Thoracoscopic pneumonectomy for massive haemoptysis secondary to chronic pulmonary vein stenosis post-atrial fibrillation ablation
Fumie Osuga, Kentaro Minegishi, Shunsuke Endo, Hiroyoshi Tsubochi

TL;DR
A man developed severe lung bleeding due to a rare complication after heart ablation surgery and required lung removal to resolve it.
Contribution
This case highlights the need for anatomical pulmonary resection in managing late-onset massive haemoptysis due to chronic pulmonary vein stenosis.
Findings
A 57-year-old man with chronic PV stenosis required left pneumonectomy after 18 months of post-ablation complications.
Pathological findings showed irreversible fibrosis of the PV intima leading to pulmonary congestion.
Surgical intervention successfully resolved the haemoptysis caused by long-term PV stenosis.
Abstract
Pulmonary vein (PV) stenosis is a rare but serious complication after transcatheter ablation for atrial fibrillation, potentially leading to massive haemoptysis. We present a case of severe PV stenosis resulting in haemoptysis. A 57-year-old man presented with haemoptysis 18 months after catheter ablation. His left PV was almost completely occluded and required the left pneumonectomy. Pathological examination revealed irreversible fibrosis of the PV intima, which led to pulmonary congestion. Surgical intervention resolved the haemoptysis. Anatomical pulmonary resection is required for massive haemoptysis caused by PV stenosis that occurs long after transcatheter ablation. Transcatheter ablation is a common and effective therapeutic strategy for atrial fibrillation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
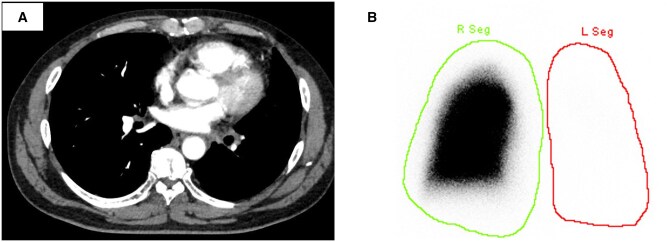 Figure 1
Figure 1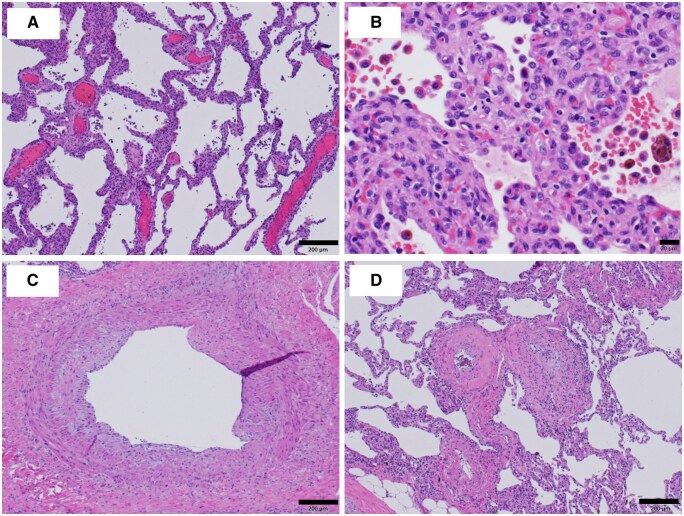 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Venous Thromboembolism Diagnosis and Management
INTRODUCTION
Transcatheter ablation is a common and effective therapeutic strategy for atrial fibrillation. Pulmonary vein (PV) stenosis is a rare complication of transcatheter ablation that can cause cough, dyspnoea, fatigue, and occasionally massive haemoptysis, though such severe cases are rarely reported. Severe PV stenosis caused by transcatheter ablation is sometimes irreversible and may require anatomical lung resection to control symptoms. Herein, we report a case treated with thoracoscopic left pneumonectomy for massive haemoptysis caused by severe PV stenosis following transcatheter ablation for atrial fibrillation.
CASE
We affirm this research adheres to the ethical standards and guidelines set by Jichi Medical University Saitama Medical Center and has received approval from Institutional Review Board (IRB) on 9 October 2024. The IRB approval number is S24-070. Informed consent was obtained from the patients in writing.
A 57-year-old man underwent transcatheter ablation for atrial fibrillation 18 months ago at another hospital. Three months after the procedure, the patient developed a persistent cough and fatigue. A chest X-ray revealed no abnormalities, so he was observed without further imaging. He presented to the emergency department with sudden haemoptysis. Computed tomography (CT) showed severe left superior and inferior PV stenosis (Figure 1A). Ventilation-perfusion scintigraphy showed that the left lung perfusion was severely diminished, receiving only 2% of the blood flow (Figure 1B).
Computed tomography showed severe stenosis of the left pulmonary vein (A). Ventilation-perfusion scintigraphy showed little or no blood flow in the left lung (B).
Thoracoscopic left pneumonectomy was performed. Operative findings showed enlarged PVs on the surface of the lung. Small vessels around the pulmonary ligament were also enlarged. The operation time was 288 minutes, and the blood loss was 327 mL. Microscopic examination of the lungs showed pulmonary congestion (Figure 2A), increased capillary growth, alveolar haemorrhage, and hemosiderin-laden macrophages (Figure 2B). The PVs from the centre (Figure 2C) to the capillaries (Figure 2D) had a narrowed lumen due to fibrous thickening of the intima. The bronchial arteries were not developed. The pleura showed dilation and enlargement of vessels, venous predominance, and lymphatic ducts. The preoperative PaO_2_/FiO_2_ ratio was 190, improving to 370 by the end of surgery. Symptoms improved postoperatively and were maintained for 1 year. During this period, we performed CT at 3 months, 6 months, and 1 year after surgery and confirmed that there were no abnormal findings.
The pathology showed congestion (A), capillary hyperplasia, alveolar haemorrhage, and hemosiderin-laden macrophages (B). Fibrous thickening of the pulmonary vein wall was present both centrally (C) and peripherally (D). Some pulmonary veins were obstructed (C, D).
DISCUSSION
Transcatheter ablation is an established treatment for atrial fibrillation when medical therapy fails to control symptoms. One of the serious complications is PV stenosis. Previous reports have placed the incidence of PV stenosis at 0%-42%. A recent review reported a mean incidence of 2% and a median incidence of 3.1%.1 The degree of PV stenosis is classified as mild if less than 50%, moderate if 50%-69%, and severe if 70% or greater.2 The severity of symptoms of PV stenosis is thought to depend on the degree of stenosis, cough, and dyspnoea are common, but haemoptysis is rare. Treatment for PV stenosis includes balloon dilatation or stenting, but recurrence rates remain high: 30%-87% (mean 60%) for balloon dilatation and 14%-57% (mean 34%) for stent placement.3
In our case, microvascular sclerosis was already complete. If severe stenosis of the large PV persists over time, the small PVs and small pulmonary arteries are also exposed to high pressure and become stenotic, leading to pulmonary congestion and alveolar haemorrhage.
Severe PV stenosis reduces pulmonary artery blood flow, which can be evaluated by pulmonary perfusion scintigraphy. If perfusion is severely diminished, lung resection may improve V/Q mismatch and lung function. If the PV stenosis is single or unilateral, lung resection can be a treatment option for haemoptysis. If all PVs are stenotic and resection is not possible, patching can be performed under cardiopulmonary support.4 In our case, the irreversible vascular changes led to reduced pulmonary blood flow, and pulmonary resection was performed which resulted in control of haemoptysis and improvement of respiratory status.
Currently, there are no guidelines for follow-up after ablation, but there is a report that it is desirable to perform imaging with CT or magnetic resonance imaging at 3-4 months is recommended.5 When PV stenosis occurs after ablation, the stenosis progresses gradually, and the longer the time between the occurrence of the stenosis and endovascular therapy, the less improvement in therapeutic efficacy has been reported.3 If severe PV stenosis persists over a long period of time, irreversible changes in the pulmonary artery and vein may occur, as in our case, and pulmonary resection may become necessary. Therefore, long-term imaging follow-up is important, though further case accumulation is needed to determine the optimal timing. At the very least, even in asymptomatic patients, CT should be considered at 3 and 6 months post-ablation, and promptly performed if symptoms develop.
In conclusion, if haemoptysis occurs long after PV stenosis after ablation, irreversible changes in PV may have occurred, and anatomical lung resection may be a treatment option.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rostamian A , Narayan SM, Thomson L, Fishbein M, Siegel RJ. The incidence, diagnosis, and management of pulmonary vein stenosis as a complication of atrial fibrillation ablation. J Interv Card Electrophysiol. 2014;40:63-74.24626996 10.1007/s 10840-014-9885-z · doi ↗ · pubmed ↗
- 2Saad EB , Rossillo A, Saad CP, et al Pulmonary vein stenosis after radiofrequency ablation of atrial fibrillation: functional characterization, evolution, and influence of the ablation strategy. Circulation. 2003;108:3102-3107.14623799 10.1161/01.CIR.0000104569.96907.7F · doi ↗ · pubmed ↗
- 3Luigi DB , Tamer SF, Oussama MW, et al Pulmonary vein total occlusion following catheter ablation for atrial fibrillation: clinical implications after long-term follow-up. J Am Coll Cardiol. 2006;48:2493-2499.17174188 10.1016/j.jacc.2006.08.038 · doi ↗ · pubmed ↗
- 4Hara H , Kanemitsu N, Hirao S, Itonaga T, Yamanaka K. Pulmonary vein reconstruction for pulmonary vein stenosis and occlusion after surgical ablation. Gen Thorac Cardiovasc Surg. 2021;69:1580-1584.34514539 10.1007/s 11748-021-01700-7 · doi ↗ · pubmed ↗
- 5Edriss H , Denega T, Test V, Nugent K. Pulmonary vein stenosis complicating radiofrequency catheter ablation for atrial fibrillation: a literature review. Respir Med. 2016;117:215-222.27492534 10.1016/j.rmed.2016.06.014 · doi ↗ · pubmed ↗