The Incidence of Stroke Mimics in the Emergency Department of a Tertiary-care Center in Lebanon
Hind Anan, Maya Bizri, Mustapha Jomaa, Nour Ibrahim, Afif Mufarrij

TL;DR
This study finds that nearly half of patients presenting with stroke-like symptoms in a Lebanese hospital are not having a real stroke, highlighting the need for better triage methods.
Contribution
The study provides a detailed analysis of stroke mimic incidence and etiologies in a Lebanese tertiary-care center, identifying key risk factors.
Findings
40.2% of stroke code activations were for stroke mimics rather than true strokes.
Medical etiologies accounted for 87.2% of stroke mimics, with neurological causes being the most common.
Neurological or psychiatric history and altered mental status increased the likelihood of stroke mimics.
Abstract
Stroke mimics comprise a significant proportion of cases presenting with neurological deficits and can be difficult to differentiate from true stroke cases. Our aim in this study was to assess the frequency and etiologies of stroke mimics presenting to our emergency department (ED). We conducted a retrospective review of the charts of patients presenting to the ED of a tertiary-care center between November 2018–August 2023 and on whom the stroke code was activated. The cases were categorized into real strokes or stroke mimics based on patients’ discharge diagnoses. Stroke code activation was implemented on 584 patients during the study period. These patients received full service and a final discharge diagnosis. Of these, 349 (59.8%) received a diagnosis of a true stroke, whether ischemic, hemorrhagic, or transient ischemic attack. The remaining 235 (40.2%) were classified as stroke…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
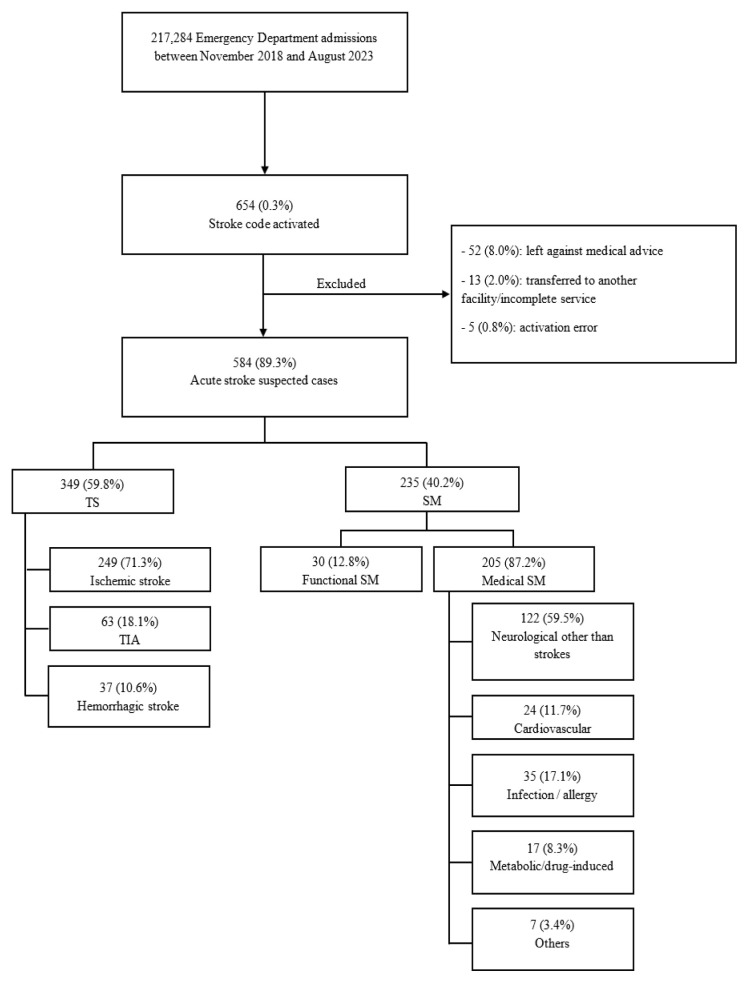 Figure 1
Figure 1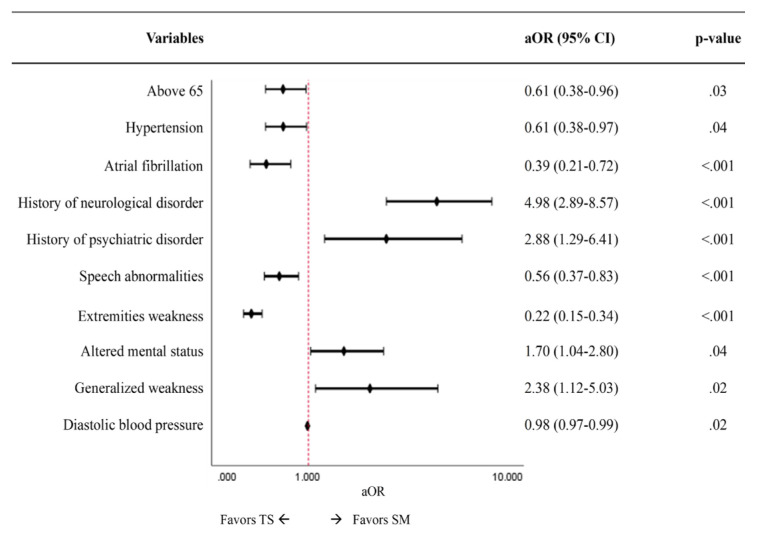 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Intracerebral and Subarachnoid Hemorrhage Research · Cerebral Venous Sinus Thrombosis
INTRODUCTION
In 2019, stroke was the second leading cause of death globally, accounting for 11.6% of deaths annually.1 Given the high rate of mortality and disability, it is essential to investigate and treat any presenting stroke patient in a timely manner. This requires a host of diagnostic tests and, possibly, subsequent thrombolytic treatment. The costs add up to further stress an already burdened healthcare system. Globally, there is one new stroke every three seconds, leading to a worldwide cost exceeding 1% of the global gross domestic product.2 This high burden makes it crucial to distinguish a stroke from any similar mimic. Stroke mimics (SM) are defined as stroke-like symptoms and presentations that arise due to a non-cerebrovascular etiology.3 Such mimics are estimated to make up an average of 22% of all stroke presentations, ranging from 1–64% of all suspected stroke cases.4
Stroke mimics have a wide range of etiologies, with seizures, migraines, and functional disorders making up more than 40% of the cases.5,6 Other causes include cerebrovascular narrowing, toxic or metabolic origins, brain trauma and subdural hematoma, infection, and cardiovascular and other neurologic disorders.5 Patients experiencing stroke mimics exhibit different characteristics from those experiencing an actual stroke. These include differences in age, gender, comorbidities, and presenting signs and symptoms.7–14
An improper identification of an SM can subject a patient to a myriad of diagnostic tests and imaging, and potentially to an unnecessary thrombolytic treatment. It is estimated that between 1–16% of SM patients receive thrombolysis with tissue plasminogen activator (tPA), with 0.5% of these patients developing a symptomatic intracerebral hemorrhage.15 Such unnecessary interventions can add up, with an estimated cost of treatment of $5,400 per admission.16 These factors necessitate the early identification of an SM patient to spare the unwarranted tests and interventions.
Stroke is also a leading cause of mortality in Lebanon, with 3.1% of total deaths in 2021 attributed to cerebrovascular incidents.17 The prevalence of stroke was estimated to be 0.5%18, with an average cost of US $6,961 per stroke patient.19 Moreover, a survey of Lebanese people above the age of 40 indicated that 12.1% had experienced at least one stroke symptom.20 Data on the incidence of SMs in Lebanon is scarce. This study aimed to assess the incidence of stroke presentations to a local emergency department (ED) and explore the subsequent diagnoses related to SMs. We looked at patient characteristics, tests and interventions performed, and final diagnoses upon discharge.
METHODS
Study Design and Sample
This was a retrospective, descriptive study of adult patients presenting to the ED of a tertiary-care center in Lebanon. We reviewed the records of all adult patients aged ≥18 years on whom the stroke code was activated upon presentation to our ED between November 2018–August 2023. In our facility, the stroke code is typically activated after the initial assessment of the patient upon arrival. The activation is triggered either directly by the senior attending in the ED or after confirmation with them.
The study was approved by our institutional review board (BIO-2020-0293) and followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
Population Health Research CapsuleWhat do we already know about this issue?A significant proportion of individuals presenting with stroke-like symptoms are ultimately diagnosed with a stroke mimic rather than true stroke.What was the research question? What are the frequency and etiologies of stroke mimics presenting to our tertiary-care center emergency department? What was the major finding of the study?Among 584 patients, 235 (40.2%) received a diagnosis of stroke mimic with functional (12.8%) or medical (87.2%) etiologies.How does this improve population health?The study highlights the need for a more specific screening pathway for stroke-code activation to reduce strain on an already burdened healthcare system.
Data Collection and Variables Measured
Patients were identified using the administrative data of all stroke code activations during the study period. Patients who left against medical advice or were transferred to another hospital before a diagnosis could be made were excluded from the analysis. All study data were extracted manually from the electronic health record (EHR) (Epic Systems Corporation, Verona, WI). Data abstractors, who had prior training in using the EHR for clinical purposes, were not blinded to the study hypothesis.
The data collection protocol was standardized, with variables defined prior to the analysis. Collected variables included patient demographics and characteristics, vital signs upon presentation to the ED, presenting symptoms, imaging studies performed, thrombolysis interventions given, disposition, and discharge diagnoses. We reported missing variables as “unknown.”
Diagnoses
We used the International Classification of Diseases, 10*^th^** Rev*, Clinical Modification (ICD-10-CM) coded diagnoses to classify patients into nine categories: ischemic stroke; hemorrhagic stroke; transient ischemic attack (TIA); functional disorders; neurological disorders other than cerebrovascular accidents; infections or allergic reactions; cardiovascular; metabolic or drug-induced; and diagnoses not elsewhere classified. True strokes were defined as TIA, ischemic stroke, or hemorrhagic stroke confirmed on brain imaging. The six remaining categories were classified under SMs.
Medical Record Review Studies Criteria
This study followed recommended practices for retrospective chart reviews, as described by Worster et al.21 Details of individual method criteria followed are described in Table 1.
Statistical Analysis
We performed statistical analysis using SPSS Statistics v28.0 (IBM Corp, Armonk, NY). Significance was set at an alpha of 0.05. We presented categorical variables as percentages and frequencies, while continuous variables were expressed as means ± standard deviation or median and interquartile range (IQR). We used chi-squared and Fisher’s exact tests to compare groups of categorical variables, and the t-test and Mann-Whitney U tests to compare the differences in numerical variables. A multivariable logistic regression model was constructed to determine independent factors associated with SMs. Variables were included in the model if they were clinically relevant or found to be significant on bivariate analysis.
RESULTS
Over a 58-month period, 654 patients presented to our ED and had a stroke code activation. Of these, 70 (10.7%) patients either left against medical advice or were transferred to another facility after being deemed stable and having received incomplete service. Patients who did not have a definitive diagnosis were excluded from the analysis. Of the 584 patients who had a known diagnosis at discharge, 349 (59.8%) had a true stroke, 249 (71.3%) were diagnosed with ischemic stroke, 37 (10.6%) with hemorrhagic stroke, and 63 (18.1%) with TIA.
The remaining 235 (40.2%) were diagnosed with a stroke mimic. Of those, 30 (12.8%) had a functional SM (ie, a psychiatric etiology of their symptoms), while 205 (87.2%) had a medical SM (non-cerebrovascular, non-psychiatric origin of symptoms. Neurological disorders other than strokes were the most common presentation (59.5%) in the medical SM, and seizures were the most common presentation, comprising 27.0% of neurological SM and 14.0% of all SM (Figure 1).
Table 2 shows the demographics and ED visit characteristics of the identified patients. Stroke patients were significantly older than stroke-mimic patients (70.6 [±13.5] years vs 64.7 [±16.0], respectively; P = .001). There was no significant difference in gender, marital, or smoking status between the two groups. Stroke patients were more likely to have hypertension (72.5% vs 61.3%; P = .004), coronary artery disease (31.8% vs 18.7%; P = .001), atrial fibrillation (23.5% vs 8.5%; P < .001), and previous ischemic stroke (21.0% vs 10.6%; P = .001). On the other hand, a history of psychiatric (11.5% vs 4.3%; P = .001) and neurological disorders (29.8% vs 9.7%; P < .001) was more common in SM patients. Of the 122 patients with neurological etiology of SM, 51 (41.8%) had a known past neurological history, and of the 30 patients with psychiatric etiology, only seven (23.3%) were known to have a past psychiatric history.
The time elapsed between patient arrival at the ED and the activation of the stroke code varied significantly between the stroke and stroke-mimic groups. Stroke patients had a shorter time from arrival to activation (median of 7.5 [IQR 8.5 minutes]) compared to SM patients (median of 11 [IQR 15 minutes], P < .001). Almost all patients (99.3%) who presented to the ED received brain imaging during the visit.
Stroke-mimic patients were less likely to have computed tomography angiography (CTA) (42.1% vs 57%; P < .001) and magnetic resonance angiography (MRA) (20.4% vs 39.3%; P < .001). Thirty-three patients (5.7%) received thrombolysis with recombinant tPA, one of whom had a stroke mimic (Table 2). Table 3 shows the patients’ vital signs and symptoms upon ED presentation. Stroke patients presented more with speech abnormalities (64.8% vs. 49.4; P< .001), extremities weakness (63% vs 29.8%; P < .001), or facial weakness (30.7% vs. 19.1%; P = .002). They were also found to have significantly higher mean systolic (151.8 ± 26.3 vs 144.0 ± 27.4; P = .001).
DISCUSSION
To the best of our knowledge, this study is the first to describe the rate and characteristics of stroke mimics in Lebanon. Roughly half of our patients (40.2%) were found to have SM. Roughly half of our patients (40.2%) were found to have SM. This incidence of mimics is more than double the reported global average of 22%4 and is higher than the reported figures in regional studies from Qatar (35%)22 and Morocco (15.6%).23 Conversely, our findings are similar to those reported in a study from Canada (43.2%).24 With no prior data on the incidence of SMs in other local hospitals, it is difficult to pinpoint the origin of our high rate and to comment on the sensitivity of our stroke code-activation practices. Several studies have proposed an algorithm for the early detection of a mimic25,26; however, in the absence of a standardized and validated mimic identification model, the activation of the stroke code must rely on the judgment of the triage team and the internal protocol set by each medical care facility. Of the 235 SM patients, 122 (51.9%) had a non-cerebrovascular neurologic origin. Seizures, as a single disease diagnosis, were the most common presentation for SMs. This mirrors globally reported trends, which state that seizures cause most SM cases.3,6 Nevertheless, global incidence accounts for an average of 20% of said cases5,10 as compared to 14.0% in our study. The lower number of seizure disorders presenting as a stroke to our ED could be due to an early identification of neurologic comorbidities at the triage level, prompting the treatment of the patient as a regular neurologic case rather than a potential stroke case. A patient presenting in the postictal phase could be accompanied by a chaperone who witnessed the seizure, which decreases the likelihood of a stroke diagnosis.
Our data revealed that 30 patients (12.8%) had functional SM. This incidence was similar to that found in the United Kingdom (13%)27 and Canada (11.9%),28 lower than that found in France (16.7%)29 and Saudi Arabia (24.4%)7, and higher than that found in Korea (5.6%)10 and Iran (8.1%).30 Cultural distinctions and variations in illness manifestation behaviors across countries could account for these differences. This is substantiated by data from Qatar initially showing a 17% incidence of functional SM.31 However, when including all nationalities presenting to the same center, this incidence increased to 29.2%.31 Interestingly, our incidence paralleled that from SM studies in other EDs (11.9%, 8.1%, 5.6%)10,28,30 as opposed to studies conducted in stroke centers where psychiatric disorders were identified as one of the highest proportions of all causes of mimics (29.2%, 25.7%, 24.4%).7,23,31 This discrepancy may be explained by the fact that the primary assessors in the former studies were neurologists, while those in the latter studies, including ours, were emergency physicians. The more diversified exposure to psychiatric cases during emergency medicine training may be related to the lesser percentage observed. It may also be skewed by self-selection bias, whereby functional patients, exhibiting stroke symptoms, would be more likely to present to a stroke center rather than to an ED.
Several clinical features were found to be associated with SM in our sample. Age <65 years was independently associated with SM. This is in line with the published literature on younger individuals being more likely to have SM.10,12–14 This is also expected, considering that 75% of all strokes occur in persons ≥65 years of age.11 Past medical history and presenting symptoms were also consistent with prior studies in terms of risk factors. A history of hypertension or atrial fibrillation, or motor deficits such as extremity weakness or speech disturbances favored a TS diagnosis.9,10,15,32,33
In contrast, a history of psychiatric or neurological disease or an altered mental status presentation increased the odds of a SM diagnosis.10,15 Specifically, in our dataset, a history of neurological diseases other than stroke strongly favored SM diagnoses. This can be explained by the fact that individuals with a history of seizures can present in a postictal state, mimicking strokes.15,34 Seizures are one of the most common SM presentations in both our data and in the literature.34,35 Additionally, previously published studies have shown that migraines, especially those with aura or hemiplegic migraines, are one of the leading SM presentations, and having a history of migraines increases the likelihood of an SM diagnosis compared to a TS. Furthermore, due to increased intracranial pressure or mass effect, patients with brain lesions can present with neurological deficits like those seen in strokes, despite the absence of any vascular event.5,36
The results obtained in our study suggest the need for a more specific algorithm for activating a stroke code. This could include the involvement of more physicians and personnel with exposure to neurologic and psychiatric training in the triage of suspected stroke cases and the subsequent activation of the stroke code. Our data also highlight the need for more studies on the incidence of SMs in various medical care facilities across Lebanon. A local average stroke-mimic rate would allow for a better evaluation of the specificity and efficiency of the stroke code system in hospitals nationwide.
LIMITATIONS
The study is limited to patients presenting to the ED of a single, tertiary-care center in Lebanon. This limits the generalizability of the results we reported and may not reflect the true rate of SMs in the country. The lack of data from other local hospitals makes it difficult to compare our results to other care centers, thus diminishing the ability to accurately describe the incidence of SMs as well as the sensitivity of our stroke code-activation system. In addition, the total number of patients treated with r-tPA was low, making it difficult to truly evaluate the negative outcomes of misidentifying and wrongly treating SM cases.?
Moreover, this study has methodological limitations common to retrospective reviews. The data were examined retrospectively, and the diagnoses at discharge were extracted as ICD-10-CM codes from the charts of identified patients. The diagnoses may have been classified and labeled incorrectly, making some etiologies over- or under-represented. Also, not all Worster et al criteria for retrospective chart reviews were followed.21 Specifically, the performance of data abstractors was not formally monitored, they were not blinded to the study objectives, and data extraction was conducted once; thus, interobserver reliability was not formally tested or reported, which may have introduced bias. However, to reduce this risk, we used a structured data abstraction form with predefined variables to ensure consistency. Additionally, all data abstractors were medically trained and had extensive prior experience with the database, which contributed to the consistency and accuracy of data entry.
CONCLUSION
Given that stroke is a time-dependent medical emergency, it is imperative that emergency physicians rule out acute stroke first. However, given that nearly half of the presenting cases received a diagnosis of stroke mimic, it is imperative to devise a more specific screening pathway for stroke code activation. In low- and middle-income countries, specifically Lebanon, unwarranted code activations overburden the fragile healthcare system, which already suffers from limited capacities characterized by insufficient staff, equipment, and medications. Thus, a step forward toward developing a psychometrically robust and culturally adapted assessment for stroke mimics may help physicians in triaging suspected patients and considering alternative diagnoses.
Supplementary Information
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Neurol 202120107958203448772110.1016/S 1474-4422(21)00252-0PMC 8443449 · doi ↗ · pubmed ↗
- 2Feigin VL Brainin M Norrving B World Stroke Organization (WSO): Global Stroke Fact Sheet 2022 Int J Stroke 202217118293498672710.1177/17474930211065917 · doi ↗ · pubmed ↗
- 3Huff JS Stroke mimics and chameleons Emerg Med Clin North Am 2002203583951237996210.1016/s 0733-8627(02)00012-3 · doi ↗ · pubmed ↗
- 4Mc Clelland G Rodgers H Flynn D The frequency, characteristics and aetiology of stroke mimic presentations: a narrative review Eur J Emerg Med Off 20192612810.1097/MEJ.000000000000055029727304 · doi ↗ · pubmed ↗
- 5Long B Koyfman A Clinical mimics: an emergency medicine-focused review of stroke mimics J Emerg Med 2017522176832778065310.1016/j.jemermed.2016.09.021 · doi ↗ · pubmed ↗
- 6Nor AM Ford GA Misdiagnosis of stroke Expert Rev Neurother 20077898910011767849410.1586/14737175.7.8.989 · doi ↗ · pubmed ↗
- 7Al Khathaami AM Alsaif SA Al Bdah BA Stroke mimics: clinical characteristics and outcome Neurosciences (Riyadh)202025138423198289310.17712/nsj.2020.1.20190096 PMC 8015631 · doi ↗ · pubmed ↗
- 8Olindo S Chardonnet M Renou P Clinical predictors of stroke mimics in patients treated with recombinant tissue plasminogen activator according to a normal multimodal computed tomography imaging J Stroke Cerebrovasc Dis 201827245492912832710.1016/j.jstrokecerebrovasdis.2017.09.024 · doi ↗ · pubmed ↗