Refractory hypoxaemia in the presence of two common conditions: a case report
José Gregorio Soto Rojas, Elvira Carrión Ríos, Isabel Maria Jorquera Lozano, Raul Reyes Parrilla, Ricardo Fajardo Molina

TL;DR
A 72-year-old woman with a pacemaker and a patent foramen ovale experienced hypoxaemia due to a right-to-left shunt caused by pacemaker-related tricuspid regurgitation.
Contribution
The paper presents a novel explanation for hypoxaemia in the absence of pulmonary hypertension, linking pacemaker interference with a right-to-left shunt.
Findings
Hypoxaemia was resolved immediately after percutaneous closure of the patent foramen ovale.
Right-to-left shunt was attributed to pacemaker-mediated tricuspid regurgitation and elevated right atrial pressure.
Pulmonary hypertension and platypnoea–orthodeoxia syndrome were ruled out as causes of the shunt.
Abstract
A 72-year-old woman with a history of bicameral pacemaker implantation 12 years earlier due to high-degree atrioventricular block presented with progressively worsening exertional dyspnoea, which recently became evident even with minimal exertion. When the patient consulted, marked hypoxaemia was observed, leading to the exclusion of pulmonary aetiology using computed tomography (CT) angiography. Subsequently, an echocardiogram revealed significant tricuspid regurgitation caused by interference with the pacemaker lead. A bubble study demonstrated a right-to-left shunt in the context of a patent foramen ovale. Given the patient’s age, the initial hypothesis was that the shunt direction resulted from a condition causing severe pulmonary hypertension, resembling Eisenmenger syndrome. However, right heart catheterization ruled out significant pulmonary hypertension. Since the presence of a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
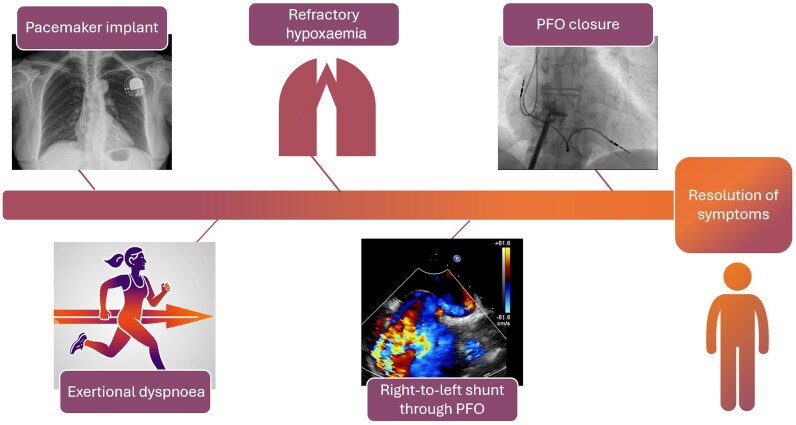 Figure 1
Figure 1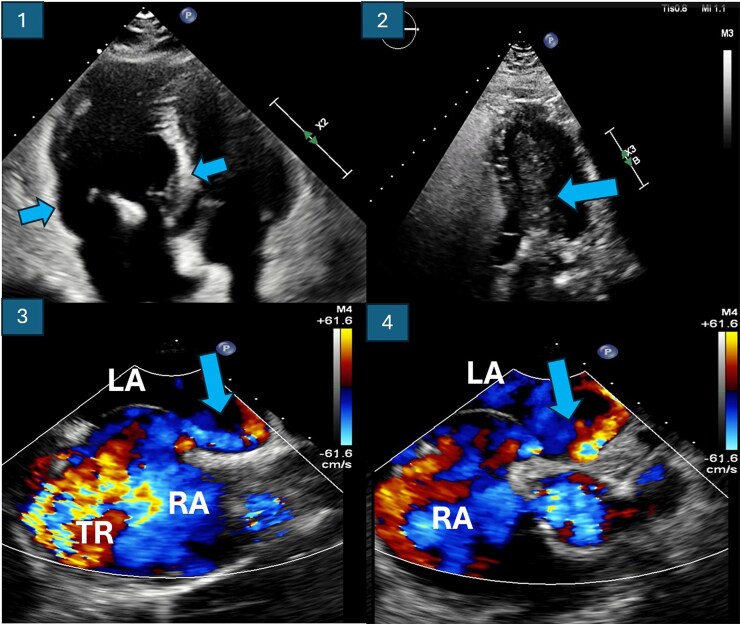 Figure 1
Figure 1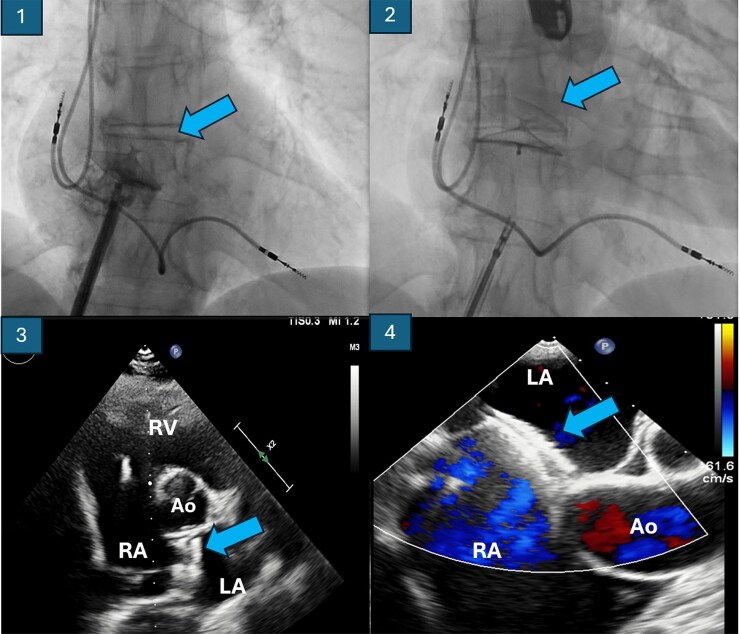 Figure 2
Figure 2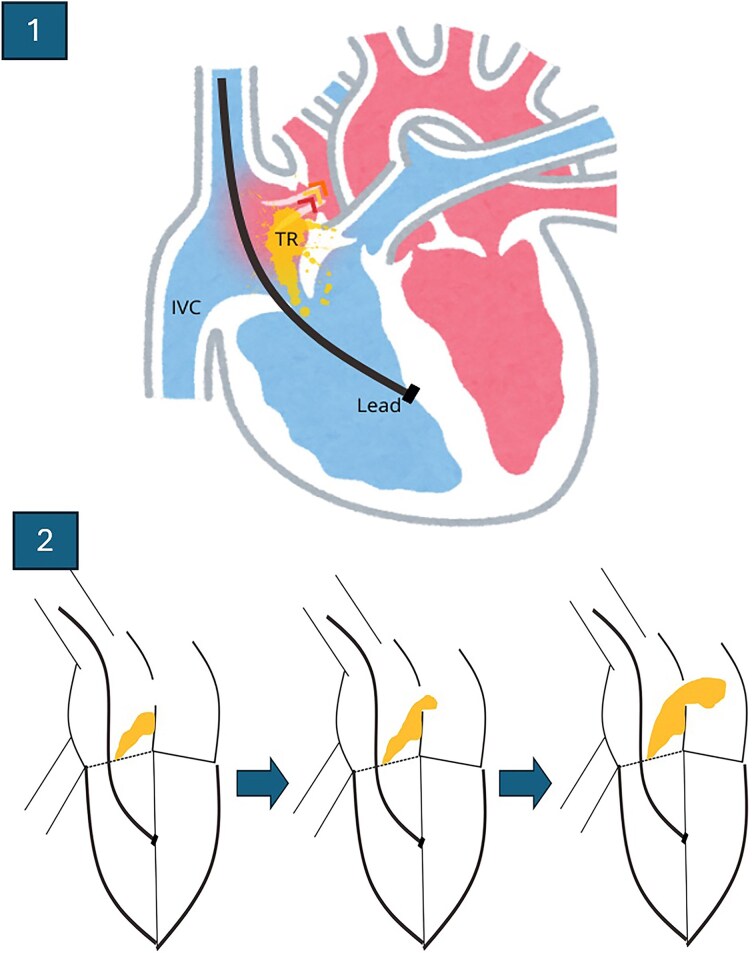 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Congenital Heart Disease Studies · Respiratory Support and Mechanisms
Introduction
The presence of a patent foramen ovale (PFO) is generally regarded as a normal anatomical variant, given its high prevalence in the general population.^1^ Similarly, tricuspid regurgitation (TR) caused by pacemaker lead interference has been a highly prevalent condition that has, until recently, been underestimated in terms of its clinical impact and prognosis.^2^ We present a case in which the interaction between these two conditions leads to the development of a clinically significant right-to-left shunt, manifesting as severe and refractory hypoxaemia.
Summary figure
Timeline summarizing the clinical course of a patient with a history of pacemaker implantation who developed a right-to-left shunt through a patent foramen ovale, secondary to tricuspid regurgitation caused by the device lead. Resolution of hypoxaemia was achieved following patent foramen ovale closure. PFO, patent foramen ovale.
Case presentation
A 72-year-old Caucasian female patient with a history of hypertension and dyslipidaemia, well managed on angiotensin receptor blockers and statins, presented to her primary care physician with a 2- to 3-month history of exertional dyspnoea that progressively limited her daily activities. Her medical history included a dual-chamber pacemaker implanted 12 years ago at another institution for high-grade paroxysmal atrioventricular block, with no further follow-up or echocardiographic data available since the implantation. She reported no orthopnoea or symptoms suggestive of decompensated heart failure, and no other significant comorbid conditions were identified. On examination, breath sounds were normal with no signs of congestion or peripheral oedema. A Grade III/VI systolic murmur was audible at the left sternal border.
The patient was referred to cardiology, where an initial transthoracic echocardiogram (TTE) revealed preserved left ventricular ejection fraction with significant TR due to interference from the pacemaker lead. No other significant abnormalities were identified. Laboratory tests, including N-terminal pro-B-type natriuretic peptide levels, were unremarkable, leading to a referral to pulmonology for further evaluation.
Pulmonary function tests did not reveal any abnormalities. However, baseline pulse oximetry demonstrated an oxygen saturation of ∼85%, prompting referral to the emergency department to exclude acute pathology. A computed tomography pulmonary angiogram ruled out pulmonary embolism and revealed no evidence of interstitial lung disease. Arterial blood gas analysis showed hypoxaemic respiratory failure with associated hypocapnia, necessitating hospital admission for further evaluation.
The patient required high-flow oxygen therapy, yet her oxygen saturation remained below 90%. Given the severe hypoxaemia refractory to oxygen supplementation, a cardiology consultation was requested during hospitalization to investigate a potential shunt. Repeat TTE revealed persistent moderate-to-severe TR due to pacemaker lead interference, as well as mild right ventricular dilation. A contrast-enhanced bubble study with agitated saline suggested a right-to-left intracardiac shunt, likely through a PFO (Figure 1).
Image 1: Baseline transoesophageal echocardiogram showing right chamber dilation. Image 2: Transthoracic echocardiogram with bubble test demonstrating early massive passage of bubbles into the left chambers. Images 3 and 4: Transoesophageal echocardiogram showing the right-to-left shunt through the patent foramen ovale, as well as the tricuspid regurgitation jet. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TR, tricuspid regurgitation.
Subsequent transoesophageal echocardiography (TEE) confirmed a PFO with a baseline right-to-left shunt, severe TR (in contrast to the moderate-to-severe TR observed on the initial TTE), and findings suggestive of pulmonary hypertension (PH), including a tricuspid regurgitant velocity of 2.8 m/s and right heart chamber dilation (Figure 1). Right heart catheterization measured a pulmonary artery systolic pressure of 31 mmHg, mean pressure of 18 mmHg, and a pulmonary vascular resistance of 2.3 Wood units, excluding significant PH.
Based on these findings, we proceeded with percutaneous closure of the PFO under echocardiographic and angiographic guidance using a Figulla Flex II Uni 28 device via right femoral access (Figure 2). The intervention resulted in prompt improvement in arterial oxygen saturation, enabling discontinuation of high-flow oxygen therapy. Post-procedural imaging confirmed proper device placement (Figure 2), and the patient was discharged without supplementary oxygen.
Closure device for foramen. In the images above (1 and 2), fluoroscopy shows the deployment of the device. In the images below, the outcome of the implant is visualized through transthoracic echocardiography on the left (3) and transoesophageal echocardiography (4), without evidence of residual shunt. Ao, aorta; LA, left atrium; RA, right atrium; RV, right ventricle.
The patient continued follow-up at another centre, where she progressively developed symptoms of right heart failure related to the progression of the severe TR. She underwent elective surgery for lead extraction, implantation of a leadless device, and tricuspid annuloplasty. Currently, 2 years after the episode, the patient remains asymptomatic in functional Class I, without further episodes of respiratory failure.
Discussion
We encountered a patient with refractory hypoxaemia, who had a history of permanent pacemaker implantation and significant TR. A bubble study revealed evidence of a right-to-left shunt, which was subsequently confirmed by TEE, in the presence of a PFO. Contrary to initial suspicion, right heart catheterization ruled out Eisenmenger syndrome by excluding significant elevations in pulmonary arterial pressures.
Although right-to-left shunting through a PFO in the absence of PH has been described,^3^ particularly in the context of platypnoea–orthodeoxia syndrome,^4,5^ our patient did not exhibit postural changes in oxygen saturation, making this diagnosis less likely. Isolated cases have been reported in which a PFO shunt was driven by the direction of the TR jet.^6^ Similarly, in, our case, pacemaker lead-induced TR was identified as a potential contributor to the shunt pathophysiology.
It is well known that TR following pacemaker lead implantation is highly prevalent and associated with worse clinical outcomes, with significant regurgitation often developing within the first 2 years post-implantation.^2,7^ Although we lacked serial echocardiographic data from follow-up, the clinical course suggested progressive TR worsening. An eccentric regurgitant jet directed towards the interatrial septum, along with increasing right atrial systolic pressure, likely promoted a right-to-left shunt across the PFO (Figure 3). Moreover, the prompt resolution of hypoxaemia after PFO closure reinforces the notion that the foramen, in association with TR, is the underlying mechanism of the clinical presentation.
Image 1: Diagram of how pacemaker lead-mediated tricuspid regurgitation generates an eccentric jet directed towards the foramen ovale. Image 2: Schematic evolution of the progression of tricuspid regurgitation and the increase in inflow through the foramen as the severity of regurgitation worsens. IVC, inferior vena cava; TR, tricuspid regurgitation.
Conclusions
In clinical practice, the presence of a PFO is frequently encountered. Notably, a significant proportion of these patients, for diverse clinical indications, will eventually require permanent pacemaker implantation. A well-recognized but often underappreciated complication of this procedure is pacemaker-mediated TR, a condition that remains insufficiently addressed despite its high prevalence. Besides, when TR is attributed to pacemaker lead interference, it tends to progress rapidly, often presenting with eccentric regurgitant jets and portending adverse clinical outcomes.
Contemporary understanding of device-induced TR has evolved. However, many affected individuals continue to lack structured follow-up or targeted management strategies. This case highlights the importance of diagnosing and monitoring pacemaker-mediated TR. Furthermore, it illustrates how the interaction between two common pathologies can lead to severe hypoxaemia in an elderly patient without additional comorbidities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giblett JP, Williams LK, Kyranis S, Shapiro LM, Calvert PA. Patent foramen ovale closure: state of the art. Interv Cardiol 2020;15:e 15.33318751 10.15420/icr.2019.27PMC 7726850 · doi ↗ · pubmed ↗
- 2Prihadi EA, Delgado V, Leon MB, Enriquez-Sarano M, Topilsky Y, Bax JJ. Morphologic types of tricuspid regurgitation: characteristics and prognostic implications. JACC Cardiovasc Imaging 2019;12:491–499.30846123 10.1016/j.jcmg.2018.09.027 · doi ↗ · pubmed ↗
- 3Chen GP, Goldberg SL, Gill EA Jr. Patent foramen ovale and the platypnea–orthodeoxia syndrome. Cardiol Clin 2005;23:85–89.15676271 10.1016/j.ccl.2004.10.003 · doi ↗ · pubmed ↗
- 4Godart F, Rey C, Prat A, Vincentelli A, Chmaït A, Francart C, et al Atrial right-to-left shunting causing severe hypoxaemia despite normal right-sided pressures: report of 11 consecutive cases corrected by percutaneous closure. Eur Heart J 2000;21:483–489.10681489 10.1053/euhj.1999.1944 · doi ↗ · pubmed ↗
- 5Rodrigues P, Palma P, Sousa-Pereira L. Platypnea–orthodeoxia syndrome in review: defining a new disease? Cardiology 2012;123:15–23.22948714 10.1159/000339872 · doi ↗ · pubmed ↗
- 6Gans CP, Kao JA. Tricuspid regurgitation causing a right to left interatrial shunt with normal pulmonary pressures. Cardiology 2007;107:429–432.17310117 10.1159/000099654 · doi ↗ · pubmed ↗
- 7Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur J Cardiothorac Surg 2021;60:727–800.34453161 10.1093/ejcts/ezab 389 · doi ↗ · pubmed ↗