Multimodal imaging in a case of quadricuspid aortic valve regurgitation and stenosis: diagnostic challenges before transfemoral aortic valve replacement implantation
Louise Sakowski, Vladyslav Kavalerchyk

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
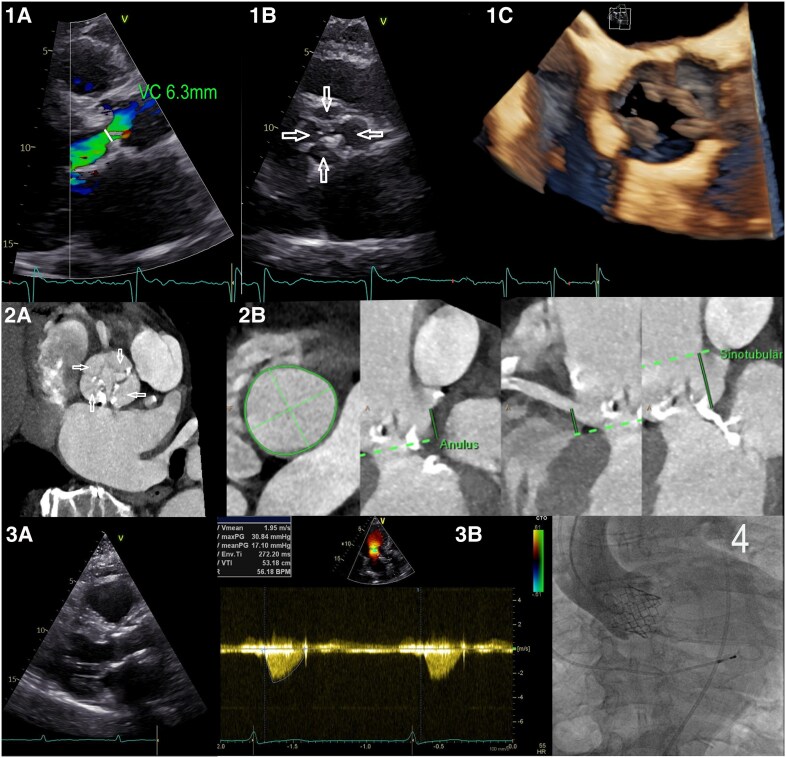 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Cardiac Imaging and Diagnostics
An 83-year-old patient was evaluated for a transfemoral aortic valve replacement (TAVR) due to severe aortic valve regurgitation and stenosis. The patient exhibited shortness of breath (New York Heart Association class III) and dizziness but denied chest pain, syncope, fever, or chills. Clinical examination revealed a crescendo–decrescendo systolic murmur most audible over the right second intercostal space. Electrocardiogram studies showed atrial fibrillation and left axis deviation. The initial pre-procedural transthoracic echocardiogram showed a quadricuspid aortic valve with severe aortic stenosis and severe aortic valve regurgitation (Figure 1A and 1B). However, transoesophageal echocardiogram, while confirming severe aortic stenosis and regurgitation, could only identify a tricuspid aortic valve, creating uncertainty about the number of leaflets (Figure 1C). To confirm the presence of a quadricuspid valve and ensure accurate sizing for the TAVR prosthesis, a cardiac computed tomography (CT) scan was performed (Figure 2A and 2B). The CT scan demonstrated a severely calcified quadricuspid aortic valve, classified as Hurwitz and Roberts class A with four equal leaflets. The patient underwent TAVR with a 26 mm Edwards prosthesis (Figure 4). During the procedure, the patient required electrocardioversion twice due to peri-procedural tachyarrhythmias. Otherwise, the procedure was unremarkable. Post-procedural echocardiography confirmed the proper placement of the Edwards valve without any paravalvular leakage (Figure 3A and 3B). The patient experienced no complications and was discharged home 4 days after the procedure.
Consent: Informed consent was achieved from the patient in written and oral form to write this case study.
Funding: This research was not supported by any sponsor or funder.
Data availability: No new data were generated or analysed in support of this research.
Lead author biography
Dr Vladyslav Kavalerchyk is an experienced physician specializing in functional diagnostics at the Helios Kliniken Schwerin, with extensive expertise in echocardiography. He leads the echocardiography lab since 2017 and holds advanced qualifications in transthoracic, transoesophageal, stress, and contrast echocardiography. As a member of the EACVI Web & Communication Committee and a certified trainer (DEGUM II), he plays an active role in advancing echocardiographic education and clinical research.