Latent Healthcare Stigma Profiles and Their Association With Human Immunodeficiency Virus (HIV) Treatment and Care Outcomes Among Women With HIV in the United States: An Intersectional Analysis
Jennifer P Jain, Nadra E Lisha, Jae Sevelius, Torsten B Neilands, Carol Dawson-Rose, Mallory O Johnson, Ayden Scheim, Bulent Turan, Adebola Adedimeji, Mirjam-Colette Kempf, Gypsyamber D’Souza, Michelle Floris-Moore, Seble Kassaye, Anandi Sheth, Azure Thompson

TL;DR
This study explores how different levels of healthcare stigma affect HIV treatment outcomes among women in the US, finding that high stigma is linked to worse health outcomes.
Contribution
The novel contribution is identifying distinct stigma profiles and their intersectional associations with HIV treatment outcomes among women with HIV.
Findings
Three stigma profiles were identified: high stigma (3%), low stigma (86%), and anticipated stigma (11%).
High stigma was strongly associated with suboptimal HIV treatment outcomes and mental health issues.
Low stigma was linked to better adherence to antiretroviral therapy and lower viral nonsuppression.
Abstract
Stigma is a barrier to human immunodeficiency virus (HIV) care among women with HIV (WWH) in the United States (US). We estimated associations between latent stigma profiles and HIV outcomes among WWH in the Women's Interagency HIV Study. From 2018 to 2019, participants (N = 1407) completed semi-annual assessments on sociodemographics, substance use, HIV-related, anticipated, and race-related stigma in healthcare, and suboptimal antiretroviral therapy adherence (<95%), and underwent HIV RNA testing. Latent profile analysis and multinomial logistic regression were used to examine adjusted associations between profiles and several covariates. Structural equation modeling estimated longitudinal associations between profiles, suboptimal adherence, and viral nonsuppression (HIV-1 RNA ≥20 copies/mL). We identified 3 profiles: high stigma (3%), low stigma (86%), and anticipated stigma (11%).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
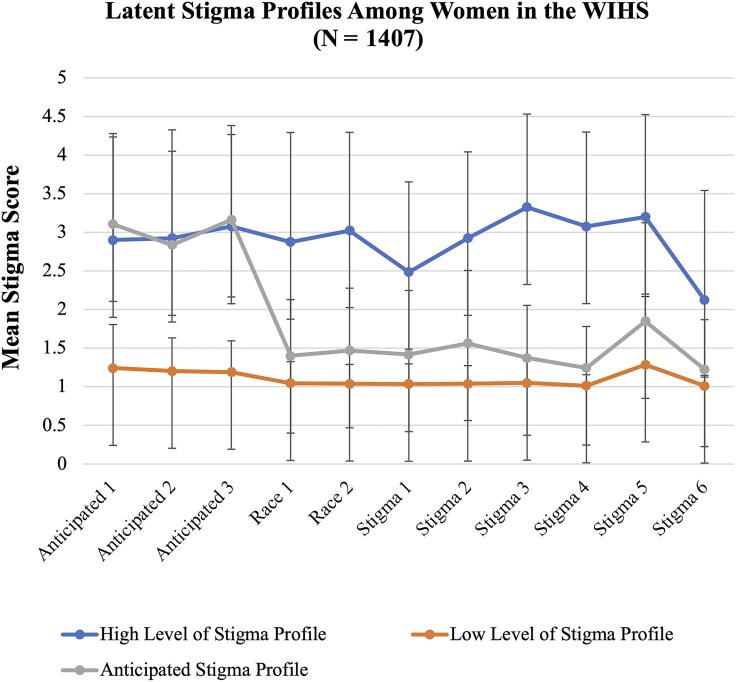 Figure 1
Figure 1| Classes (Items) | N1 | N2 | N3 | N4 | N5 | N6 | BIC | BLRT | VLMRT | Entropy |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1407 | … | … | … | … | … | 29 451.66 | … | … | … |
| 2 | 1318 | 89 | … | … | … | … | 24 667.02 | 0.00 | 0.0987 | 0.994 |
| 3 | 40 | 1207 | 160 | … | … | … | 22 777.17 | 0.00 | 0.1966 | 0.983 |
| 4 | 25 | 100 | 1200 | 82 | … | … | 21 641.24 | 0.00 | 0.6132 | 0.99 |
| 5 | 44 | 9 | 53 | 1207 | 94 | … | 19 974.56 | 0.00 | 0.2443 | 0.992 |
| 6 | 23 | 27 | 1196 | 44 | 105 | 12 | 17 957.08 | 0.00 | 0.7382 | 0.993 |
| Variable | Overall (N = 1407) | Profile 1: High Stigma | Profile 2: Low Stigma (Reference Profile) | Profile 3: Anticipated Stigma |
|
|
|---|---|---|---|---|---|---|
| Intersectional groupings based on drug use and race | .01 | .13 | ||||
| Non-Black women who do not use drugs | 249 (17.7%) | 4 (10.0%) | 219 (18.1%) | 26 (16.3%) | ||
| Non-Black women who use drugs | 96 (6.8%) | 6 (15.0%) | 74 (6.1%) | 16 (10.0%) | ||
| Black women who do not use drugs | 775 (55.1%) | 17 (42.5%) | 678 (56.2%) | 80 (50.0%) | ||
| Black women who use drugs | 287 (20.4%) | 13 (32.5%) | 236 (19.5%) | 38 (23.8%) | ||
| Sociodemographic factors | ||||||
| Age, y, mean (SE) | 38.68 (9.3) | 38.70 (1.5) | 38.89 (0.27) | 37.08 (0.73) | .99 | .05 |
| Average annual income | .76 | .10 | ||||
| ≤$24 000 on average annually | 980 (72.9%) | 29 (74.4%) | 838 (72.1%) | 123 (78.3%) | ||
| >$24 000 on average annually | 364 (27.1%) | 10 (25.6%) | 320 (27.9%) | 34 (21.7%) | ||
| Married | .39 | .66 | ||||
| No | 1093 (79.7%) | 29 (74.4%) | 940 (80.0%) | 124 (78.5%) | ||
| Yes | 279 (20.3%) | 10 (25.6%) | 235 (20.0%) | 34 (21.5%) | ||
| Employed | .02 | .01 | ||||
| No | 883 (63.8%) | 32 (80.0%) | 736 (61.0%) | 115 (71.8%) | ||
| Yes | 524 (37.2%) | 8 (20.0%) | 471 (39.0%) | 45 (28.1%) | ||
| Education | .62 | .21 | ||||
| Less than high school | 450 (32.0%) | 14 (35.0%) | 378 (31.3%) | 58 (36.2%) | ||
| High school or more | 956 (68.0%) | 26 (65.0%) | 828 (68.7%) | 102 (63.8%) | ||
| Unstably housed | .43 | .70 | ||||
| No | 1252 (89.0%) | 34 (85.0%) | 1074 (89.0%) | 144 (90.0%) | ||
| Yes | 155 (11.0%) | 6 (15.0%) | 133 (11.1%) | 16 (10.0%) | ||
| Race/Ethnicity | ||||||
| White, non-Hispanic | 139 (9.9%) | 4 (10.0%) | 119 (9.8%) | 16 (10.0%) | .14 | .05 |
| White, Hispanic | 65 (4.6%) | 1 (2.5%) | 60 (5.0%) | 4 (2.5%) | ||
| Black/African American, non-Hispanic | 1035 (73.6%) | 30 (75.0%) | 890 (73.7%) | 115 (71.9%) | ||
| Black/African American, Hispanic | 27 (1.9%) | 0 (0.0%) | 24 (2.0%) | 3 (1.9%) | ||
| Other, Hispanic | 98 (7.0%) | 2 (5.0%) | 84 (7.0%) | 12 (7.5%) | ||
| Asian/Pacific Islander | 6 (0.9%) | 0 (0.0%) | 3 (0.2%) | 3 (1.9%) | ||
| Native American/Native Alaskan | 13 (0.9%) | 2 (5.0%) | 8 (0.7%) | 3 (1.9%) | ||
| Other | 24 (1.7%) | 1 (2.5%) | 19 (1.6%) | 4 (2.5%) | ||
| HIV treatment and care in the past 6 mo | ||||||
| Suboptimal adherence to ART | .04 | .35 | ||||
| No | 1119 (84.8%) | 27 (73.0%) | 969 (85.5%) | 123 (82.5%) | ||
| Yes | 201 (15.2%) | 10 (27.0%) | 165 (14.5%) | 26 (17.5%) | ||
| Virally nonsuppressed | .44 | .88 | ||||
| No | 967 (71.3%) | 25 (65.8%) | 832 (71.6%) | 110 (70.1%) | ||
| Yes | 389 (28.7%) | 13 (34.2%) | 331 (28.4%) | 45 (29.0%) | ||
| Time on ART | 7.89 (5.2) | 9.24 (0.82) | 7.76 (0.15) | 8.51 (0.41) | .18 | .20 |
| Substance use and related factors in the past 6 mo | ||||||
| Heavy drinking | .76 | .38 | ||||
| No | 1313 (93.4%) | 37 (92.5%) | 1129 (93.7%) | 147 (91.9%) | ||
| Yes | 92 (6.6%) | 3 (7.5%) | 76 (6.3%) | 13 (8.1%) | ||
| Any drug use | .00 | .03 | ||||
| No | 1024 (72.8%) | 21 (52.5%) | 897 (74.3%) | 106 (66.2%) | ||
| Yes | 383 (27.2%) | 19 (47.5%) | 310 (25.7%) | 54 (22.8%) | ||
| Marijuana use | .02 | .03 | ||||
| No | 1106 (78.7%) | 26 (65.0%) | 964 (80.0%) | 116 (72.5%) | ||
| Yes | 299 (21.3%) | 14 (35.0%) | 241 (20.0%) | 44 (27.5%) | ||
| Crack cocaine use | .39 | .20 | ||||
| No | 1337 (95.1%) | 37 (92.5%) | 1151 (95.4%) | 149 (93.1%) | ||
| Yes | 69 (4.9%) | 3 (7.5%) | 55 (4.6%) | 11 (6.9%) | ||
| Cocaine use | .56 | .90 | ||||
| No | 1359 (96.7%) | 38 (95.0%) | 1166 (96.7%) | 155 (96.9%) | ||
| Yes | 47 (3.3%) | 2 (5.0%) | 40 (3.3%) | 5 (3.1%) | ||
| Heroin use | .14 | .33 | ||||
| No | 1396 (99.3%) | 39 (97.5%) | 1199 (99.4%) | 158 (98.8%) | ||
| Yes | 47 (3.3%) | 1 (2.5%) | 7 (0.6%) | 2 (1.2%) | ||
| Noninjection drug use | .01 | .00 | ||||
| No | 1058 (75.3%) | 24 (60.0%) | 925 (76.7%) | 109 (68.1%) | ||
| Yes | 348 (24.7%) | 16 (40.0%) | 281 (23.3%) | 51 (31.9%) | ||
| Enrolled in an opioid use treatment program | .00 | .66 | ||||
| No | 1360 (96.7%) | 35 (87.5%) | 1169 (96.9%) | 156 (97.5%) | ||
| Yes | 47 (3.3%) | 5 (12.5%) | 38 (3.1%) | 4 (2.5%) | ||
| Ever engaged in sex work | .40 | .55 | ||||
| No | 934 (66.5%) | 24 (60.0%) | 800 (66.4%) | 110 (68.8%) | ||
| Yes | 471 (33.5%) | 16 (40.0%) | 405 (33.6%) | 50 (31.2%) | ||
| Mental health/psychosocial factors in the past 6 mo | ||||||
| At risk of clinical depression | <.0001 | <.0001 | ||||
| No | 957 (68.2%) | 12 (31.6%) | 865 (71.8%) | 80 (50.0%) | ||
| Yes | 446 (31.8%) | 26 (68.4%) | 340 (28.2%) | 80 (50.0%) | ||
| PTSD | <.0001 | .00 | ||||
| Little or no PTSD symptoms (score 17–27) | 763 (56.2%) | 9 (22.5%) | 679 (58.6%) | 75 (47.2%) | ||
| Some PTSD symptoms (score 28–29) | 74 (5.4%) | 3 (7.5%) | 65 (5.6%) | 6 (3.8%) | ||
| Moderate PTSD symptoms (score 30–44) | 308 (22.8%) | 10 (25.0%) | 260 (22.4%) | 38 (23.9%) | ||
| High PTSD symptoms (score 45–85) | 212 (15.6%) | 18 (45.0%) | 154 (13.4%) | 40 (25.2%) | ||
| Perceived stress score | 16.84 (7.49) | 21.22 (1.18) | 16.46 (0.22) | 18.49 (0.59) | .00 | .00 |
| Trust in HIV care providers score | 3.44 (0.41) | 3.42 (0.81) | 3.46 (0.93) | 3.39 (0.13) | .81 | .13 |
| Resilience score | 4.03 (0.73) | 3.77 (0.12) | 4.06 (0.02) | 3.82 (0.06) | .03 | .00 |
| Variable | Profile 1: |
| Profile 3: |
|
|---|---|---|---|---|
| Intersectional groupings | ||||
| Black women who do not use drugs | 1.70 (.55–5.20) | .36 | 1.12 (.69–1.82) | .66 |
| Black women who use drugs | 3.67 (1.12–12.10) | .03 | 1.45 (.83–2.54) | .19 |
| Non-Black women who use drugs | 4.88 (1.32–18.00) | .02 | 1.75 (.87–3.52) | .11 |
| Non-Black women who do not use drugs (reference class) | … | … | ||
| Suboptimal adherence to ART | 2.29 (1.08–4.86) | .04 | 1.24 (.78–1.96) | .37 |
| Any drug use | 2.65 (1.38–5.11) | .003 | 1.40 (.97–2.01) | .07 |
| Marijuana use | 2.16 (1.08–4.32) | .03 | 1.44 (.98–2.11) | .06 |
| Noninjection drug use | 2.26 (1.15–4.42) | .02 | 1.49 (1.03–2.15) | .03 |
| Enrolled in opioid use treatment | 4.07 (1.47–11.26) | .006 | 0.69 (.24–1.97) | .49 |
| At risk of clinical depression | 5.84 (2.85–11.97) | <.0001 | 2.58 (1.82–3.65) | <.0001 |
| Employed | 0.36 (.15–.87) | .02 | 0.60 (.39–.91) | .02 |
| Resilience score | 0.59 (.39–.91) | .01 | 0.65 (.52–.81) | .0002 |
| Perceived stress score | 1.09 (1.05–1.14) | <.0001 | 1.04 (1.01–1.06) | .003 |
| High PTSD | 10.63 (4.38–25.79) | <.0001 | 2.43 (1.56–3.78) | <.0001 |
| Moderate PTSD | 3.07 (1.22–7.74) | .02 | 1.33 (.87–2.05) | .19 |
| Some PTSD | 4.41 (1.14–17.06) | .03 | 0.90 (.37–2.17) | .81 |
| Little or no PTSD (reference class) | … | … |
- —National Heart, Lung, and Blood Institute10.13039/100000050
- —Eunice Kennedy Shriver National Institute of Child Health and Human Development10.13039/100009633
- —National Institute on Aging10.13039/100000049
- —National Institute of Dental and Craniofacial Research10.13039/100000072
- —National Institute of Allergy and Infectious Diseases10.13039/100000060
- —National Institute of Neurological Disorders and Stroke10.13039/100000065
- —National Institute of Mental Health10.13039/100000025
- —National Institute on Drug Abuse10.13039/100000026
- —National Institute of Nursing Research10.13039/100000056
- —National Cancer Institute10.13039/100000054
- —National Institute on Alcohol Abuse and Alcoholism10.13039/100000027
- —National Institute on Deafness and Other Communication Disorders10.13039/100000055
- —National Institute of Diabetes and Digestive and Kidney Diseases10.13039/100000062
- —National Institute on Minority Health and Health Disparities10.13039/100006545
- —National Institutes of Health10.13039/100000002
- —Office of AIDS Research10.13039/100006084
- —University of California, San Francisco xxx [CTSA]
- —Johns Hopkins University Institute for Clinical and Translational Research
- —University of California, Los Angeles Clinical and Translational Science I
- —Atlanta Center for AIDS Research
- —Miami CFAR
- —UNC CFAR10.13039/100011072
- —UAB CFAR10.13039/100019610
- —Miami Center for HIV and Research in Mental Health
- —DC CTSA
- —DC CTSA
- —DC CTSA
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV, Drug Use, Sexual Risk · LGBTQ Health, Identity, and Policy
In the era of treatment as prevention (TasP), optimal adherence to antiretroviral therapy (ART) is vital to attaining human immunodeficiency virus (HIV) viral suppression and preventing the onward transmission of HIV [1]. Despite advances in HIV treatment, troubling disparities in HIV treatment outcomes persist among women with HIV (WWH) who use drugs and Black WWH in the United States (US) [2–8]. Black WWH are disproportionately affected by structural barriers to HIV care, including limited access to culturally tailored healthcare services and racial discrimination [9]. These barriers may be more intensified among Black WWH who use drugs, because they experience overlapping stigmas related to their HIV status, race, and drug use [10]. These intersecting forms of stigma are known to contribute to lower rates of engagement in HIV care, adherence to ART, and viral suppression. For example, WWH who use drugs have an 87% higher prevalence of suboptimal adherence to ART compared to WWH who do not use drugs [11]. Similarly, Black WWH report significantly lower rates of adherence compared to other ethnoracial groups, and their mortality rate due to HIV is 17 times higher than that of White WWH [6–8].
Intersectionality is a critical theoretical framework that highlights how systems of power and privilege—including sexism, racism, and substance use–related stigma—create and reinforce social inequities, while acknowledging resilience and resistance to stigma [12–14]. Intersectional stigma and discrimination continue to drive inequalities in HIV treatment outcomes among WWH who use drugs and Black WWH through inhibiting optimal engagement in HIV care [15–20]. Intersectional stigma and discrimination are defined as polices, practices, and behaviors that marginalize stigmatized individuals and perpetuate health inequities [12, 21]. Specifically, among WWH who use drugs, racism, sexism, HIV stigma, and substance use stigma often lead to suboptimal ART adherence and viral nonsuppression through an escalation of harmful drug use and healthcare avoidance [10, 15, 22–26]. On the contrary, resilience is a critical resource that may moderate stigma's impact on HIV care among WWH who use drugs and Black WWH; however, its role in this context remains understudied [27–29].
To alleviate the burden of HIV among WWH who use drugs and Black WWH, it is essential to mitigate the impact of intersectional stigma and discrimination and enhance resilience [30]. To do this, research with clear theoretical linkages to intersectionality is needed. Further, when utilizing data from racially diverse cohorts of WWH with varying patterns of drug use, there is a need to identify similar subpopulations based on their endorsement of different stigmas in healthcare settings to understand how distinct stigma profiles differentially predict HIV treatment outcomes across multiple axes of discrimination based on drug use and race. In addition, there is a need to understand how distinct profiles differentially predict inequalities in HIV treatment outcomes over time using longitudinal models [31].
To address these gaps in research, we used a latent profile analysis (LPA) in conjunction with a longitudinal path model as recommended by prominent experts focused on intersectionality in quantitative research [32, 33]. These methods were applied to evaluate how distinct stigma profiles differentially predict suboptimal adherence, and then how suboptimal adherence predicts viral nonsuppression across intersections of drug use and race among US WWH. This person-centered approach evaluates intersectionality by treating different patterns of experienced stigmas as latent empirically determined constructs, while incorporating a social grouping predictor variable that spans multiple axes of discrimination [33]. We hypothesized that profiles characterized by higher levels of stigma would be associated with suboptimal adherence and viral nonsuppression, and that WWH who use drugs and Black WWH who use drugs will be more likely to be in profiles defined by higher levels of stigma. For the longitudinal component, we hypothesized that profiles defined by stigma would predict suboptimal adherence and suboptimal adherence would in turn predict future viral nonsuppression. As such, this research may shed light on how oppression at the intersections of drug use and race among US WWH, stigma, and HIV care outcomes interact, offering insights to inform public health programs and policies that promote intersectional equity and TasP among WWH [34–37].
METHODS
Study Population
The Women's Interagency HIV Study (WIHS) established in 1994, is the oldest and largest ongoing prospective cohort study of women with HIV and sociodemographically similar women without HIV in the US [38]. It is now integrated with the Multicenter AIDS Cohort Study (MACS) and has become the MACS/WIHS Combined Cohort Study (MWCCS). Women are recruited into the MWCCS through several outreach strategies conducted at clinical sites and community settings across the US. MWCCS enrolls WWH as well as demographically similar women without HIV. Participants are identified through HIV clinics, community-based organizations, and word-of-mouth referrals. The cohort is designed to reflect the demographic profiles of women affected by HIV across the US, with extra effort placed on recruiting underserved women.
This study leveraged WIHS data collected among women with HIV only; women without HIV were excluded from the present study. Data collected between 1 April 2018 and 30 September 2019 were utilized for this study. Data from the following sites were leveraged for the present study/analysis: the Bronx and Brooklyn, New York; Chicago, Illinois; San Francisco, California; Los Angeles, California; Washington, District of Columbia; Atlanta, Georgia; Chapel Hill, North Carolina; Miami, Florida; Jackson, Mississippi; and Birmingham, Alabama.
Study Procedures
WIHS procedures and protocols are described fully elsewhere [38]. In brief, data on sociodemographics, substance use, stigma, mental health, and HIV treatment and care were collected semiannually, via an interview-administered questionnaire. Women underwent HIV viral load testing every 6 months. For this analysis, one's baseline visit was considered the first visit on record during the study period, which includes 3 visits (visits 48, 49, and 50). Participants were not required to complete all 3 study visits (visits 48–50) to be included in the analysis. Participants provided written informed consent, and study activities took place in a private setting. Study procedures were approved by the institutional review boards at each site.
Measures
Experienced Stigmas in Healthcare Settings
We used validated measures of experienced HIV-related stigma, race-related stigma, and anticipated stigma in healthcare settings at visit 48. We assessed anticipated HIV-related stigma using a 3-item measure and subscale from the HIV Stigma Framework Scale [39] (eg, “Healthcare workers will not listen to my concerns”) and a Likert response scale (1 = very unlikely to 5 = very likely); the Cronbach coefficient was α = .89. We assessed experienced race-related stigma or implicit racial bias in healthcare settings using a 2-item measure from the discrimination subscale of the Interpersonal Processes of Care Survey [40] (eg, “In the past 12 months, how often did you feel discriminated against by healthcare workers because of your race or ethnicity?”) and a Likert scale (1 = never to 5 = almost always); the Cronbach coefficient was α = .86. We measured experienced HIV-related stigma using a 6-item measure adapted from the experienced stigma subscale measuring HIV-related stigma among health facility staff [41] (eg, “Healthcare workers disclosed or told your HIV status to others without your permission”) and the same Likert scale; the Cronbach coefficient was α = .81. All stigma items are displayed in Figure 1.
This figure illustrates the separation between each latent profile and homogeneity within each profile. The mean stigma score for each type of stigma is plotted, along with standard errors to show the variability around each mean score. Here are the items for each stigma measure: Anticipated HIV Stigma in Healthcare Setting, 1–3: (1) “Healthcare workers will not listen to my concerns”; (2) “Healthcare workers will avoid touching me”; and (3) “Healthcare workers will treat me with less respect.” Experienced Race-Related Stigma in Healthcare Settings, 1–2: (1) “In the past 12 months, how often did healthcare workers pay less attention to you because of your race or ethnicity?” and (2) “In the past 12 months, how often did you feel discriminated against by healthcare workers because of your race or ethnicity?” Experienced HIV Stigma in Healthcare Settings, 1–6: (1) “Healthcare workers were unwilling to care for you because you are living with HIV”; (2) “Healthcare workers provided poorer quality of care to you than to other patients because you are living with HIV”; (3) “Healthcare workers talked badly about people living with HIV”; (4) “Healthcare workers disclosed or told your HIV status to others without your permission”; (5) “Healthcare workers used extra infection control precautions (like wearing extra gloves) when caring for you because you are a person living with HIV”; and (6) “Healthcare workers sent or referred you to another health facility because the workers do not want to treat you there.” Abbreviations: HIV, human immunodeficiency virus; WIHS, Women's Interagency HIV Study.
Sociodemographics
Sociodemographic factors utilized for this study include employed (yes/no), education (high school or more vs less than high school), age in years, average annual income ( >24 000), married (yes/no), and unstably housed (yes/no).
Intersectional Groupings
Data on race and drug use were used to create 4 intersectional groupings as predictors of profile membership. A dichotomous measure of any drug use (yes/no) was created by placing those who reported using any of the following drugs in the past 6 months in the drug use category: cannabis, methamphetamine, cocaine, crack cocaine, heroin, nonprescribed prescription opioids, ecstasy, phencyclidine or angel dust, psychedelics, poppers (alkyl nitrites), and nonprescribed benzodiazepines or barbiturates. A dichotomous measure of race, Black versus non-Black, was created to avoid data sparsity issues, as the majority (75%) identified as Black. From these variables, a categorical variable with 4 intersectional groupings was created: (1) non-Black women who do not use drugs (reference group); (2) non-Black women who use drugs; (3) Black women who do not use drugs; and (4) Black women who use drugs.
HIV Treatment/Care
Adherence to ART was measured by asking participants to report how often they took their HIV medications as prescribed in the past 6 months (100% of the time; 95%–99% of the time; 75%–94% of the time; <75% of the time). Based on these responses, we created a dichotomous measure of suboptimal adherence to ART (yes/no), defined as reporting <95% [42–44]. In addition, a dichotomous measure of viral nonsuppression (yes/no), was created using a cutoff of HIV-1 RNA ≥20 copies/mL, as viral suppression is defined as levels below the lower limit of detection of the HIV RNA assay, which is 20 copies/mL in the MWCCS. Viral load measurement corresponds to the time of each study visit.
Substance Use
As noted above, we created a variable for any drug use in the past 6 months. We also collected data on any noninjection drug use (yes/no); heavy drinking (yes/no), defined as consuming >7 drinks per week; and enrollment in opioid treatment (yes/no), in the past 6 months.
Mental Health
Using the Center for Epidemiological Studies Depression Scale [45] and a cutoff of 16, we created a binary variable for being at risk of clinical depression (yes/no). We measured stress using the Perceived Stress Scale–10 [46]; scores range from 0 to 40, and higher scores indicate higher levels of stress. Trust in one's HIV care provider was assessed using the Safran Physician Trust Subscale [47]. Resilience was measured using the Conner-Davidson Resilience Scale [48], where participants responded to 10 statements about personal resilience using a Likert scale (1 = not true at all to 5 = true nearly all the time). All of these variables were collected across the entire study period. PTSD symptoms were assessed using the 17-item Civilian PTSD Checklist (PCL-C), which is designed for the general population. Participants were asked to rate how bothered they were by each symptom in the past month using a 5-point Likert scale ranging from 1 (“Not at all”) to 5 (“Extremely”). Total scores range from 17 to 85, with higher scores indicating higher levels of PTSD symptom severity. Scores were categorized into four severity levels: little or no PTSD symptoms: 17–27, some PTSD symptoms: 28–29, moderate PTSD symptoms: 30–44 and high PTSD symptoms: 45–85 [49].
Statistical Analyses
Latent Profile Analysis
We conducted a LPA using cross-sectional data from visit 48 to identify similar subgroups of women based on their endorsement of (1) experienced HIV-related stigma in healthcare settings; (2) experienced race-related stigma in healthcare settings; and (3) anticipated stigma in healthcare settings. LPA identifies unobserved subgroups by examining observed response patterns from continuous indicators. Since there were only 3 subscales, rather than using summary scores, we utilized individual items from each stigma subscale for the LPA. We fit between 1 and 6 LPA models and selected the 3-profile model as the final solution based on fit indices including Bayesian information criterion (BIC), bootstrapped likelihood ratio test, Vuong-Lo-Mendell-Rubin likelihood ratio test (VLMRT), and entropy, as well as practical considerations such as profile size and the interpretability or the meaningfulness of the profiles (Table 1) [50–52]. Although BIC values continued to decrease with additional classes, improvement plateaued after the 3-class model (BIC, 22 777.2 vs 24 667.0 for the 2-class model). The 3-class solution showed acceptable entropy (0.983), indicating strong classification certainty. Although the VLMRT P value was not significant (P = .1966), models with 4 or more classes produced small, potentially unstable groups (eg, only 9 individuals in 1 class), raising concerns about overfitting. Thus, we selected the 3-class model as the most parsimonious and conceptually meaningful solution. Participants were assigned to their most likely latent class based on posterior probabilities derived from the LPA. Although this approach does not explicitly account for classification uncertainty, the model entropy was high (1.00), indicating strong class separation and high confidence in class assignment. While not incorporating uncertainty in class membership can lead to underestimated standard errors in downstream analyses, the high entropy and clear profile distinctions support the appropriateness of this approach for the current study. Figure 1 illustrates the separation between each profile and homogeneity within each profile.
Descriptive Analysis
We analyzed the distribution of several covariates across the 3 profiles to identify those that varied significantly. The χ^2^ test was used for categorical and binary variables, while t test was employed for continuous variables, with a significance threshold of P < .05 (Table 2). Covariates that showed significant variation across profiles were subsequently included in the multinomial regression analysis to explore the relationship between profile membership and these covariates (Table 3). The covariates of interest included intersectional groupings based on race and drug use, suboptimal adherence and viral nonsuppression, substance use, substance use treatment, sex work, depression, stress, posttraumatic stress disorder (PTSD), and resilience.
Multinomial Logistic Regression
To examine the association between profile membership and the covariates of interest, we built a series of multinomial logistic regression models. Each covariate was modeled separately, and we report the total effects of each exposure on the outcome. All models were adjusted for age in years, time on ART, education, income, and marital status. These variables were selected based on prior MWCCS research identifying them as correlates of HIV treatment and care outcomes, and were conceptualized as confounders in our analysis [54]. Analyses were completed using SAS version 9.4 software.
Longitudinal Analysis
To measure changes over time and account for temporal ordering, we leveraged the longitudinal data structure and analyzed how distinct stigma profiles at visit 48 differentially predicted suboptimal adherence at visit 49, and how suboptimal adherence predicted viral nonsuppression at visit 50, using a structural equation model. Specifically, we used significant predictors (P < .05) from the multinomial regression results (at visit 48) to predict latent stigma profile membership at visit 48, and then used latent stigma profile membership to predict suboptimal adherence at visit 49 to see if latent stigma profile membership impacted suboptimal adherence. Finally, the model assessed how suboptimal adherence at visit 49 predicted viral nonsuppression at visit 50. These models controlled for the same confounders listed above. To address missing data and provide more robust and reliable estimates, multiple imputation was performed using Bayesian estimation with an unrestricted model [55]. Analyses were performed using Mplus version 8.11.
RESULTS
A total of 1407 WWH were included in this analysis, of whom 10% were non-Hispanic White, 5% were Hispanic White, 73% were non-Hispanic Black, 2% were Hispanic Black, 7% were other Hispanic, 0.4% were Asian/Pacific Islander, 0.9% were Native American/Native Alaskan, and 1.7% identified as another race/ethnicity. Regarding intersectional groupings, 55% were Black women who do not use drugs, 20% were Black women who use drugs, 18% were non-Black women who do not use drugs, and 7% were non-Black who use drugs. The mean age was 38.7 years (standard deviation [SD], 9.3 years), the majority (72%) reported earning ≤$24 000 on average annually, most (79%) were not married, many were unemployed (63%), and 68% completed high school or more. Everyone reported a history of incarceration, 33% reported a history of sex work, and nearly all (89%) reported being stably housed. Only 15% reported suboptimal adherence to ART, 28% were virally unsuppressed, and the mean time on ART was 7.9 years (SD, 5.2 years). At visit 48, 28.73% of participants were virally nonsuppressed; this increased slightly to 29.12% at visit 49 and declined to 25.94% at visit 50. Transitions in viral suppression status between visits revealed that some participants moved from viral suppression to viral nonsuppression and vice versa, indicating fluctuation in HIV treatment outcomes over time.
Few women (6%) reported heavy drinking, over a quarter (27%) reported any drug use, 24% reported any noninjection drug use, 21% reported cannabis use, 4% reported crack cocaine use, 3% reported cocaine use, 3% reported heroin use, and very few (3%) reported being enrolled in an opioid treatment program. Many (30%) were at risk of clinical depression, the majority reported few or no PTSD symptoms (56%), followed by moderate symptoms (22%), high symptoms of PTSD (15%), and some symptoms (5%). The mean perceived stress score was 16 (standard error [SE], 7), indicating a moderate level of stress overall; the mean trust in HIV care providers score was 3 (SE, 0.4) indicating a moderate level of trust overall; and the mean resilience score was 4 (SE, 0.7), indicating an average level of resilience in relation to population norms.
Latent Profile Analysis
We identified 3 profiles of WWH based on their endorsement of experienced HIV-related stigma, race-related stigma, and anticipated stigma in healthcare settings. Profile 1 was characterized by a high level of stigma in healthcare settings overall (3%), profile 2 was characterized by a low level of stigma in healthcare settings overall (86%), and profile 3 was characterized by anticipated stigma in healthcare settings (11%).
Compared to the low stigma profile, a significantly greater proportion of women in the high stigma profile reported being Black WWH who use drugs (32% vs 19%) or non-Black WWH who use drugs (15% vs 6%), any drug use (47% vs 25%), suboptimal ART adherence (27% vs 14%), and enrollment in an opioid treatment program (12% vs 3%). Compared to the low stigma profile, a significantly greater proportion of women in the high stigma and anticipated stigma profiles reported being unemployed (80% vs 61% and 71% vs 61%), cannabis use (35% vs 20% and 27% vs 20%), noninjection drug use (40% vs 23% and 31% vs 23%), clinical depression (68% vs 28% and 50% vs 28%), and higher mean (SE) stress scores (21 [1.18] vs 16 [0.22] and 18 [0.59] vs 16 [0.22]). Finally, women in the low stigma profile had significantly higher levels of resilience compared to those in the high stigma profile and the anticipated stigma profile (4.06 [0.02] vs 3.77 [0.12] and 4.06 [0.02] vs 3.82 [0.06]) (Table 2).
Compared to the low stigma profile, the odds of membership in the high stigma profile were higher for Black WWH who use drugs, non-Black WWH who use drugs, and those who reported suboptimal adherence, any drug use, cannabis use, noninjection drug use, enrollment in a opioid treatment program, depression, higher stress levels, and any PTSD. Compared to membership in the low stigma profile, the odds of membership in the anticipated stigma profile were higher for those who reported; noninjection drug use, depression, higher levels of stress, and high PTSD. Women who were employed had a significantly lower odds of membership in the high stigma profile and the anticipated stigma profile compared to the low level of stigma profile. Similarly, those who reported higher levels of resilience had a significantly lower odds of membership in the high stigma profile and the anticipated stigma profile compared to the low level of stigma profile (Table 3).
Longitudinal Analysis Results
In the longitudinal model, which controlled for age, time on ART, education, income, and marital status, we found that depression (at baseline) was related to being in the anticipated stigma profile (adjusted odds ratio [aOR], 2.00 [95% confidence interval {CI}, 1.30–3.09]) and the high stigma profile (aOR, 2.94 [95% CI, 1.25–6.95]) versus the lower stigma profile. High PTSD (at baseline) (odds ratio [OR], 5.47 [95% CI, 1.37–21.83]) was related to being in the high level of stigma profile compared to the low level of stigma profile. Profile membership was related to suboptimal ART adherence, such that suboptimal adherence was lowest for those in the low level of stigma profile (profile 1 vs 2: OR, 0.46 [95% CI, .22–.96]; profile 3 vs 2: OR, 0.62 [95% CI, .41–.94]). Finally, suboptimal adherence at timepoint 2 predicted future viral nonsuppression at timepoint 3 (OR, 0.31 [95% CI, .22–.42]).
DISCUSSION
We identified several important findings in this large intersectional study examining subgroups of US WWH based on their endorsement of experienced stigmas in healthcare settings, and their association with suboptimal adherence and viral nonsuppression. While most women in our study reported a low level of stigma in healthcare settings overall, we did identify 2 socially and structurally marginalized groups of women defined by high levels of stigma and anticipated stigma. Our longitudinal path model revealed that these higher stigma profiles predicted suboptimal adherence, which in turn predicted viral nonsuppression. As such, we used longitudinal modeling to estimate the temporal relationships between stigma profiles, ART adherence, and viral nonsuppression, and moved beyond cross-sectional associations to model how stigma in healthcare settings contributes to downstream HIV treatment and care outcomes. Altogether, these findings may help inform the development of multilevel interventions to optimize HIV treatment and intervention among US WWH who use drugs.
The high stigma profile was characterized by women who reported elevated levels of HIV-related, race-related, and anticipated stigma in healthcare settings. This profile had a higher prevalence of Black WWH who use drugs and non-Black WWH who use drugs. Additionally, women in this group were more likely to report drug use, opioid use treatment, suboptimal adherence to ART, depression, unemployment, higher levels of stress, PTSD, and lower levels of resilience, compared to women in the low stigma profile. Similarly, women who reported the following were more likely to be in the anticipated stigma profile: any noninjection drug use, poor mental health conditions, unemployment, and lower levels of resilience. These anticipated findings point to a clear relationship between different stigmas in healthcare settings and women who are multiply marginalized for drug use, poor adherence, psychological morbidity, and economic marginalization. Hence these findings highlight the need to combat stigma and deliver programs that integrate trauma-informed HIV care, substance use treatment, mental health support, and economic empowerment strategies among US WWH [56, 57]. Additionally, it is important to involve WWH with lived experience of stigma in healthcare settings in the design and implementation of such programs and to acknowledge how interlocking systems of power and privilege shape the experiences of WWH [37, 58–60].
Our finding that profiles defined by higher levels of stigma in healthcare settings predicted future suboptimal adherence, which in turn predicted future viral nonsuppression, was consistent with our main hypothesis, which predicted that women with higher levels of stigma would have worse HIV treatment outcomes. This model demonstrates that suboptimal adherence to ART mediates the relationship between stigma and viral nonsuppression, emphasizing that stigma is an important modifiable upstream factor in improving adherence, and ultimately, viral suppression among women. Furthermore, although some of the anticipated relationships in the longitudinal analysis were no longer significant—likely due to the inclusion of other variables that account for shared variance, thereby reducing the unique contribution of the initial predictor—depression and PTSD remained key factors in shaping the higher-risk groups' HIV outcomes. This highlights how interconnected forms of stigma are associated with psychological morbidity and impact HIV care. Altogether, these results suggest the need to challenge social power structures and systems that perpetuate these inequalities among US WWH, through progressive policy reform, and expanded access to integrated care models that comprehensively address HIV, mental health (eg, depression and trauma), and other relevant factors, including substance use and economic empowerment [37, 61, 62].
Integrated care models that address both HIV and substance use are increasingly recognized as essential to improve the health of people with HIV who use drugs. Innovative strategies including mobile health clinics, telehealth platforms, and peer-led outreach that reduce structural barriers, including stigma, transportation challenges, and disjointed service delivery, have been shown to improve health outcomes among individuals affected by both HIV and substance use. For example, low-barrier models that combine HIV care, substance use treatment, and mobile pharmacy access through community health workers have shown promise in improving health outcomes among people who are dually impacted by HIV and drug use [63]. In addition, recent research highlights the value of person-centered, human rights-based approaches that address the underlying social, economic, and political inequalities that drive health inequities among this population [64]. Altogether, there is growing consensus that integrated models grounded in shared decision-making, trauma-informed care, cultural responsiveness, and human rights, all of which align with the principles of harm reduction, are critical for sustaining long-term engagement in HIV care and substance use treatment. Our research contributes to this literature by underscoring the importance of integrated programs that specifically focus on WWH who use drugs that address the co-occurring challenges related to stigma, trauma, mental health, substance use, HIV, and economic marginalization.
This study has several limitations that should be considered. The data utilized for this study were collected between 1 April 2018 and 30 September 2019 and therefore may not be reflective of current trends among WWH in the US. Future studies are planned to utilize data collected more recently to explore the role of intersectional stigma and discrimination on inequalities in HIV treatment and care outcomes among racially diverse WWH in the US. Cross-sectional data were used to create the LPA, and therefore temporal relationships are unclear and causality cannot be determined. Although we controlled for several known correlates of HIV treatment and care outcomes among US women, it is possible that residual or unmeasured confounding affected our results. Latent variable approaches make several assumptions, including unobserved heterogeneity and local independence, and the accuracy of these methods can be affected by data sparsity. Given the small percentage of women in the high stigma profile, whether reflecting a true finding or potential underreporting, we recommend that future studies with larger samples of WWH be conducted to further assess experiences of healthcare stigma.
We acknowledge that this study did not analyze measures of social inequality or power, which are core constructs of intersectionality; therefore, our findings provide an incomplete understanding of how these factors shape the experiences of WWH. Similarly, substance use stigma was not measured; thus, our findings do not capture how this dimension of stigma relates to the profiles identified or the health outcomes assessed. Moreover, non-Black participants, including those of Hispanic ethnicity, may also experience discrimination, and these forms of stigma are important but could not be meaningfully disaggregated in our analysis due to sample size limitations. Nonprobability recruitment methods were used to recruit women into the WIHS, which affects the generalizability of our results to other populations of WWH in the US. Further, because women in the WIHS have regular access to HIV treatment and care and are being retained in a longitudinal cohort study, they may not be reflective of other WWH. We relied upon self-reported data of several sensitive variables including stigma, substance use, and adherence to ART, which are subject to social desirability bias. Due to small cell sizes for some combinations of variables, the CIs for some estimates are very wide.
CONCLUSIONS
Our study utilized a latent variable person-centered approach to characterize experiences of stigma in healthcare settings among a large, racially diverse cohort of US WWH. While prior research has examined individual forms of stigma in isolation, we used a latent profile analysis to understand how stigma experiences cluster and impact HIV treatment and care outcomes over time among women. Findings from this study highlight that stigma in healthcare settings functions as a barrier to HIV treatment and care, particularly for women who face multiple layers of marginalization. Among both Black and non-Black WWH who use drugs, stigma is strongly associated with suboptimal adherence and viral nonsuppression. Although overall stigma levels were lower among Black and non-Black WWH who do not use drugs, and there were no substantial differences between these groups in this regard, they are not immune to stigma's effects and may still experience other forms of discrimination or structural disadvantage that impact their HIV care. In contrast, stigma was markedly higher among women who use drugs, regardless of race, underscoring substance use as a critical axis of marginalization within healthcare settings.
To optimize viral suppression across these subgroups, efforts must prioritize decreasing stigma through cultural norms shifts and reducing structural barriers to HIV care. Additionally, programs that integrate HIV care, harm reduction services that address drug use, offer mental health support and economic empowerment strategies, especially for WWH who use drugs, may have a profound impact on improving HIV outcomes and advancing intersectional equity among US WWH. Taken together, this research may help inform the development of future interventions and guide resource allocation by highlighting the subgroups of women most at risk of poor HIV treatment and care outcomes and offering insights to inform targeted care strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Robbins RN, Spector AY, Mellins CA, Remien RH. Optimizing ART adherence: update for HIV treatment and prevention. Curr HIV/AIDS Rep 2014; 11:423–33.25304006 10.1007/s 11904-014-0229-5PMC 4268351 · doi ↗ · pubmed ↗
- 2Metsch L, Philbin MM, Parish C, Shiu K, Frimpong JA, Giang LM. HIV testing, care, and treatment among women who use drugs from a global perspective: progress and challenges. J Acquir Immune Defic Syndr 2015; 69:S 162–8.25978483 10.1097/QAI.0000000000000660 PMC 4710173 · doi ↗ · pubmed ↗
- 3Larney S, Mathers BM, Poteat T, Kamarulzaman A, Degenhardt L. Global epidemiology of HIV among women and girls who use or inject drugs: current knowledge and limitations of existing data. J Acquir Immune Defic Syndr 2015; 69:S 100–9.25978476 10.1097/QAI.0000000000000623 PMC 5023521 · doi ↗ · pubmed ↗
- 4Glick JL, Huang A, Russo R, et al ART uptake and adherence among women who use drugs globally: a scoping review. Drug Alcohol Depend 2020; 215:108218.32916450 10.1016/j.drugalcdep.2020.108218 PMC 7899784 · doi ↗ · pubmed ↗
- 5Sullivan KA, Messer LC, Quinlivan EB. Substance abuse, violence, and HIV/AIDS (SAVA) syndemic effects on viral suppression among HIV positive women of color. AIDS Patient Care STDS 2015; 29:S 42–8.25397666 10.1089/apc.2014.0278 PMC 4283071 · doi ↗ · pubmed ↗
- 6Anastos K, Schneider MF, Gange SJ, et al The association of race, sociodemographic, and behavioral characteristics with response to highly active antiretroviral therapy in women. J Acquir Immune Defic Syndr 2005; 39:537–44.16044004 · pubmed ↗
- 7Geter A, Sutton MY, Armon C, et al Trends of racial and ethnic disparities in virologic suppression among women in the HIV outpatient study, USA, 2010–2015. P Lo S One 2018; 13:e 0189973.29293632 10.1371/journal.pone.0189973 PMC 5749722 · doi ↗ · pubmed ↗
- 8Sharpe TT, Lee LM, Nakashima AK, Elam-Evans LD, Fleming PL. Crack cocaine use and adherence to antiretroviral treatment among HIV-infected Black women. J Community Health 2004; 29:117–27.15065731 10.1023/b:johe.0000016716.99847.9b · doi ↗ · pubmed ↗