Emergency Medicine Scholarly Tracks: A Mixed- methods Study of Faculty and Resident Experiences
Jason Rotoli, Ryan Bodkin, Grace VanGorder, Valerie Lou, Lindsey Picard, Beau Abar

TL;DR
This study explores how emergency medicine scholarly tracks affect faculty and residents, finding positive impacts on mentorship and career development with few barriers.
Contribution
The study provides new insights into the impact of emergency medicine scholarly tracks on mentorship and career outcomes, highlighting benefits and challenges.
Findings
Most participants reported a positive impact on mentorship from scholarly tracks.
The most common reason for track selection was interest in a clinical area.
Faculty noted increased one-on-one time with residents and specialization opportunities.
Abstract
Emergency medicine (EM) scholarly tracks have been adopted for increased subspecialty exposure and training. However, current literature fails to elucidate the impact on faculty and resident careers and resident and faculty engagement opportunities or demonstrate barriers to continuation. The purpose of this study was to evaluate the perceived impact of EM scholarly tracks on participating faculty (eg, resident interaction/mentorship, career satisfaction, perceived barriers to implementation) and recent graduates (eg, faculty mentorship, reasons for track selection, perceived barriers to continuation). This mixed-methods study includes a cross-sectional quantitative survey with 30 EM residents (who graduated between 2021–2023) and semi-structured, one-hour qualitative interviews with six faculty in a large, tertiary-care academic medical center with a university-based hospital and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
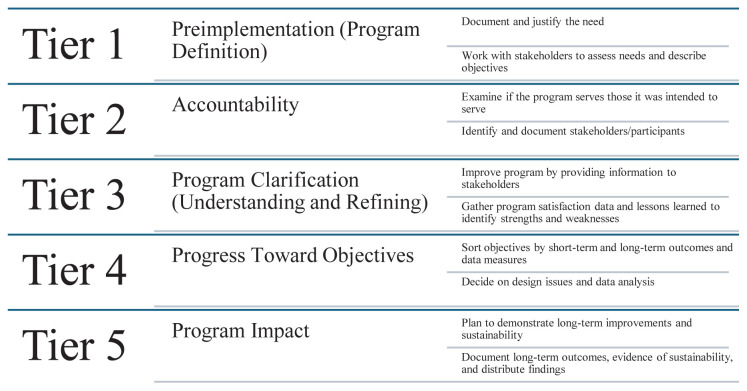 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiology practices and education · Primary Care and Health Outcomes · Healthcare Systems and Technology
INTRODUCTION
Since emergency medicine (EM) was approved as a primary medical specialty by the American Board of Medical Specialties in 1989, opportunities for subspecialty training have gradually increased. Currently, there are seven fellowships recognized by the Accreditation Council for Graduate Medical Education (ACGME), 11 fellowships recognized by the American Board of Emergency Medicine (ABEM) (Table 1), and many more non-ACGME/ABEM fellowship training opportunities available to emergency physicians under other board specialties.1–3 In 2017, a survey of US EM program directors found that approximately 40% of EM residency programs had subspecialty tracks available to trainees.4 Track format varied widely, including required didactics, experiential learning models, and longitudinal electives.
Population Health Research CapsuleWhat do we already know about this issue?Data show the benefits of subspecialty tracks, but no study has looked at the perceived benefits for both residents and faculty on a more granular level.What was the research question?We evaluated the perceived impact of tracks on participating faculty and recent EM graduates.What was the major finding of the study?Subjects mostly pursued either an academic or hybrid academic/commmunity care career (18/30) and most reported a positive impact on scholarly tract mentorhip (25/30).How does this improve population health?Scholarly tracks can lead to enhanced career satisfaction for both EM faculty and residency graduates, which in turn could result in better care for their patients.
A few studies have assessed the efficacy of EM track-based education and the association with residents’ interest in fellowships.5–8 Scholarly track-based learning is associated with pursuing a career in academic EM, and residencies often integrate tracks to enhance career guidance by inspiring residents to choose academic careers.7 However, most of the studies that have looked at the benefits of tracks, such as faculty development and mentorship, are anecdotal and based on consensus literature from program director surveys. Research that directly assesses the perceived impact on participating EM residents and faculty is sparse.7,9 Additionally, while some research describes best practices when implementing EM tracks and suggests why tracks may not exist (ie, lack of time, lack of faculty, limited administrative support), little research has investigated barriers to the continuation of EM subspecialty tracks after they have been established.4,9 We aimed to evaluate how participating faculty members and recently graduated residents perceived track-based education. Given the benefits of robust mentorship for EM residents and faculty (eg, career success, professional growth, academic productivity, and opportunity to give back to the profession), we hypothesized that academic faculty and residents would report improved engagement (mentorship) opportunities and enhanced career satisfaction.10,11 Additionally, we investigated EM residents’ perceived barriers to track continuation.
METHODS
Study Design and Survey
We conducted this mixed-methods study, comprised of a cross-sectional quantitative survey of 30 EM graduates and semi-structured qualitative interviews with six faculty at an academic medical center in the northeastern US with a university-based hospital, a medical school, and >100,000 annual ED patient visits. We defined a career in academics as working in a medical center with a university-based hospital, university ownership/affiliation, and/or an affiliated medical school. Alternatively, we defined a career in community EM as working in a hospital with limited (or no) relationship with a university/medical school and with a limited numbers of (or no) learners. A hybrid career was defined as working any amount of time in both academic and community settings. Our department has a three-year, ACGME-accredited program with 14 residents per class, seven fellowships with 8–10 fellows per year, and approximately 80 faculty members.
We developed quantitative and qualitative survey questions using the process of iteration and literature review for research gaps, and by harnessing the research team’s academic experience and experience with national grant funding, EM fellowship training (medical education), and residency administration. The team consisted of one medical student interviewer, two junior academic faculty, two senior academic faculty, and one research methodologist. Collectively, and through an iterative process, we capitalized on team expertise to design the survey, which we refined and subsequently pre-tested for errors and comprehension. While we did not formally assess construct validity, the survey was reviewed by an external content expert and the study team for face validity.12 Although less widely accepted than construct validity, face validity is a complex paradigm used to evaluate how respondents perceive test items. It consists of many dimensions, including accuracy, acceptance (likeability) and relevance, and has been regarded as an acceptable form of validity in prior medical education curricula.13–15
We collected and managed survey data using Research Electronic Data Capture (REDCap) tools hosted at the University of Rochester. The survey questions sent via email to EM graduates included demographics (age, graduation year, completion of fellowship, career selection), critical review of track implementation (reasons for track selection, timing, barriers), and training impact (mentorship opportunities). They answered questions using a three-point Likert scale with a “strongly negative,” “neutral,” or “strongly positive” response (see Appendix A). The faculty data came from one-hour, semi-structured interviews conducted by a third-party person trained by a research team member. The faculty interviews targeted four areas: 1) demographics (additional degrees, years at the institution, scholarly track role such as director, creator); 2) resident interaction (opportunities for mentorship, engagement, and non-clinical evaluation); 3) impact on career (longevity, trajectory, opportunities for scholarly work); and 4) barriers to track perpetuation (See Appendix B).
Faculty were interviewed using a program evaluation framework, seeking evidence of common and distinctive feedback to improve the experience of the tracks program. We designed the interview questions to address tier 3 (understanding and refining the program), tier 4 (continuing progress toward desired outcomes), and tier 5 (broad program impact) of the five-tiered approach to program evaluation (Figure).16 To maintain anonymity in feedback, interviews were not recorded or transcribed. Instead, the interviewer took notes on faculty responses, requesting confirmation from participants when summarizing or quoting. To further maintain confidentiality we did not collect faculty-associated tracks.
Recruitment, Consent, and Risk to Subjects
Resident Selection and Recruitment
Since our track learning began in 2019, inclusion for the study included any residents who graduated between 2021–2023. Exclusion criterion was any resident who did not graduate within this period. Eligible participants were emailed information detailing the project’s objectives. Participation was voluntary. The email contained a link to the REDCap survey. All data collection was anonymous. Completion of the survey implied consent. We sent a reminder email two weeks after the initial email to maximize participation.
Faculty Selection and Recruitment
Inclusion for the study included any faculty deemed a scholarly track leader or creator. We excluded faculty who did not lead or create a scholarly track. Our goal was to obtain a representative sample with respect to tracks supervised, stage of academic career, and faculty sex. We emailed eligible faculty an information sheet that detailed the project’s objectives and emphasized that participation was voluntary. We sent reminder emails two weeks and four weeks after the initial email. Interview scheduling and completion implied consent.
There were no sex, race, or ethnicity-based restrictions. This project was undertaken as a quality improvement initiative. Per the University of Rochester’s Guideline for Determining Human Subject Research, it did not meet the definition of research according to 45CFR46 and was exempt from institutional review board-approval. Data were anonymous for all participants, and there was minimal risk to participant confidentiality.
Track Structure
The tracks start at the beginning of postgraduate year (PGY)-2 year and culminate at the end of the PGY-3 year. The sessions, 60–90 minutes long, take place during didactic conference 9–10 times per academic year. Tracks are led by 1–3 faculty members and have a maximum of 1:3 faculty-to-resident ratio. Track curricula are 18–20 months long and incorporate required elements that are the same across all tracks, including basic research certification training, a medical student- or peer-teaching requirement, and choosing a research question. Other required elements are unique to each specific track, including didactics, journal clubs, community engagement (eg, partnering with local shelters to organize an activity), track-specific certifications (eg, advanced research training), or hands-on activities (eg, joining a Wilderness Medicine Society or local- event medicine). Similarly, the requirements for track completion vary based on the chosen subspecialty but with some overlap for all tracks (eg, teaching component and research projects). Given the intensity of the PGY-2 year in a three-year training program, residency leadership backloaded many of the requirement due dates to the end of PGY-2 and early/mid PGY-3 year. For residents who have any interests outside existing tracks, the “Education Track” empowers them to pursue these interests.
Analysis
We conducted frequency analysis on resident demographics, mentorship impact, timing of tracks, most common track choice, and implementation barriers. Chi-square analyses were used to compare reasons for resident track selection. The initial evaluation of faculty interviews was conducted by a non-clinical, research faculty team member (BA) in a program evaluation framework, seeking commonalities and distinctive experiences that might inform track revision. It has been reported that using deductive and inductive analytic practices provides the deductive tools to organize the data, allows findings to emerge from the data, and applies existing knowledge and theory to interpret and explain findings.17 We used inductive coding and constant comparative analysis, which enabled us to analyze the responses to discover common themes among the data.18,19 Due to limited numbers of participants, data were insufficient for more robust analysis methods, such as grounded theory analysis.
RESULTS
Resident Data
The response rate for the resident survey was 71% (30/42). Most participants were male (19/30) (corresponding to the demographics of the sample pool of residents), between 30–34 years of age (23/30), and had either academic or hybrid (academic/community) careers (18/30). A minority of participants had purely academic EM jobs (6/30) and one third (10/30) of all graduates had either completed or were completing a fellowship, with ultrasound the most common (4/10).
Eighty-three percent (25/30) of participants reported a positive impact on mentorship during residency. The most common reason for track selection was “area of clinical interest” (93% report this reason as “very important” (overall chi-square and each subsequent pairwise comparison <.001)). Most residents did not report barriers to track implementation and continuation, with only one third of residents (10/29) reporting that COVID-19 interfered with scholarly track implementation. (Table 2 lists complete results.)
Faculty Data
The response rate for the faculty interview was 75% (6/8). Most faculty members frequently discussed how the implementation of tracks led to increased one-to-one faculty-resident time and engagement with residents and provided opportunities to guide and observe resident skill development outside the clinical arena. One faculty member commented how faculty can use “[track] relationships to form new, deeper connections— to see a different way of [resident] thinking.” Three faculty members discussed the opportunity that tracks provide for education in hands-on skills that are difficult to teach in large group settings, particularly to learners who are not particularly interested in the area of instruction (Table 3). Additionally, faculty favorably reported that tracks offered the opportunity for some specialization for non-fellowship seeking residents. For example, one faculty member noted, “[tracks] allow teachers to talk more about a specific advanced topic of interest and provide enthusiastic residents with a focused learning curriculum outside of the group setting.” Shared and distinctive themes and supporting comments can be found in Table 3.
When discussing barriers to continuation, faculty suggested striking a balance between teaching too much to discourage interest and teaching enough to engage interested learners during a track meeting. There was no thematic saturation regarding the impact on faculty career longevity.
DISCUSSION
Among many factors in the complex decision of choosing a career, scholarly tracks have been associated with a higher likelihood of an academic career choice.8,20 Although not directly investigated in this study, most graduates in our study worked in academic or hybrid careers.5 Additionally, one-third of the participants entered or completed academic fellowships, consistent with Jordan et al’s reported percentages of track-trained residents entering fellowships in 2018.5 Both results are logical, as scholarly track training can inspire residents to choose fellowships, and fellowship-trained graduates may be more likely to look for jobs and are often sought out by academic institutions. As supported by a study by Jordan et al in 2024, track exposure is one of several factors that guide residents down their career paths as it increases exposure to and involvement with faculty scholarly work and mentorship.20
On the contrary, an older study from 2008 contradicts our findings, reporting only that 23% of residents accept academic jobs and 5% fellowship entry. This discrepancy may be due to the Lubavin study design; they included community- and academically-trained EM residents, with community-trained EM residents less likely to pursue academic EM careers. Additionally, the 16-year time difference between that study and ours reflects potentially more contemporary motivators to pursue academics, including more fellowship options and an increased emphasis on wellness through balance of clinical and academic (research, leadership, teaching, and mentorship) roles.8,21,22
Over 80% of our graduated residents noted the increased opportunities for mentorship. Given the excellent faculty-to-resident ratio, additional time for interaction, and shared passion for an academic interest, this is one of the most important aspects of track training. Although nearly all the previous EM program director literature has perceived this and it has been documented by participating residents in other specialties, to our knowledge this is the first study with direct feedback from EM residents who participated in tracks during residency.23,24
The most common reason for track choice was “area of clinical interest.” This is a logical finding, given the increased desire to learn from like-minded people with common interests and goals. The least common reason for track selection was “lowest effort/amount of work.” In an academic residency, this finding may be related to residents being more motivated to pursue scholarly work during their training. To our knowledge, these motivations have not been measured in participating EM residents until now.
Overall, most residents did not report barriers to track continuation. Given the structure of the tracks (eg, backloaded due dates to avoid adding to high-intensity training periods and dedicated time during didactics), there was minimal reported impact on clinical obligations or work-life balance. Additionally, resident participation and interest were not reported as barriers to track continuation. This may have been influenced by the program’s dedication and faculty interest in track implementation. Also, subspecialty tracks are not new, and we likely benefited from previously published literature on the perceived benefits, as well as pitfalls to avoid when creating tracks. To our knowledge, these have not been measured directly by participating EM residents until now.
Participating faculty had a favorable view of the impact of the subspecialty track on interaction with residents. The faculty reported increased time with residents and the potential to inspire and educate non-fellowship seeking residents. Although this study did not establish causality, this additional time and mentorship from participation in subspecialty tracks are consistent with current literature as two of the many factors that help guide graduates in their career-decision process and to stay focused on academic careers.20 Also, faculty used track sessions to observe non-clinical skill development, including time management, project execution, and communication. This allowed for a deeper understanding of the residents’ development, which fostered enhanced career guidance through more individualized coaching and mentorship. One reported barrier to the continuation of tracks was the need to establish a balance between teaching and “over-teaching” to keep learners engaged and cultivate curiosity but prevent them from feeling overwhelmed. Notably, overwhelming learners has been shown to reduce active learning/engagement and has proven to be time-consuming (and detrimental) for the instructor.25
LIMITATIONS
First, this study measured recently graduated EM resident perceptions of track impact over a limited period (three years) and did not measure impact directly. Additionally, we did not have access to comparative data from the three years preceding the establishment of tracks, making it insufficient to establish causation. Second, the study was conducted at a single academic institution, potentially limiting generalizability to smaller (or community) institutions without a robust core faculty with dedicated time for or expertise and interest in track implementation. Additionally, the lack of standardization of implementation and design of educational tracks across programs makes it difficult to generalize our results to other institutions. Also, single-center studies can overestimate effect in comparison to multicenter studies.26 Third, a limited set of faculty members provided qualitative feedback about the program, and a single research team member was responsible for collating responses in a program evaluation framework. Subsequent evaluation work might benefit from a larger faculty sample and the use of more extensive qualitative analysis methods (eg, transcription, grounded theory analysis).27
Fourth, pre-selection bias may have influenced our results as residency applicants who are interested in pursuing subspecialty fellowships may have initially chosen our residency program due to existing fellowships. Consequently, these trainees may have been more likely to positively review and participate in scholarly tracks. Fifth, self-selection bias may have influenced qualitative results, given that the faculty chosen to participate may have been more apt to favor the scholarly track work and highlight its benefits. It may have also influenced some of the resident data; specifically, the least common reason for choosing a track was “lowest effort/amount of work,” as recently graduated residents may not have wanted to be perceived as lazy or uninterested in learning during a study conducted by former colleagues/mentors. Lastly, non-response bias may have been present; it is important to acknowledge that any patterns uncovered in analyzing a non-random sample do not provide valid grounds for generalizing about a population.28,29
CONCLUSION
Recently graduated EM residents reported that scholarly tracks positively impacted mentorship. While this study did not assess causation between tracks and academic careers, most participating residents chose academic careers and reported few implementation barriers. The impact on faculty engagement (mentorship) with residents was reported to be high. Participating faculty reported a more holistic view of resident development, suggesting that scholarly tracks may offer more than educational benefits to participating residents, including individualized mentorship and career guidance. This work was conducted at a single site, and track-related education is dynamic, both locally and at other EM residencies. Future multisite research should build upon our evaluative work by investigating potential causation of track integration on resident career choice including comparative data analyzing pre- and post- track implementation.
Supplementary Information
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Suter RE Emergency medicine in the United States: a systemic review World J Emerg Med 2012315102521503110.5847/wjem.j.issn.1920-8642.2012.01.001PMC 4129827 · doi ↗ · pubmed ↗
- 2American Board of Emergency Medicine Subspecialty Dates & Fees 2018 Available at: https://www.abem.org/public/news-events/events/subspecialty-dates-fees Accessed December 28, 2023
- 3Accreditation Council for Graduate Medical Education Emergency Medicine Subspecialties 2015 Available at: https://www.acgme.org/specialties/emergency-medicine/overview/Accessed December 28, 2023
- 4Spector J London K Mongelluzo J Scholarly track training in emergency medicine residencies in 2017 West J Emerg Med 2018194.1S 20
- 5Jordan J Hwang M Coates WC Academic career preparation for residents - are we on the right track? Prevalence of specialized tracks in emergency medicine training programs BMC Med Educ 20181811843007577310.1186/s 12909-018-1288-x PMC 6076411 · doi ↗ · pubmed ↗
- 6Adams D Bischof J Larrimore AA longitudinal emergency medical services track in emergency medicine residency Cureus 201793 e 11272846587410.7759/cureus.1127 PMC 5409817 · doi ↗ · pubmed ↗
- 7Jordan J Hwang M Kaji AH Scholarly tracks in emergency medicine residency programs are associated with increased choice of academic career West J Emerg Med 201819359392976086110.5811/westjem.2018.1.36753 PMC 5942030 · doi ↗ · pubmed ↗
- 8Lubavin BV Langdorf MI Blasko BJ The effect of emergency medicine residency format on pursuit of fellowship training and an academic career Acad Emerg Med 2004119938431534754310.1197/j.aem.2004.03.019 · doi ↗ · pubmed ↗