Outcome of Follow-Up Care Frequency on the Glycemic Control of Diabetic Patients in Qassim, Saudi Arabia
Omar M Aldhabbah, Saulat Jahan

TL;DR
This study shows that regular follow-up care improves blood sugar control in diabetic patients in Saudi Arabia.
Contribution
The study demonstrates a direct link between follow-up frequency and glycemic control in diabetic patients in Qassim.
Findings
75.2% of diabetic patients had poor glycemic control (HbA1c ≥ 7%).
Only 11.9% of patients received routine follow-up care.
Regular follow-up was significantly associated with better glycemic control.
Abstract
Aims The aim of this study was to investigate the outcome of follow-up care frequencies on the glycemic control of diabetic patients in Qassim, Saudi Arabia. Methods A retrospective review of the electronic medical records of diabetic patients registered during the period August 2022 to July 2024 at King Fahad Specialist Hospital (KFSH) in Qassim was conducted. The association between follow-up care and various metabolic outcomes was determined by applying the chi-square test and Fisher's exact test. SPSS software version 22.0 (IBM Corp., Armonk, NY, US) was used for data analysis. Results The study included 286 patients with diabetes; 75.2% of them had glycemic control issues (HbA1c ≥ 7%), 56.3% of patients saw a doctor just once during the study period, and only 11.9% of patients received routine follow-up. Glycemic control and follow-up frequency were found to be significantly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
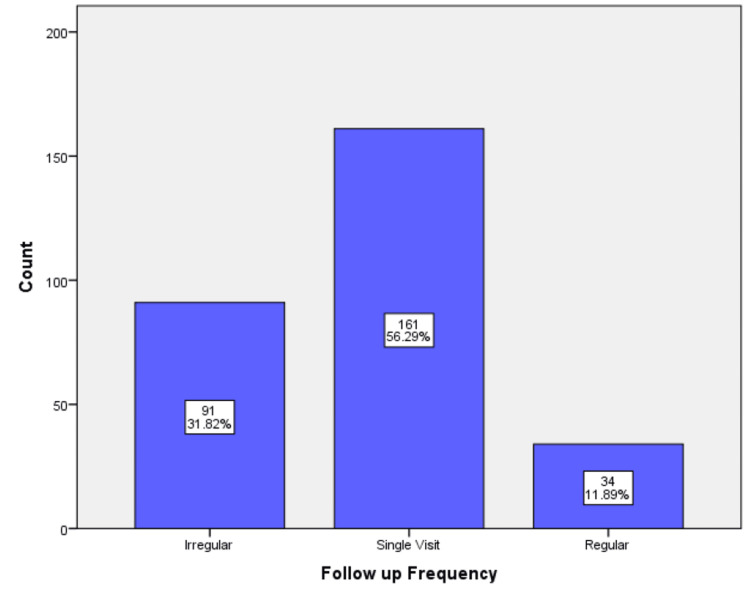 Figure 1
Figure 1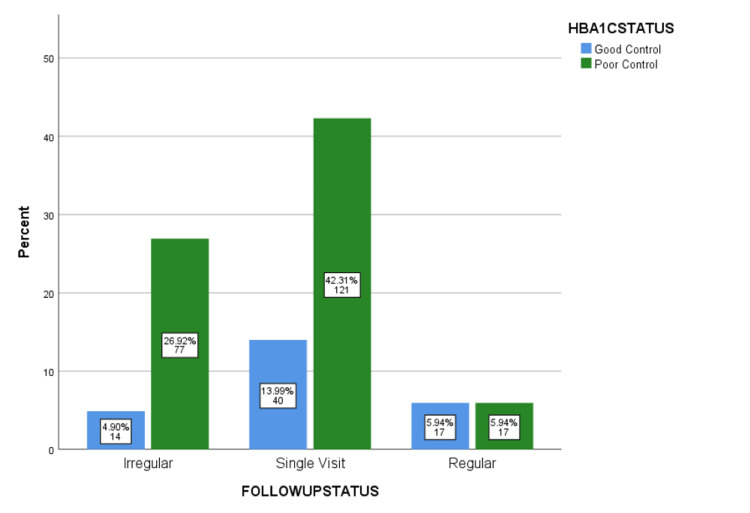 Figure 2
Figure 2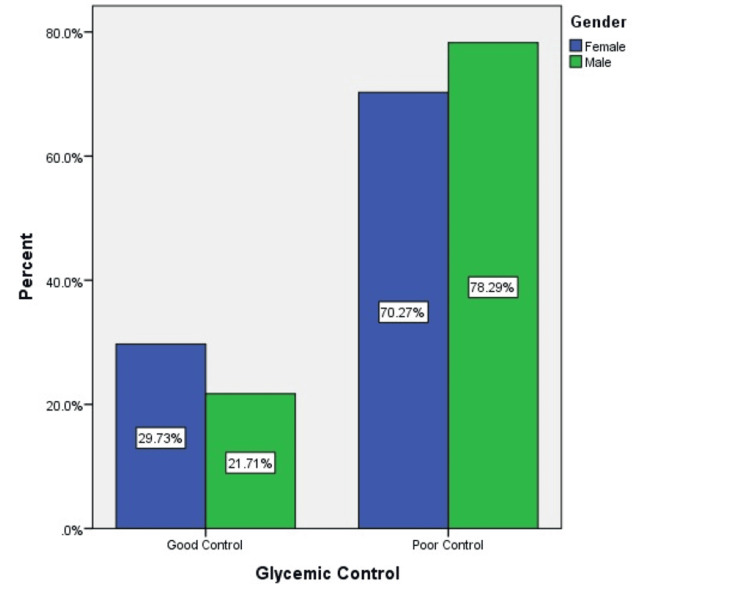 Figure 3
Figure 3| Variable | Mean ± SD | Range (Min–Max) | Valid N |
| Age (years) | 60.5 ± 11.3 | 28 – 108 | 286 |
| BMI (kg/m²) | 28.0 ± 5.2 | 16.0 – 45.5 | 228 |
| HbA1c (%) | 8.35 ± 1.98 | 5.1 – 17.8 | 286 |
| LDL (mmol/L) | 2.49 ± 1.01 | 0.85 – 6.90 | 221 |
| HDL (mmol/L) | 1.02 ± 0.30 | 0.20 – 3.10 | 248 |
| Triglycerides (mmol/L) | 1.68 ± 1.08 | 0.30 – 8.50 | 226 |
| Cholesterol (mmol/L) | 4.00 ± 1.18 | 1.90 – 9.10 | 232 |
| Serum creatinine (µmol/L) | 94.5 ± 75.3 | 36 – 859 | 277 |
| Follow-up Visits | Irregular | Single | Regular | χ²-value | p-value |
| Glycemic Control | |||||
| HbA1c <7% | 14 | 40 | 17 | 15.892 | <0.0001 |
| HbA1c ≥7% | 77 | 121 | 17 | ||
| Total Cholesterol | |||||
| Normal | 75 | 120 | 27 | 3.997 | 0.1 |
| High | 1 | 6 | 3 | ||
| Triglyceride | |||||
| Normal | 60 | 96 | 25 | 2.788 | 0.248 |
| High | 10 | 30 | 5 | ||
| LDL Cholesterol | |||||
| Normal | 71 | 112 | 24 | 5.291 | 0.057 |
| High | 1 | 10 | 3 | ||
| HDL Cholesterol | |||||
| Normal/High HDL | 54 | 64 | 18 | 4.22 | 0.118 |
| Low HDL | 32 | 67 | 13 | ||
| Lipid Profile | HbA1c <7% | HbA1c ≥7% | χ²-value | p-value |
| Total Cholesterol | ||||
| Normal | 50 | 172 | __ | 1 |
| High | 2 | 8 | ||
| Triglyceride | ||||
| Normal | 50 | 131 | 3.949 | 0.054 |
| High | 6 | 39 | ||
| LDL Cholesterol | ||||
| Normal | 54 | 153 | __ | 0.526 |
| High | 2 | 12 | ||
| HDL Cholesterol | ||||
| Normal/High HDL | 40 | 96 | 5.249 | 0.015 |
| Low HDL | 19 | 93 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Management and Education · Diabetes, Cardiovascular Risks, and Lipoproteins · Chronic Disease Management Strategies
Introduction
Diabetes mellitus (DM) is becoming more prevalent worldwide. Diabetes is a chronic illness that arises from insufficient insulin production by the pancreas or the body's inability to utilize the insulin that is produced. Uncontrolled diabetes frequently results in hyperglycemia, also known as elevated blood glucose or elevated blood sugar, which, over time, seriously damages numerous organs and tissues, including the blood vessels and nerve cells [1]. The International Diabetes Federation reports that 537 million adults aged between 20 and 79 years have diabetes. By 2030, this figure is expected to increase to 643 million, and by 2045, it is expected to reach 783 million [2]. Diabetes increases the likelihood of having various health problems such as cardiovascular disease, renal disease, and retinopathy. However, people with diabetes who receive high-quality medical care with continuity experience fewer complications [3,4]. Even though many patients do not receive optimal-quality care and good results are rarely obtained, preventive medical care has the potential to improve health outcomes. A significant number of patients do not receive regular care, resulting in diabetic complications [5].
In primary care, regular follow-up care has been linked to lower rates of hospitalizations, reduced Emergency Room (ER) visits, increased patient satisfaction, and significantly lower healthcare expenditures [6]. Despite the importance of continuity of care, there are some limitations to accessing the services in some countries and difficulties in coordinating primary and secondary care. Longer doctor-patient relationships are substantially linked to lower mortality and fewer acute hospital admissions. The fact that continuity and these results have a dose-response connection suggests that these relationships are crucial [7]. Numerous studies looked into the connection between metabolic outcomes and follow-up frequency in type 2 DM (T2DM) patients. These findings led us to look more closely at the relationship between glycemic control and follow-up frequency [8]. Also, many studies have shown that continuous care plays a crucial role in improving metabolic control and reducing complications in people with diabetes [9,10]. However, there remains a gap in research that focuses on how this relationship applies in typical clinical settings. This study was conducted to investigate the impact of follow-up care on the glycemic control of diabetic patients. Furthermore, lipid profile, renal function, and liver function parameters were compared between T2DM patients with good glycemic control (HbA1c >7) and those with poor glycemic control (HbA1c <7).
Materials and methods
Study design and setting
This is a retrospective record review of patients with diabetes who received follow-up care and were registered in King Fahad Specialist Hospital (KFSH), Buraidah City, Qassim, Saudi Arabia. As a tertiary care center, KFSH provides specialized services to a varied patient population. Its electronic health record system enabled efficient access to appropriate patient data, particularly for those receiving continuing care for diabetes. Patients involved in the study were adults aged 18 years or older who had an established diagnosis of Type 2 diabetes mellitus (T2DM), had at least one documented HbA1c result between August 2022 and July 2024, and attended at least one follow-up visit for diabetes management during the study period. Patients were excluded if they had significant comorbidities that could independently affect glycemic control, such as advanced chronic kidney disease (stage 4 or 5), liver cirrhosis, active malignancy, or congestive heart failure (NYHA (New York Heart Association) classes III-IV), or had incomplete or missing medical records (especially lacking HbA1c or follow-up data). The form used to extract data from the electronic medical records of eligible diabetic patients is shown in the Appendices.
Data source and data management
Patients’ electronic records at KFSH, from August 2022 to July 2024, were obtained. Following ADA (American Diabetes Association) recommendations for follow-up frequency, alongside typical clinical standards, patients were categorized into three groups based on the frequency of their follow-up visits. The first group comprised those with regular follow-up, defined as attending scheduled visits regularly, every three to six months throughout the study period. The second group contained patients with irregular follow-up, who had multiple visits but did not meet the recommended minimum number of visits. The third group consisted of patients with only a single recorded follow-up visit during the entire study period. A qualified family physician reviewed the records and extracted the data on age, gender, HbA1c levels, follow-up care frequency, lipid profile, and renal function parameters.
Laboratory parameters were classified based on standard clinical guidelines and the hospital’s laboratory reference ranges. HbA1c was reflected as controlled if it was less than 7%, and uncontrolled if it was 7% or higher, in agreement with the ADA guidelines. Triglyceride levels were reflected as high if they were 150 mg/dL or more, while low-density lipoprotein (LDL) cholesterol was reflected as high if it was 130 mg/dL or more. High-density lipoprotein (HDL) cholesterol was reflected as low if it was below 40 mg/dL for men or below 50 mg/dL for women. Total cholesterol was classified as high if it was 200 mg/dL or more.
Data analysis
Our descriptive statistics included means, standard deviations, frequencies, and percentages. To examine inferential tests, the chi-square test and Fisher's exact test were performed. Statistical significance was defined as a p-value of less than or equal to 0.05. SPSS software version 22.0 (IBM Corp., Armonk, NY, US) was used for data analysis.
Ethical considerations
The Regional Research Ethics Committee, Qassim, provided ethical approval for this study (Reg No: 607-46-6466). Utmost privacy and confidentiality were maintained for all data. Patient records were anonymized, and data access was limited to the research team. The collected data were securely stored in encrypted, password-protected files throughout the study and afterward. This ensured ethical research practices and adherence with data protection rules.
Results
A total of 286 diabetic patients were included in the study. Of these, 175 (61.2%) were males and 111 (38.8%) were females, reflecting a male predominance in the study population. The majority were Saudi Nationals (n = 243, 85.0%), while 43 patients (15.0%) were non-Saudi.
Table 1 summarizes the clinical characteristics of the patients. The mean age of the patients was 60.5 (± 11.3) years. Additionally, the study population had an average BMI of 28.0 (± 5.2) kg/m2. The overall glycemic control was poor, as demonstrated by the mean HbA1c of 8.35%. With a mean LDL of 2.49 (± 1.01) mmol/L and a serum creatinine of 94.5 (± 75.3) umol/L, the lipid and renal profiles were within the normal ranges.
Table 2 summarizes the relationship between follow-up visit frequency and key metabolic markers. Glycemic control and follow-up status were found to be significantly associated (χ² = 15.892, p < 0.001), suggesting that patients who had regular follow-up had a higher chance of achieving good HbA1c levels. Total cholesterol (p = 0.100), triglycerides (p = 0.248), LDL cholesterol (p = 0.057), and HDL cholesterol (p = 0.118) did not show a statistically significant association with follow-up status; however, LDL cholesterol was almost significant.
Table 3 details the relationship between glycemic control and lipid profile parameters. HbA1c levels and HDL cholesterol were found to be significantly associated (χ² = 5.249, p = 0.015), with low HDL more common in patients with inadequate glycemic control. Although triglycerides approached significance (p = 0.054), there were no statistically significant associations with total or LDL cholesterol.
Figure 1 shows the distribution of patients by follow-up frequency. The majority of patients (56.3%) had only a single follow-up visit, while just 11.9% maintained regular follow-up, highlighting a gap in continuity of care among diabetic patients.
Distribution of diabetic patients by follow-up frequency
Figure 2 shows the glycemic control status of diabetic patients by follow-up frequency. The percentage of regular visits was low for both groups (5.94%). However, individuals with poor glycaemic control had noticeably more irregular visits (26.92%) and single visits (42.31%) than patients with good control (4.90% irregular, 13.99% single). This shows clearly that individuals who do not receive regular follow-up typically have poorer blood sugar control.
Glycemic control status of diabetic patients by follow-up frequency
Figure 3 illustrates glycemic control status by gender. A higher proportion of males (78.3%) had poor glycemic control compared to females (70.3%). Conversely, good control was more common among females (29.7%) than males (21.7%).
Distribution of glycemic control status by gender
Discussion
This study examined the association between glycemic control and the frequency of follow-up care among patients with diabetes in Qassim. Our findings showed that patients who had regular follow-up were significantly more likely to achieve good glycemic control (HbA1c < 7%) than those who only occasionally or infrequently obtained follow-up (χ² = 15.892, p < 0.001).
The ADA suggests routine HbA1c monitoring every three to six months and more frequently for those with poor control or treatment changes, emphasizing that continuity of care is a key determinant in successful diabetes management [11].
During the study period, more than half of the population (56.3%) had only one recorded follow-up, while only 11.9% had regular follow-up. The high rate of poor glycemic control observed (75.2% of patients with HbA1c ≥ 7%) may be partially explained by this, which highlights a significant gap in long-term care continuity. These findings are consistent with previous studies conducted in Saudi Arabia, which reported the same patterns in limited follow-up adherence and its link to suboptimal outcomes [12,13]. In addition, nearly three-quarters of patients with type 2 diabetes in northern Saudi Arabia had poor glycemic control, with contributing factors including obesity, long disease duration, and poor adherence to lifestyle measures [14].
Low HDL cholesterol was linked to poor glycemic control (χ² = 5.249, p = 0.015), supporting evidence that HDL is a marker of cardiovascular protection and insulin sensitivity [15]. Although no significant associations were found between LDL and triglyceride levels, their borderline p-values (p = 0.057 and 0.054, respectively) suggest that correlations may become more apparent in a larger sample or over a longer study period.
The metabolic and clinical profile of this study, with a mean BMI of 28.0 kg/m², elevated HbA1c, and modest lipid abnormalities, is consistent with the typical cardiometabolic risk cluster seen in patients with T2DM. These findings highlight the importance of integrated care models that not only monitor glucose but also address weight, blood pressure, and lipid control during routine follow-up, as emphasized in current international guidelines and demonstrated in local interventional research [11,16]. Moreover, Tourkmani et al. revealed that applying a structured, multidisciplinary care program with regular follow-up led to significant improvements in HbA1c, lipid profiles, and blood pressure control [16].
Despite the value of using real-world clinical data, this study has limitations. Sociodemographic factors that are known to affect the course of chronic diseases, such as access to care, education, and income, were not evaluated. Based on the results of our study, we recommend increasing awareness about the sustained benefits of regular follow-up of diabetic patients in healthcare settings. Further research is recommended to investigate the relationships between specific follow-up schedules and long-term metabolic results.
Conclusions
This study showed a statistically significant relationship between glycemic control and frequency of subsequent testing in diabetic patients in Qassim. Individuals who consistently attended their scheduled follow-up visits demonstrated a significantly increased likelihood of achieving their HbA1c targets. This highlights the positive impact of routine, scheduled appointments in improving health outcomes and decreasing the incidence of diabetes-related complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diabetes. World Health Organization 3 2024 2024 https://www.who.int/news-room/fact-sheets/detail/diabetes
- 2IDF. The diabetes atlas 4 2024 n.dhttps://diabetesatlas.org/
- 3The relationship between type 2 diabetic patients' early medical care--seeking consistency to the same clinician and health care system and their clinical outcomes Medicine (Baltimore) Liao PJ Lin ZY Huang JC Hsu KH 094201510.1097/MD.0000000000000554 PMC 455416225700326 · doi ↗ · pubmed ↗
- 4Interpersonal continuity of care and type two diabetes Prim Care Diabetes Lustman A Comaneshter D Vinker S 1651701020162653031710.1016/j.pcd.2015.10.001 · doi ↗ · pubmed ↗
- 5Measuring continuity of care in diabetes mellitus: an experience-based measure Ann Fam Med Gulliford MC Naithani S Morgan M 548555420061714863410.1370/afm.578PMC 1687166 · doi ↗ · pubmed ↗
- 6Importance of continuity of care from a patient perspective - a cross-sectional study in Swedish health care Scand J Prim Health Care Cohen E Lindman I 1952004220243818994510.1080/02813432.2023.2299119 PMC 10851828 · doi ↗ · pubmed ↗
- 7Continuity in general practice as predictor of mortality, acute hospitalisation, and use of out-of-hours care: a registry-based observational study in Norway Br J Gen Pract Sandvik H HetlevikØ Blinkenberg J Hunskaar S 09072202210.3399/BJGP.2021.0340 PMC 851069034607797 · doi ↗ · pubmed ↗
- 8Follow-up frequency and clinical outcomes in patients with type 2 diabetes: a prospective analysis based on multicenter real-world data J Diabetes Zhao Q Li H Ni Q 3063141420223561385010.1111/1753-0407.13271 PMC 9366569 · doi ↗ · pubmed ↗