Bilateral Optic Disc Edema in the Course of Idiopathic Intracranial Hypertension: A Case Report
Aleksandra Górska, Krzysztof Kuzniar, Malgorzata Kuzniar, Arlena Wyrebak

TL;DR
A 46-year-old woman with bilateral optic disc swelling and elevated cerebrospinal fluid pressure was diagnosed with idiopathic intracranial hypertension and showed improvement with treatment.
Contribution
This case report emphasizes the importance of early diagnosis and treatment of IIH to prevent permanent optic nerve damage.
Findings
Bilateral optic disc edema and elevated cerebrospinal fluid pressure confirmed a diagnosis of IIH.
Acetazolamide treatment improved visual acuity within one month.
Weight reduction was recommended to address contributing factors of IIH.
Abstract
Idiopathic intracranial hypertension (IIH) is a rare disease characterized by elevated cerebrospinal fluid pressure in the absence of structural changes in the brain. One of the main symptoms of IIH is deterioration of visual acuity with evidence of swelling of the optic nerve disc. Other complaints reported by patients may also include headaches, dizziness, and tinnitus. A 46-year-old female patient presented to the ophthalmology outpatient clinic because of bilateral visual acuity deterioration. The patient had previously been treated for hypertension and dizziness, and she also reported increasing obesity over the past three months. A fundus examination revealed bilateral swelling of the optic disc with obliterated borders and elevation above the fundus level. An optical coherence tomography study was also performed. The patient was consulted neurologically. A CT scan and an MRI of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
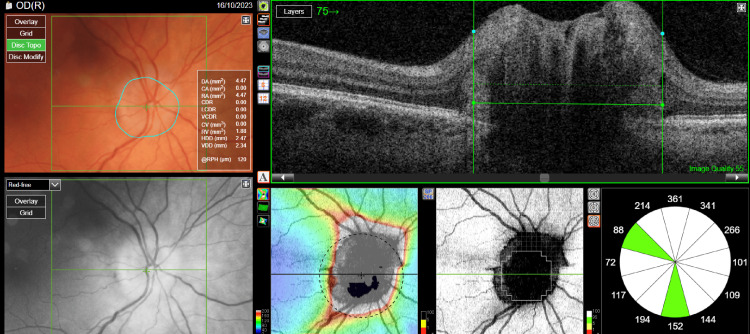 Figure 1
Figure 1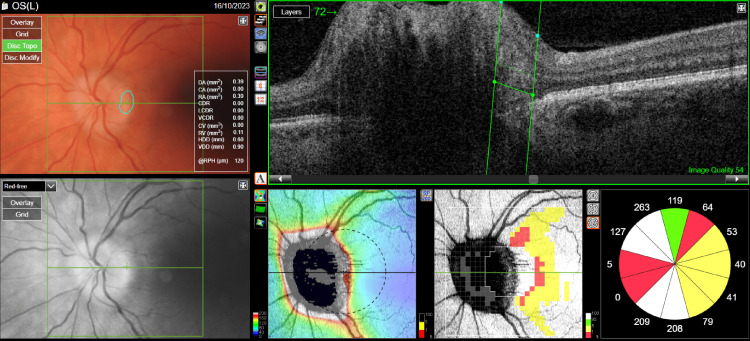 Figure 2
Figure 2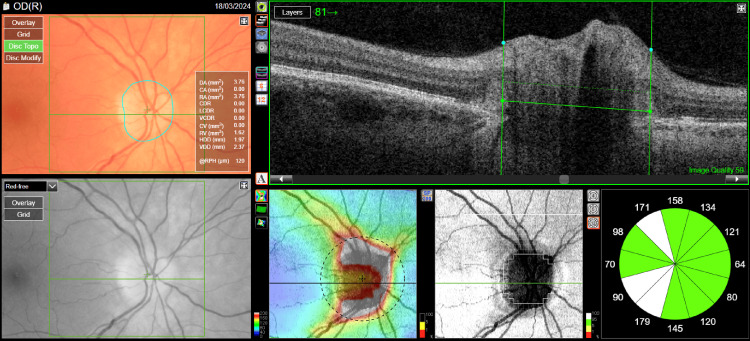 Figure 3
Figure 3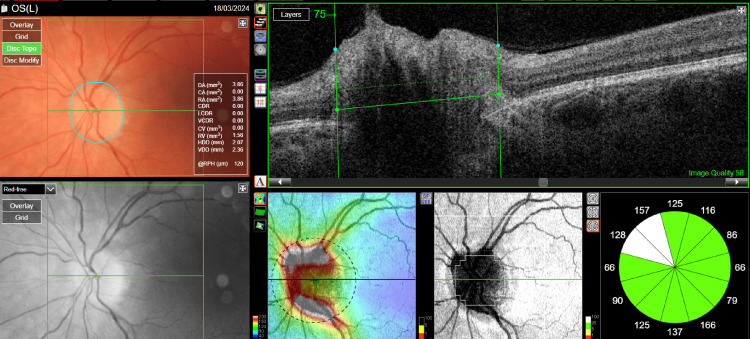 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Venous Sinus Thrombosis · Neurosurgical Procedures and Complications · Ocular Diseases and Behçet’s Syndrome
Introduction
Idiopathic intracranial hypertension (IIH), also known as pseudotumor cerebri, is a rare condition characterized by elevated cerebrospinal fluid pressure without an obvious cause such as a brain tumor or venous sinus thrombosis. Some of the main symptoms of IIH are bilateral swelling of the optic nerve disc, which can lead to deterioration of visual acuity and in extreme cases, even loss of vision, transient visual impairment, which can be triggered by changes in body position, and double vision (diplopia), which is usually horizontal and caused by paralysis of the VIth cranial nerve. Other symptoms reported by patients may include headaches that worsen when lying down, dizziness, and tinnitus, which is usually unilateral and can be auscultated as a murmur synchronous with the heart rate.
In this article, we present a case of a 46-year-old female patient with bilateral optic disc edema in the course of IIH.
Case presentation
A 46-year-old female patient presented to an ophthalmology outpatient clinic because of a bilateral deterioration of visual acuity that had persisted for about six months. She had a history of hypertension, obesity (rapid weight gain of 30 kg in three months), and dizziness for six years. A fundus examination showed bilateral swelling of the optic disc with obliterated borders and elevation above the fundus level (Figures 1, 2). Best-corrected visual acuity (BCVA) was 0.8 for the right eye and 0.7 for the left eye. The intraocular pressure of the right eye was 20 mmHg, and that of the left eye was 19 mmHg. Optical coherence tomography (OCT) was performed, and fundus photography was taken.
Optical coherence tomography of the optic nerve disc of the right eye before treatment.
Optical coherence tomography of the optic nerve disc of the left eye before treatment.
A computed tomography (CT) scan of the head without contrast and a magnetic resonance (MR) scan of the head with contrast were performed to expand the diagnosis, which showed no abnormalities. The patient was referred to the neurology department, where a lumbar puncture was performed. The cerebrospinal fluid (CSF) was watery, clear, with pleocytosis of 1, protein, and normal glycemia. The CSF pressure was 450 mmH₂O (normal for an obese person is up to 250 mmH₂O). Based on the findings, IIH was diagnosed.
Treatment with acetazolamide at a dose of 2 x 250 mg was started. After one month of treatment, visual acuity improved to 1.0 in both eyes, and disc edema decreased (Figures 3, 4). The patient remains under constant follow-up with the ophthalmology clinic, neurology clinic, and metabolic disease clinic.
Optical coherence tomography of the optic nerve disc of the right eye after treatment.
Optical coherence tomography of the optic nerve disc of the left eye after treatment.
Discussion
IIH, also known as pseudotumor of the brain, is a rare but potentially dangerous condition that can lead to serious complications, including permanent optic nerve damage [1]. In the case of our 46-year-old patient, the key symptom that prompted further diagnosis was bilateral swelling of the optic disc. IIH occurs predominantly in young, obese women of childbearing age, as also confirmed by the case of our patient, who experienced a rapid weight gain of 30 kg in three months [2,3].
Imaging studies such as CT and MRI are crucial in the diagnosis of IIH to exclude other causes of elevated intracranial pressure, such as brain tumors, venous sinus thrombosis, or infections [4]. In our patient's case, both CT and MRI of the head showed no abnormalities, which confirmed the diagnosis of IIH. However, the most important test in the diagnosis of IIH is lumbar puncture with measurement of CSF pressure. In our patient, the CSF pressure was 450 mmH₂O (45 cmH₂O), which is markedly elevated compared to the normal range (50-150 mmH₂O in healthy individuals) and exceeds even the upper limit seen in obese patients with IIH (typically ≤250 mmH₂O) [5].
Treatment of IIH, depending on the severity of symptoms, is based on three main pillars: weight reduction, pharmacotherapy, and, in some cases, surgical intervention [6]. Acetazolamide, a carbonic anhydrase inhibitor, is the first-line treatment for moderately severe cases of IIH. It reduces cerebrospinal fluid production, leading to a reduction in intracranial pressure [7]. In our patient's case, treatment with acetazolamide was initiated, and after one month of therapy, a significant improvement in visual acuity from 0.7/0.8 to 1.0 was observed in both eyes. However, long-term treatment of IIH requires ongoing ophthalmic and neurological care to monitor disease progression and prevent recurrence [1].
The main complication of IIH is loss of vision due to swelling of the optic disc. This swelling leads to compression of ganglion cell axons, which can result in their death and permanent loss of visual function [8]. In our patient's case, the correct diagnosis and implemented treatment prevented these complications.
IIH is a condition with a complex etiology, and its pathophysiology is not fully understood. Abnormalities in CSF flow and increased resistance to CSF outflow are thought to play a key role [9]. In addition, hormonal factors, particularly in women, may play an important role in the development of IIH. In our patient's case, rapid weight gain may have been one of the triggers [10].
The literature highlights the importance of early diagnosis and treatment of IIH to prevent permanent optic nerve damage [1]. A study by Friedman et al. showed that early implementation of acetazolamide treatment significantly improves the prognosis of patients with IIH [4]. Similarly, Sinclair et al. highlighted that not only drug treatment but also weight reduction can lead to long-term remission of the disease [11].
IIH is a rare but serious condition that requires comprehensive diagnosis and treatment. In the case of our patient, early diagnosis and the implementation of acetazolamide treatment allowed a significant improvement in visual acuity and prevented further damage to the optic nerve. Imaging studies and measurement of cerebrospinal fluid pressure are crucial in the diagnosis of IIH, and treatment should include both pharmacotherapy and weight reduction [4,5].
Conclusions
Idiopathic intracranial hypertension should be considered in the differential diagnosis of bilateral optic disc edema, especially in patients with obesity and other risk factors. Imaging studies and measurement of CSF pressure are crucial in making a correct diagnosis. Early implementation of treatment can prevent permanent optic nerve damage and improve patients' prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Idiopathic intracranial hypertension Neurol Clin Wall M 5936172820102063799110.1016/j.ncl.2010.03.003PMC 2908600 · doi ↗ · pubmed ↗
- 2Epidemiology of idiopathic intracranial hypertension in Israel J Neuroophthalmol Kesler A Gadoth N 1214212001 https://pubmed.ncbi.nlm.nih.gov/11315973/1131597310.1097/00041327-200103000-00003 · doi ↗ · pubmed ↗
- 3The relationship between obesity and idiopathic intracranial hypertension Int J Obes Relat Metab Disord Rowe FJ Sarkies NJ 5459231999 https://pubmed.ncbi.nlm.nih.gov/10094577/10.1038/sj.ijo.080075810094577 · doi ↗ · pubmed ↗
- 4Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children Neurology Friedman DI Liu GT Digre KB 115911658120132396624810.1212/WNL.0b 013e 3182 a 55f 17 · doi ↗ · pubmed ↗
- 5Evolving evidence in adult idiopathic intracranial hypertension: pathophysiology and management J Neurol Neurosurg Psychiatry Mollan SP Ali F Hassan-Smith G Botfield H Friedman DI Sinclair AJ 9829928720162688896010.1136/jnnp-2015-311302 PMC 5013119 · doi ↗ · pubmed ↗
- 6Idiopathic intracranial hypertension (pseudotumor cerebri): recognition, treatment, and ongoing management Curr Treat Options Neurol Thurtell MJ Wall M 1121520132313603510.1007/s 11940-012-0207-4PMC 3554852 · doi ↗ · pubmed ↗
- 7Treatment of idiopathic intracranial hypertension: topiramate vs acetazolamide, an open-label study Acta Neurol Scand Celebisoy N Gökçay F Sirin H Akyürekli O 32232711620071792272510.1111/j.1600-0404.2007.00905.x · doi ↗ · pubmed ↗
- 8Asymmetric papilledema in idiopathic intracranial hypertension J Neuroophthalmol Bidot S Bruce BB Saindane AM Newman NJ Biousse V 31363520152549419710.1097/WNO.0000000000000205 PMC 4326590 · doi ↗ · pubmed ↗