Effect of Socio-economic factors on malaria prevalence in a Peri-urban setting in Vihiga County, Western Kenya Highlands
Beatrice Aleyo Muzame, Elizabeth Omukunda, David Mulama, Patrick Okoth

TL;DR
This study explores how socio-economic factors affect malaria prevalence in a peri-urban area of Kenya, highlighting the need for household-level interventions.
Contribution
The study identifies specific socio-economic factors influencing malaria in a peri-urban Kenyan setting.
Findings
Socio-economic factors significantly influence malaria prevalence in the study area.
Education, wealth, land size, house type, and ventilation are key factors affecting malaria prevalence.
Abstract
Malaria is the leading cause of mortality in sub-Saharan Africa. The study assessed the effect of socio-economic factors on high malaria prevalence in a peri-urban setting in Vihiga County, Western Kenya highlands aimed at strengthening implementation of cost-effective malaria control strategies at household level. A longitudinal study was carried out in the study area from December 2019 to November 2020. From patients who presented themselves at Mbale Provincial Rural Training health centre for various treatments, 768 malaria confirmed patients were recruited and signed consent before the study commenced. Data was collected using microscopy and structured questionnaires used to stratify malaria patients into socio-economic status and their residence. Data was presented through graphs, frequency, analyzed using linear regression and correlation. P-value ≤ 0.05as considered…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
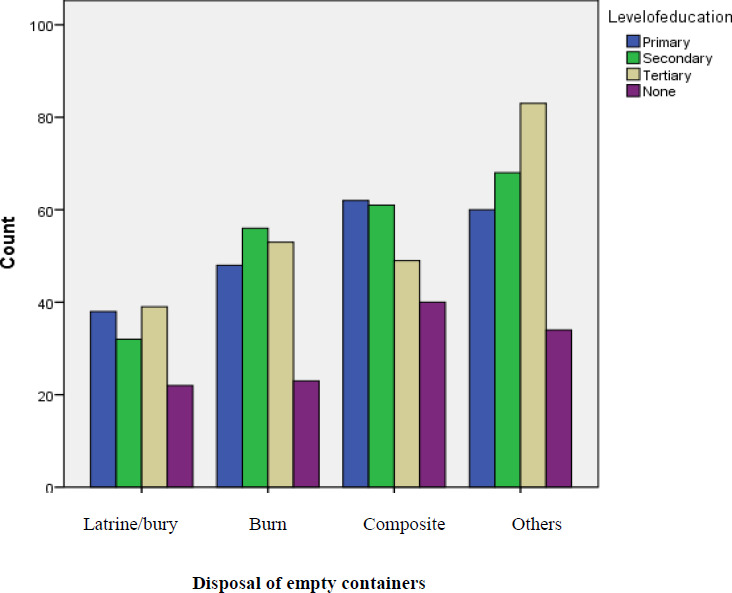 Figure 1
Figure 1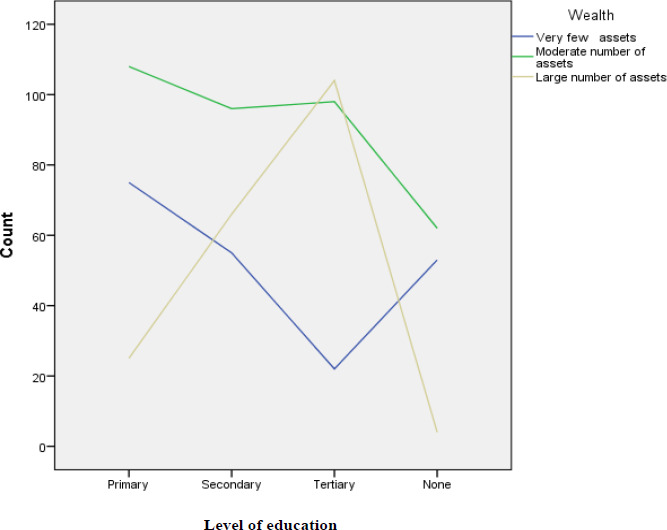 Figure 2
Figure 2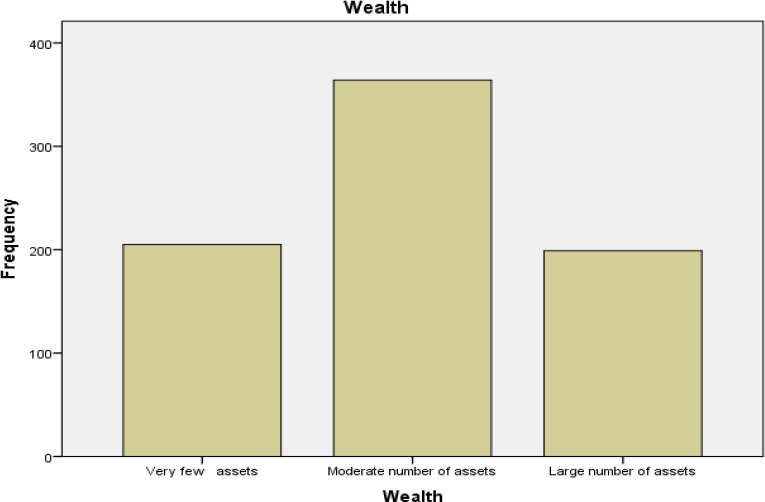 Figure 3
Figure 3| Coefficients | |||||
|---|---|---|---|---|---|
| Model | Unstandardized | Standardized | T | Sig. | |
| B | Std. | Beta | |||
| Constant) | 518.597 | 68.263 | 7.597 | .000 | |
| Level of education | 22.966 | 7.562 | .107 | 3.037 | .002 |
| Salary | 2.776 | 12.785 | .009 | .217 | .828 |
| Wealth | -53.833 | 12.264 | -.176 | -4.389 | .000 |
| Size of land | 15.507 | 5.592 | .099 | 2.773 | .006 |
| Household size | -.967 | 9.156 | -.004 | -.106 | .916 |
| House type | -37.786 | 10.441 | -.152 | -3.619 | .000 |
| Ventilation in the house | 37.454 | 18.883 | -.083 | -1.984 | .048 |
| Malaria | Level of Education | Wealth | Information on mosquito breeding grounds | ||
|---|---|---|---|---|---|
| Malaria | Pearson | 1 | .088 | -.158 | .079 |
| .014 | .000 | .028 | |||
| 768 | 768 | 768 | 768 | ||
| Level of education | Pearson | .088 | 1 | .062 | -.010 |
| .014 | .084 | .772 | |||
| 768 | 768 | 768 | 768 | ||
| Wealth | Pearson | -.158 | .062 | 1 | .028 |
| .000 | .084 | .447 | |||
| 768 | 768 | 768 | 768 | ||
| Information | Pearson | .079 | -.010 | .028 | 1 |
| .028 | .772 | .447 | |||
| 768 | 768 | 768 | 768 |
| Frequency | Valid Percent | Cumulative Percent | |
|---|---|---|---|
|
| |||
| High | 159 | 20.7 | 20.7 |
| Moderate | 395 | 51.4 | 72.1 |
| Low | 214 | 27.9 | 100 |
|
|
|
| |
|
| |||
| Two | 36 | 4.7 | 4.7 |
| Three | 86 | 11.2 | 15.9 |
| Four | 208 | 27.1 | 43 |
| More than four | 438 | 57 | 100 |
|
|
|
|
| Frequency | Valid Percent | Cumulative Percent | |
|---|---|---|---|
|
| |||
| Less than 1 acre | 237 | 30.9 | 30.9 |
| 1- 1.5 acres | 226 | 29.4 | 60.3 |
| 1.5 – 2 acres | 120 | 15.6 | 75.9 |
| More than 2 acres | 61 | 7.9 | 83.9 |
| Rented houses on | 124 | 16.1 | 100 |
| less than one acre | |||
| |
| 100 | |
|
| |||
| Primary | 208 | 27.1 | 27.1 |
| Secondary | 217 | 28.2 | 55.4 |
| Tertiary | 224 | 29.2 | 84.5 |
| No formal education | 119 | 15.5 | 100 |
|
|
|
|
| House Type | Frequency | Valid Percent | Cumulative Percent |
|---|---|---|---|
| Permanent (cemented floor/bricks/stone wall/iron/tile roof with ceiling boards) | 327 | 42.6 | 42.6 |
| Semi-permanent (mud floor mud walls/iron roofed | 309 | 40.2 | 82.8 |
| Semi-permanent (cemented floor/mud walls/iron roofed | 73 | 9.5 | 92.3 |
| Others (iron walls/roof/cemented floor) | 59 | 7.7 | 100 |
| |
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access
Background Information
Despite numerous global intervention strategies, malaria still remains the leading cause of morbidity and mortality in developing countries such as sub-Sahara Africa1, 2. A female Anopheles mosquito (Anopheles gambiae, A. arabiensis or A. funestus) takes in human blood meal and when infected with Plasmodium parasites, transmit them causing uncomplicated or severe malaria which kills a child every minute globally3,4. About 99% of malaria in Kenya is Plasmodium falciparum malaria while 1% of human malaria infection is caused by Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae2, 4, 5. Malaria targeted risk populations include; pregnant women, children below five years old, immunosuppressed patients such as those with HIV/AIDS, the aged and travellers to malaria endemic regions due to their low body immunity6. In Kenya, universal coverage with malaria prevention is yet to be achieved4,5. Malaria prevalence in Kenya was 5.08 in 2018, 5.02 million in 2019 and 3.66 million in 2020 with Western Kenya carrying most of the malaria burden where more than 70 % of the population in Western Kenya is at malaria risk4, 5. Vihiga County where the study area falls is a Lake endemic malaria zone5 and 28,786 patients across Vihiga County were diagnosed with malaria between January and March 2019 causing high mortality among children below 5 years old7. The study assessed the effect of socio-economic factors on high malaria prevalence in the study area aimed at strengthening implementation of cost-effective malaria control strategies at household level. There are no recorded documents specifically in the study area which have assessed effect of socio-economic factors on malaria prevalence yet socio-economic factors influence malaria prevalence according to ‘a malaria-free Kenya, Kenya Malaria Strategy- 2019-2023’ 5, hence the study.
Socio-economic factors refer to an individual's social and economic status in relation to other people in a given area4. A study carried out in Madhya Pradesh, India8 and in sub-Saharan Africa9, 10, 11 indicated that malaria burden can be reduced by improving people's socio-economic status. Studies carried out in sub-Saharan Africa10, 11 and in Assam, India12 reported that socio-economic factors that determine malaria transmission by influencing mosquito density3 and frequency of mosquito bites included; level of education, house structure, wealth, residence which can be in urban or rural areas, use of bed nets, household size, socio-cultural practices, stagnant water, vegetation, land use, time of fetching water for domestic use, nutrition which was linked to education and economic status and how far homes are from sources of water4. Perceptions and knowledge towards malaria infection and antimalarial compliance determines emergence of antimalarial resistance in malaria parasites which is closely associated with wealth and level of education1, 4. In Nigeria, socio-economic factors influenced malaria incidences in Calabar region13 and in Kwara14, where treatment and control of malaria attracted more financial and human resources. A study carried out in rural Uganda15 and in Chewaka district, Western Ethiopia16 indicated that inequalities in socio-economics affected malaria prevalence. Socio-economic status such as wealth, education and salary influences malaria prevalence as it determines the individual's knowledge and attitude towards malaria infection and control leading to malaria health inequalities as it was reported in study findings in lower North, Northern Tanzania17, and in Madhya Pradesh, Central India18. A malaria indicator survey was carried out in all 47 Counties in Kenya, which associated malaria prevalence with socio-economic factors which included; wealth, household size, house design and education4.
Wealth is the main socio-economic factor influencing malaria prevalence because it seems to influence other socio-economic factors4, 5, 6. Wealth in the study area was considered to be the income from various economic activities (type and quantity of crops grown, quality and quantity of livestock kept, fishing, brick making, mining and trading), salary, quantity and quality of assets such as type of the house, vehicle if any, television owned by the head of the household 9. In Assam, India, malaria was considered to be an infectious disease of poverty12, and an economic burden disease in Western Ethiopia16. Wealth can enable one to purchase enough insecticide-treated mosquito nets for all household members, build houses that can prevent entry of mosquitoes into the house, spray the house regularly with insecticides, buy original antimalarial drugs as counterfeits drugs can cause unavoidable malaria deaths and take his/her household members for malaria treatment early enough16, 18. A study carried out in Kenya showed that high level of poverty and low education level influenced malaria prevalence4, 5. Study findings on malaria from other parts of the world6 and from Kenya malaria indicator survey4 proved that poverty can led to malaria patients avoiding health facilities but instead engaged in; self-antimalarial prescription without laboratory test for malaria, failed to adhere to antimalarial treatment given, used counterfeit drugs which could have led to antimalarial treatment failure that might have resulted in spread of antimalarial drug resistance in the population that impacted negatively to malaria control. Studies on effect of socio-economic on malaria were carried out in Western Kenya19 and in all 47 Counties in Kenya4, where study findings of the household malaria survey associated socio-economic inequalities such as wealth (salary included), education level, household size, land size and land use with malaria prevalence19. A Study carried out in rural Uganda20 associated malaria with poverty.
A study was carried out in Western Kenya highlands on female Anopheles mosquitoes and their malaria transmission in regions where bed net ownership was high21, but mosquito bed nets are supposed to cover beds yet poverty-stricken individuals lack beds and it becomes difficult for them to effectively use the nets4. In Busia County, Kenya malaria prevalence was high which was linked to socio-cultural practices and economic factors in procurement and utilization of mosquito nets22. More studies were carried out on mapping socio-economic inequalities on malaria prevalence in sub-Saharan African countries23. Study findings from sub-Saharan Africa on house structure which seem to be linked to economic status and size of the land proved that house structure influenced malaria prevalence10. Houses that are close to each other which might be linked to size of the land encourage malaria transmission from one house to another and house designs with ceiling boards and limited ventilation through windows and doors to some extend reduce entry of mosquitoes into the house2,6,24. A multi-country study on housing improvement and malaria risk10, and on housing and health11 were carried out in sub-Saharan Africa which linked malaria to house design. A study carried out in rice irrigation areas in Western Kenya proved that house designs can reduce the density of female Anopheles mosquitoes that rest inside the houses waiting to transmit malaria at dusk influencing malaria prevalence24.
Lack of knowledge towards malaria infection and adherence to antimalarial drugs prescribed by health workers which may be linked to wealth and education level was reported in New Guinea and in rural Kenya25, 26, 27. Poverty-stricken population are not exposed to current information through media or through other means such as attending malaria days to be educated on malaria control, drug adherence and compliance according to study findings in Kenya4, 5, rural Mozambique and other regions in the world and misconception on malaria infection include being rained on or a curse or a punishment from God as opposed to being bitten by mosquitoes which breed in stagnant water28,29,30. Recorded malaria studies in Vihiga County are mainly on effect of climate on malaria prevalence7. “A malaria - free Kenya, Kenya Malaria Strategy- 2019-2023” recommended effective malaria prevention strategies by people at risk to reduce economic burden of malaria, yet transmission of malaria is determined by socio-economic factors, hence the study.
Materials and methods
Study Site
The study area was Mbale town and its environs which was identified by a global positioning systems (GPS) mapping at Vihiga County headquarters. A baseline survey was done to familiarize with mosquito breeding grounds in the study area before the study commenced. Mbale town is the headquarters of Vihiga County, found within Vihiga and Sabatia sub-Counties, Western Kenya, along Kisumu-Kakamega Road31. It is located at latitude 0° 0′54.0′N and longitude 34°43′17.0 E with an altitude of 1200 meters above sea level, rainfall of between 1800mm to 2000mm annually, highest in April (288 mm) and lowest in January 94 mm31. Highest average temperature occurs in February (21.4° C) and lowest in July (19.1°C) with an annual average temperature of 20.4° C 7, 31. Economic activities in the study area included; crop farming, livestock keeping, fishing, brick making, mining and trading7. This study site was chosen because it had high malaria prevalence and mortality despite various malaria control strategies having been put in place7, 32. The study area had poverty level of 62% with high dependency ratio of 100.9033, which could have contributed towards high malaria prevalence. Population of people in Mbale town and its environs who are mainly Maragoli community was 60,000 according to 2019 population census33 and sample size should have been 382 people but the research used 768 people to cover a higher number of malaria patients because the study area is densely populated34.
Study Design
The study adopted a longitudinal study design35, which was carried out from December 2019 to November 2020 to cater for both short and long rainy seasons.
Data Collection
At the triage room of Mbale Provincial Rural Training Health Center, anthropometric characteristics of the study population were recorded. Patients who were observed with signs of malaria by doctors at the health facility used were screened for malaria by qualified laboratory technicians using microscopy and observation as per world health organization standards28, while other health workers interviewed malaria patients as they administered semi-structured questionnaires stratifying them into various socio-economic status and their residence as per Kenya Malaria Strategy- 2019-2023 5. Records on malaria prevalence data was obtained from the Mbale Provincial Rural Training Health Center. The area for finger-prick to collect blood was first swabbed with methylated spirit to sterilize it and allowed to dry before blood collection was done. Blood films were dried, stained with giemsa stain, immersed in oil and observed under 100 x microscope objectives to examine malaria parasites.
Inclusive and Exclusive Criteria
The study was purposive and equal numbers of 192 malaria confirmed patients/guardians who were volunteering to participate in the study were recruited for each of the following age groups; children below 5 years old, children between 5-14 years old, children between 14-18 years old and adults. Malaria patients with; allergy to antimalarial drugs, chronic infections and people who had been on antimalarial treatment within the preceding 2 weeks were excluded from the study. Most pregnant women were reluctant to participate in the study and they were also excluded.
Sample Size Determination
The sample size formula below was adopted from Krejcie, R.V and Morgan, D.W., 1970 (34).
S = X2NP(1-P)/d2(N-1) +X2P(1-P)
S =Desired sample size
X = Z-value = 1.96 for 95% confidence level, N = Population size (60,000)
P = Population proportion = 0.5,
d = degree of accuracy = 0.05,
S = (1.96)2(60,000) (0.5) (0.5)/(0.05)2(59,999) + (1.96)2(0.5) (0.5)
S = 382.
Data management and analysis
Data was entered in spread sheets and analysed using a SPSS software version 17. Descriptive and inferential data analyses were done. Graphs and frequency tables were used to show distribution of socio-economic factors in the study population while linear regression and correlation were used to analyse effect of various socio-economic factors on malaria prevalence in the study area. P-value ≤ 0.05 was considered statistically significant in all tests.
Ethical considerations
Masinde Muliro University of Science and Technology Institutional Ethical Review Committee granted an ethical review letter (MMU/COR: 509099) while National Commission for Science, Technology and Innovation provided License number: NACOSTI/P/20/3379 for data collection. A written informed consent was signed by adult malaria patients and parents or guardians signed for malaria patients below 18 years old before the study commenced and their confidentiality was guaranteed.
Limitations of the Study
The research was conducted during the COVID-19 pandemic period. Most patients were reluctant to visit health facilities during this period for fear of being infected with COVID-19.
Results
From linear regression analysis obtained, R2 was 0.061 [F (7,760) = 7.063], p < 0.000) showing that overall socio-economic factors had statistically significant effect on malaria prevalence. Individual socio-economic factors that were statistically significant to malaria infection in the study area were; level of education ([F (7,760) = 7.063], p-value = 0.002), wealth [F (7,760) = 7.063], p-value = 0.000, size of land ([F (7,760) = 7.063], p-value = 0.006, house type ([F (7,760) = 7.063], p-value = 0.000 and ventilation in the house ([F (7,760) = 7.063], p p-value = 0.048 as opposed to salary ([F (7,760) = 7.063], p-value = 0.828) and household size [F (7,760) = 7.063], p = 0.916) as shown in table 1.
From analysis obtained, study participants seemed to have deposited empty containers appropriately which included selling them to be recycled (others) irrespective of their level of education as shown in figure 1 which might have influenced malaria prevalence.
Relationship Between the Head of a Household's Level of Education and Disposal of Empty Containers
Analysis obtained showed correlation between information on mosquito's breeding grounds was statistically insignificant to education and wealth while correlation between level of education and malaria prevalence and correlation between wealth and malaria prevalence was statistically significant as shown in table 2.
Wealth in the study referred to quality and quantity of assets one owned which included sources of income such as salary, vehicles, livestock, farms, rental houses, businesses. Televisions, electricity, telephones, and radios are very important in delivering malaria prevention programs. From analysis obtained, it was observed that, large numbers of assets were owned by study participants who had high level of education (tertiary) as shown in figure 2.
Relationship Between the Head of a Household's Wealth and Level of Education in the Study Area
Distribution of salary among study population in the study area was high among individuals earning between Ksh.10, 000 to Ksh. 20,000 per month (51.4 %) who were considered to be earning moderate salary, followed by those who were considered to have had low salary of below Ksh. 10,000 per month (27.9 %), while those earning high salary of over Ksh. 20,000 per month accounted for 20.7 % (Table 3). Most homesteads recorded household size of more than 4 members (57 %) as shown in table 3.
Most participants in the study area lived in areas where the land size was less than 2 acres (92 %). The land which was more than 2 acres in the study area accounted for only 7.9 % (Table 4).
Study population who recorded tertiary level of education constituted 29.2 %, secondary education recorded 28.2 %, primary level of education constituted 27.1 % while 15.5 % of the study population did not have formal education (Table 4). However not all of the study population in the study area who recorded tertiary education were employed.
Permanent houses in the study area constituted 42.6 % while other types of houses constituted 57.4 % (Table 5).
Most individuals in the study area had moderate number of assets which accounted for 47.4 %. Individuals who recorded large number of assets accounted for 25.9 % while individuals with very few assets accounted for 26.7 %. as shown in figure 3.
A Bar Graph Showing Wealth in among Study Population Study in the Study Area
Discussion
Socio-economic factors in the study were considered to be risk factors in malaria prevalence. Socio-economic factors that were considered in the study area included; level of education, salary, wealth, size of the land, household size, types of houses and ventilation in houses. Overall socio-economic factors in the study area were statistically significant (p-value 0.00) to malaria prevalence although the household size (p- value = 0.916) and salary of the head of the household (p- value = 0.828) were statistically insignificant. The following are the individual socio-economic factors that showed statistically significant effect on malaria prevalence; wealth (p- value = 0.000), size of land (p- value = 0.006), house type (p- value = 0.000), other sources of ventilation in the house besides lack of ceiling board (p- value = 0.048) and level of education (p- value = 0.002). From the study area, level of education did not affect disposal of empty containers. From analysis obtained, it was observed that large numbers of assets (57%) were owned by participants who had high level of education (tertiary education which accounted for 29.2%) which might have reduced malaria prevalence in such individuals. Knowledge on stagnant water as breeding ground of mosquitoes plays a vital role in malaria prevention. Analysis obtained showed correlation between information on mosquito's breeding grounds was statistically insignificant to education and wealth while correlation between level of education and malaria prevalence and correlation between wealth and malaria prevalence was statistically significant.
Most heads of the household recorded salary of Ksh. 10,000 to Ksh. 20,000 per month while those earning high salary of above Ksh. 20,000 per month accounted for 20.7 % which might have compromised malaria prevalence in the study area. Most homesteads in the study area occupied less than 2 acres of land (75.9%) which might have encouraged transmission of malaria from one house to another. Most study participants who were more than four (57%) in a homestead and those who also earned low income experienced challenges in purchasing adequate mosquito prevention bed nets which might have exposed them to mosquito bites, increasing malaria prevalence. Houses without ceiling boards and with more ventilation through windows and doors in the study area which accounted for 57.4% to some extend allowed entry of mosquitoes into the house which increased malaria prevalence. The Kenyan government should consider improving socio-economic status of poor population and target malaria control at household level in order to reduce malaria prevalence as recommendations by Degarege9 and attain a malaria free Kenya, Kenya Malaria Strategy- 2019-2023 5.
Socio-economic factors were considered to be risk factors in malaria transmission which influenced malaria prevalence3, 9, 36. Socio-economic factors in the study area were statistically significant (p-value 0.00) to malaria prevalence supporting study findings in Western Kenya Highlands19, Busia22 and Siaya19 Counties in Kenya, Tanzania17, sub-Sahara African countries12, 23, India8, Pakistan36, Nigeria13, 14, and Ethiopia16. High level of education in the study area seemed to have enabled individuals to understand the causes, management and prevention of malaria as opposed to individuals with low or no formal education, supporting study findings in rural Uganda15,20 and in endemic primary health centres in Assam, India12. From the results obtained in the study area, a good number of study participants who either dropped at primary school level and those without any formal education in study area tended to link malaria to feeding on first harvest of maize and beans, curse from God and being rained on supporting study findings from Kenya Malaria Indicator Survey, 2020 4 on malaria beliefs. In some cases, study population seemed to have preferred white bed nets to the green or blue nets which they claimed suffocated them and led to miscarriage in pregnant mothers. This misconception led them to use mosquito nets to cover their fish and vegetables thus increasing malaria prevalence in the study area. Most study participants with no formal education also found it difficult to link malaria to stagnant water and mosquito bites.
Wealth in the study was considered to be the income from the salary if employed and quantity and quality of assets owned by the head of the household which was statistically significant to malaria prevalence. One can be wealthy without necessarily being well educated. Wealth affected malaria prevalence in study area supporting study findings that were carried out in rural Uganda20, which linked malaria to poverty. Most individuals who earned over 20,000ksh per month (25.9%) in the study area (availability of money and property in this case) were able to purchase enough insecticide-treated mosquito nets for all household members in consistence with findings from Western Kenya highlands21, built houses with ceiling board to prevent entry of mosquitoes into the houses supporting findings in other regions in Western Kenya24 and sub-Saharan Africa10, sprayed houses regularly with insecticides, bought original antimalarial drugs as counterfeits drugs can cause unavoidable malaria deaths and availability of money also enabled individuals to take their household members for malaria treatment early enough4, 5. However, level of education and wealth of the study population were statistically insignificant to information on breeding grounds of mosquitoes which transmitted malaria. Poverty level in study area was very high (62%) with high dependency level31, 33, which was a challenge to participants with low salary and very few assets to effectively engage in quality malaria management, similar to findings in Busia County, Kenya22, rural Uganda20, Chewaka district, Western Ethiopia16, and in sub-Saharan Africa countries, which linked malaria to poverty. One can be well educated with a lot of information on how to treat and prevent malaria but may lack money may be due to being unemployment which may prevent a person from controlling or treating malaria effectively. From correlation analysis obtained in the study area, wealth was statistically insignificant to level of education and information on mosquito breeding grounds.
The size of the land to some extend determined malaria transmission which influenced malaria prevalence where individuals with comparatively large pieces of land over 2 acres in the study area were able to farm far from the location of their houses as opposed to close houses which were observed in areas where the sizes of land were less than 2 acres. Mosquitoes easily transferred malaria parasites from one house to another in compounds where the sizes of land were small which increased malaria prevalence in the study area. In cases where farmers decided to construct fish ponds for their income generation on small pieces of land, the stagnant water in the fish ponds attracted breeding of mosquitoes increasing malaria prevalence. Research participants who were more than 4 in a home with low income in the study area were unable to buy adequate mosquito prevention bed nets to increase the number the Kenyan government provided which exposed them to more mosquito bites increasing malaria prevalence. Participants from low income homesteads in the study area used insecticide-treated bed nets in turns while some decided to tear them to enable everybody in the home to tie the net on their heads at night to prevent mosquito bites which increased malaria prevalence in the study area.
House designs in some parts of the study area lacked ceiling boards (57.2 %) which influenced entry of mosquitoes into the houses supporting study findings that were carried out in rice irrigation areas in Western Kenya24 and in sub–Sahara Africa10, 11. Number of windows and doors in a house which were used as house ventilation created entry of mosquitoes into the house and hence increasing malaria prevalence. During the study, it was observed that participants in some homesteads lacked vital information on mosquito breeding grounds. They did not associate fish ponds, disposal of empty containers, creating burrow pits by gold mining and brick making with malaria. In some cases, participants failed to adhere to, and comply with antimalarial drugs and their knowledge on causes and prevention of malaria was poor supporting a study that was carried out in Papua New Guinea and other parts of the world25, 27,30. In Nigeria, socio-economic factors influenced malaria incidences in Calabar region where treatment and control of malaria attracted more financial and human resources in the budget of Nigeria government13. The Kenya government should emulate malaria case management from Nigeria by campaigning for more malaria treatment and control funding from other donor countries to increase the 26% yearly budgetary allocation on health which malaria treatment and control takes most of it4. The African Union agenda 2063 include; quality of life and well-being, health and economic growth37 and health as one of Kenya's big four vision 2030 38 aim at reducing poverty and improving health which should in turn decrease malaria burden in Kenya and other African countries.
Conclusion and recommendations
Socio-economic factors influenced malaria prevalence in the study area as they determined malaria transmission. Malaria prevalence was high among individuals from poverty-stricken homesteads. Malaria control strategies should be strengthened in study area and in Kenya at household level to reduce malaria prevalence. The Kenya Malaria Strategy- 2019-2023 objective to achieve a malaria-free Kenya can be realized by strengthening implementation of malaria control strategies which is linked to socio-economic factors. There should be appropriate economic and social interventions in low- income and poverty- stricken individuals in the study area, Kenya and the whole world to reduce and eliminate malaria burden. Campaign on use of malaria vaccines should be monitored regularly as a way of eliminating spread of malaria transmission especially in rural areas where most low income people who may not have access to internet, newspapers and television live. The Kenyan government should regularly educate people on net treatment and proper use because individuals especially in poverty-stricken areas used torn nets which allowed mosquito bites while others did not use given nets at all which increased malaria prevalence in some regions in the study area. The government should provide free malaria treatment in public health facilities where most poor individuals get their treatment and allow more health personnel to reach remote areas to educate people on malaria treatment and control. The Kenya government and the world at large should also put more emphasis on use of modern technology and laboratories to eliminate circulating counterfeit drugs from the market in order to prevent increase in malaria deaths.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AMREF Africa Medical and Research Foundations. Community Health Workers enhance health service delivery in Western Kenya 2020 http://amref.org.kenya.community.health
- 2World health organization World malaria report 2020. 20 years of global progress and challenges 2020 November 30global report ISBN: 978.92 4-001579-1(electronic version) ISBN 978-92 4-001580-7 (print version) www.who.int/publication/Reports
- 3Omukunda E Githeko A Ndong'a MF Emmanuel Mushinzimana E Atieli H Wamae Peter Malaria vector population dynamics in highland and lowland regions of western Kenya J Vector Borne Dis 2013 Apr-Jun 5028592(2013). PMID: 2399530923995309 · pubmed ↗
- 4Republic of Kenya MALARIA Indicator Survey Division of Malaria Control Ministry of Public Health and Sanitation Kenya National Bureau of Statistics ICF Macro 2020 https://dhsprogram.com/pubs/MIS 7/MIS 7.pdf
- 5Kenya Malaria Strategy-2019-2023 https://fountainafrica.org/wp-content/uploads/2020/01/Kenya-Malaria-Strategy-2019-2023.pdf
- 6Center for Disease Control and Prevention About Malaria Kenya.cdc.gov/malaria 2019 https://www.cdc.gov/malaria/index.html
- 7Wafula H Mulinya C Impact of climate change on spread of malaria in Vihiga county, Kenya 2018 www.iosrjournals.org. doi:10.9790/2402-1201011626
- 8Sharma Ravendra K Rajvanshi Harsh Lal Altaf A Socio-economic determinants of malaria in tribal dominated Mandla district enrolled in Malaria Elimination Demonstration Project in Madhya Pradesh Malaria Journal Research 2021 https://malariajournal.biomed-central.com 10.1186/s 12936-020-03540-x PMC 778697133402186 · doi ↗ · pubmed ↗