months after initiation of daily DFE inhalation and described her symptom onset as coinciding around the same time. Her case emphasizes the potential for rapid development of skeletal fluorosis from daily DFE use and encourages suspicion of fluorosis in patients with a history of DFE inhalation and signs of skeletal pain, swelling, or deformities. Additional diagnoses to consider may include myelofibrosis, osteoblastic metastasis, renal osteodystrophy, ankylosing spondylitis, and Paget disease.2
Treatment of skeletal fluorosis is primarily supportive with physical therapy, minimizing fracture risk, and ceasing use of the offending product. In the case of abrupt DFE cessation, observation and benzodiazepines may be warranted for inhalant withdrawal.10 Once there is no further fluoride exposure, skeletal fluorosis improves slowly over the course of years due to the long skeletal fluoride half-life of seven years.2 Tucci et al described a 28-year-old male who had been huffing keyboard duster with DFE for about 3–4 years, with elevated urine and serum fluoride levels, progressive bony deformities on both hands, and loss of mobility in several joints. Three years after cessation of DFE, he had continued elevations in fluoride levels and BMD, with improvements in walking and mobility six months after a left hip arthrotomy for ankylosis, which included extensive osteochondroplasty of the femoral head and neck and prophylactic pinning of the femoral neck.6 Suwak et al described a 56-year-old male who had been huffing three cans of dust cleaner daily for about two years, in addition to previous occupational exposure to chlorofluorocarbon solvent cleaners. One year after he stopped huffing, the patient had decreased, although still elevated, serum fluoride levels, and he had continued bony protrusions on his digits and anterior tibia.12
Our patient had continued symptoms and pain after five weeks of DFE cessation, and reported alleviation of symptoms with rest, heat therapy and pain medication. Our case is limited by the lack of serum or urine fluoride concentrations. However, the patient presented to our ED three weeks after reportedly discontinued use, making serum concentrations less useful, except for confirming exposure. Additionally, radiologic examination, which is considered the best method of diagnosis, was highly consistent with the patient’s reported history and clinical course.
CONCLUSION
Skeletal fluorosis is a rare and painful condition that can have prolonged adverse effects and lasting impacts on quality of life. Patients presenting to the emergency department who report regular inhalant use should be counseled on the potential toxicities of these products and encouraged to cease use. Those presenting with diffuse skeletal findings and reported DFE use should be evaluated for skeletal fluorosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salles Rosa Neto N Englert D Mc Alister WH Periarticular calcifications containing giant pseudo-crystals of francolite in skeletal fluorosis from 1,1-difluoroethane “huffing.”Bone 20221601164213542965710.1016/j.bone.2022.116421 · doi ↗ · pubmed ↗
- 2Sellami M Riahi H Maatallah K Skeletal fluorosis: Don’t miss the diagnosis!Skeletal Radiol 2020493345573150195710.1007/s 00256-019-03302-0 · doi ↗ · pubmed ↗
- 3Ponce A Oakes JA Eggleston W Acute skeletal fluorosis in the setting of 1,1-difluoroethane abuse Clin Toxicol (Phila)201957537453044920210.1080/15563650.2018.1527034 · doi ↗ · pubmed ↗
- 4Mohideen H Dahiya DS Parsons D Skeletal fluorosis: a case of inhalant abuse leading to a diagnosis of colon cancer J Investig Med High Impact Case Rep 2022102324709622108491910.1177/23247096221084919 PMC 896609735343855 · doi ↗ · pubmed ↗
- 5Fikse DJ Le D Surmaitis RM Skeletal fluorosis secondary to harmful inhalant use Clin Toxicol (Phila)20226012137683642663510.1080/15563650.2022.2150634 · doi ↗ · pubmed ↗
- 6Tucci JR Whitford GM Mc Alister WH Skeletal fluorosis due to inhalation abuse of a difluoroethane-containing computer cleaner J Bone Miner Res 2017321188952744995810.1002/jbmr.2923 PMC 5977397 · doi ↗ · pubmed ↗
- 7Cook FJ Seagrove-Guffey M Mumm S Non-endemic skeletal fluorosis: causes and associated secondary hyperparathyroidism (case report and literature review)Bone 20211451158393341809910.1016/j.bone.2021.115839 PMC 8142331 · doi ↗ · pubmed ↗
- 8Adwan MH Voriconazole-induced periostitis: a new rheumatic disorder Clin Rheumatol 20173636096152737675410.1007/s 10067-016-3341-7 · doi ↗ · pubmed ↗