A comparative assessment of CD4 recovery in a cohort of patients on different HAART regimens in a Nigerian tertiary healthcare facility
Paul Onah, Catherine Idoko, Aliyu Kai'gama, Siyaka Abdulateef

TL;DR
This study compares CD4 cell recovery in patients on different HIV treatments in Nigeria, finding that while some improvement occurs, many patients still struggle to reach immune recovery goals.
Contribution
The study provides a comparative analysis of CD4 recovery across four HAART regimens in a Nigerian setting, highlighting persistent challenges in immune reconstitution.
Findings
CD4 cell counts increased by 65.6–82.1% of baseline values, with Efavirenz-based regimens showing the highest rise.
Patients who reached CD4 counts ≥500 cells/ml showed an additional 22.2–34.1% increase compared to baseline.
A high proportion (65.9–77.8%) of patients on all regimens experienced incomplete immune recovery.
Abstract
Antiretroviral therapy is expected to produce sustained viral load reduction and a rise in CD4 cell count, both of which are important clinical markers of immune recovery. There is contrasting clinical evidence of CD4 stability among patients on long term therapy, which is a major challenge in poor resource settings. This study aims to evaluate CD4 cell recovery among patients on four regimens who have been on long term antiretroviral therapy This was a retrospective cohort study using data from the medical records of patients on four antiretroviral regimens. A three year record of CD4 cell count of 405 randomly selected subjects was extracted for analysis. The increase of CD4 cells was between 65.6 – 82.1% of baseline values, with the highest rise occurring with Efavirenz based regimens. Among patients who achieved target CD4 cell counts ≥ 500 cells/ml, there was further increase of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
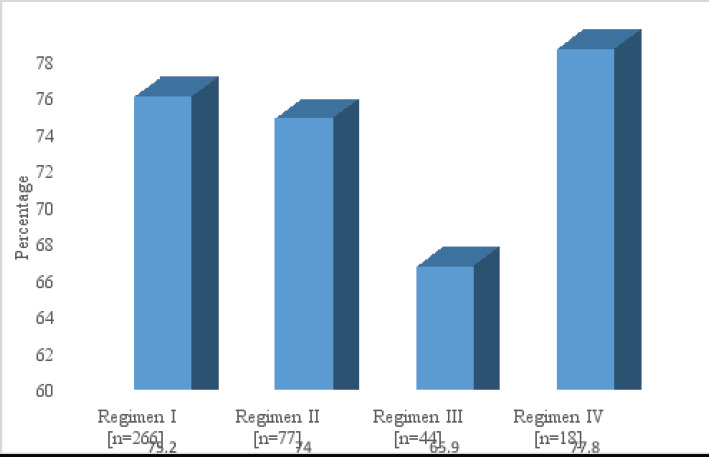 Figure 1
Figure 1| Variable | Number % |
|---|---|
|
| |
| Male | 177 35.4 |
| Female | 324 64.6 |
|
| |
| Illiterate | 305 61 |
| Primary | 75 15 |
| Secondary | 88 17.6 |
| Tertiary | 32 6.4 |
|
| |
| Single | 52 10.4 |
| Married | 347 69.4 |
| Divorced | 78 15.6 |
| Widowed | 23 4.6 |
|
| |
| Self employed | 184 36.8 |
| Civil service | 85 17 |
| Unemployed | 210 42 |
| Student | 21 4.2 |
| Mean age yrs. |
|
| Duration on HAART yrs. | |
| 1 – 3 | 100 24.6 |
| 4 – 6 | 221 54.6 |
| 7 – 9 | 51 12.6 |
| ≥ 10 | 33 8.2 |
| Mean SD |
|
| Year 2016 | Year 2017 | Year 2018 | P value | CD4 | |
|---|---|---|---|---|---|
| Regimen I | 365.5 161.2 | 466.1 158.2 | 665.5 162.8 | <0.0001 | 82.1 |
| Regimen II | 380.5 183.3 | 479.2 153.4 | 634.5 182.3 | <0.0001 | 66.8 |
| Regimen III | 408.9 171.3 | 468.7 130.1 | 698.9 211.7 | <0.0001 | 70.9 |
| Regimen IV | 379.8 157.4 | 428.5 116.5 | 629.1 220.8 | <0.0001 | 65.6 |
| Year 2016 | Year 2017 | Year 2018 | P value | CD4 increase % | |
|---|---|---|---|---|---|
| Regimen I | 594.3 87.2 | 675.4 102.7 | 618.9 94.8 | <0.0001 | 24.8 |
| Regimen II | 568.2 48.6 | 611.7 66.9 | 657.1 72.9 | 0.0002 | 25.9 |
| Regimen III | 533.7 20.8 | 597.8 37.8 | 689.5 50.7 | <0.0001 | 34.1 |
| Regimen IV | 574.4 61.8 | 609.6 41.5 | 653.7 80.4 | 0.2585 | 22.2 |
| CD4 count | Regimen I | Regimen II | Regimen III | Regimen IV | P value |
|---|---|---|---|---|---|
| ≤ 100 | 80.7 ± 5.2 | 72.7 ± 12.1 | na | 92.1 ± 2.7 | < 0.001 |
| 101 – 200 | 179.2 ± 20.3 | 189.1 ± 7.5 | 154.4 ± 9.9 | 166.2 ± 10.4 | < 0.001 |
| 201 - 300 | 287.9 ± 9.1 | 256.3 ± 22.7 | 275.5 ± 15.7 | 255.5 ± 13.9 | < 0.001 |
| 301 – 400 | 365.5 ± 31.1 | 380.5 ± 13.3 | 348.9 ± 22.2 | 379.8 ± 11.1 | < 0.001 |
| 401 – 500 | 466.1 ± 18.2 | 477.2 ± 20.2 | 450.2 ± 10.1 | 447.2 ± 16.7 | < 0.001 |
| 501 - 600 | 532.5 ± 10.8 | 535.5 ± 19.4 | 575.6 ± 17.2 | 581.7 ± 12.5 | < 0.001 |
| ≥ 601 | 798.5 ± 55.6 | 733.5 ± 8.7 | 822.2 ± 60.7 | 676.5 ± 27.8 | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV Research and Treatment · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
One of the major clinical markers of immune recovery among patients on highly active antiretroviral therapies HAART is the improvement in CD4 T lymphocyte count. It is considered to be an important predictor of disease progression, occurrence of opportunistic infections and long term reconstitution of immune function in patients living with HIV infection 1,2 It is expected that patients on HAART will achieve normal CD4 count and undetectable viral load both of which are indicated for monitoring disease progression. Immune reconstitution following antiretroviral therapy occur in three distinct phases all of which can be explained by the rate of CD4 recovery.
In the first phase, which usually last for 2 – 3 months of therapy, the number of peripheral CD4 cells increase rapidly at the rate of 20 – 30 cells/mm^3^/month3,4,5. The second phase of recovery generally slow down to between 5 – 10 cells/mm^3^/month, while the third phase is characterized by even slower increases of between 2 – 5 cells/mm^3^/month. The last two phases involves de novo production of CD4 cells by the thymus gland, homeostatic proliferation and extension of the half-life of circulating CD4 cells.
Many patients who achieved effective viriologic suppression, often fail to optimize and sustain CD4 recovery over long periods of therapy. A significant percentage of patients on therapy not only fail of achieve optimal immune recovery, but those who do may take years to have normal CD4 cell count6,7. A number of studies reported that up to a third of patients on therapy do not achieve normal CD4 cell count within five years of therapy8,9,10. The recovery of CD4 positively correlates with lower risk of opportunistic infections, disease progression and mortality11,12.
The long term effect of HAART on CD4 cell recovery is a subject of debate because questions still remain as to whether or not the initial CD4 cell rise is maintained over long period of time 13. While some studies reported that CD4 cell rise following initiation of therapy vary widely between antiretroviral regimens, this has not been consistently observed between patients3, 14. A number of comparative studies have reported that CD4 cell recovery differ widely among patients on different regimens15,16,17,18,19. For instance, some studies reported better CD4 recovery rates with Efavirenz containing regimens15,20,21, while others reported contrasting recovery rates13.
Several longitudinal studies carried out in north American and European adults living with HIV showed that CD4 recovery continued to improve after 4 – 7 years of therapy22,23,24,25 and stabilized26,27 or at least remained stable in a subset of patients28. The trajectory of CD4 recovery is largely unknown largely due to differences in patient specific characteristics, CD4 at initiation of therapy29, presence of co-infections, treatment interruptions and adherence, all of which may explain the highly variable study conclusions.
A review of randomized clinical trials involving Nevirapine and Efavirenz based regimens have demonstrated good CD4 recovery rates, though the latter has been reported as a better choice as initial therapy13. In contrast, a number of other studies reported short term increase in CD4 recovery with all regimens30, however there was no significant difference in the rate of immune reconstitution on the long term.
Some patients who failed to achieve normal CD4 counts after long term therapy ≥ 7 years have been reported to have had low CD4 at the point of initiating therapy 30,31, though this observation may not be representative of all subset of patients.
A number of determinants of immune recovery included increasing age 32,33,34,35, viral suppression36,37, CD4 count at initiation of therapy 38, the presence and severity of co-morbidities.
The achievement and stability of normal CD4 count over long period of time is critical to optimal immune recovery, improved quality of life, lower risk of opportunistic infections and risk of mortality. The aim of this study is to assess CD4 cell recovery among patient receiving different HAART regimens
Methods
Setting: The study was carried out at the ARV clinic of University of Maiduguri teaching hospital. This is a public tertiary hospital which also serve as a referral centre for both private and public health facilities in the Nigeria's north east region. The HIV clinic provide services which include diagnosis, treatment and prevention as well as management of complications and comorbidities. The clinic units included adult ART unit, paediatric ART unit, prevention of mother to child transmission PMTCT unit and laboratory.
Study design
This was a cross sectional retrospective study using data obtained from the medical records of patients who have been on HAART regimens for at least two years and above at the start of the study. The three year CD4 records obtained were from 2016, 2017 and 2018.
Sample size: A total 405 eligible subjects were selected and records used for the study. The medical records were separated according to their HAART regimen before selection by simple random method.
Eligibility: The subjects must have been above 18 years and have been on HAART for at least two years at the time of the study. They must have at least attended 90% of physician appointment and have routine CD4 test done at least once a year during the study period.
Data collection: Data was extracted from medical and laboratory records as related to CD4 counts during the three year study period 2016 – 2017. The primary outcome measure for complete CD4 recovery was ≥ 500 cells/ml.
HAART regimens
Regimen I
Tenofovir/Lamivudine/Efavirenz (n = 266)
Regimen II Zidovudine/Lamivudine/Nevirapine (n=77)
Regimen III Tenofovir/Lamivudine/Dolutegravir (n=44)
Regimen IV Zidovudine/Lamivudine/Lopinavir/Ritonavir (n=18)
Data analysis
The data was double checked for accuracy and entered into SPSS 21 for descriptive and inferential statistics. The analysis was carried out using one way ANOVA Tukey post Hoc and P values ≤ 0.05 was considered statistically significant. The proportion of subjects with incomplete CD4 recovery was expressed using descriptive statistics. Ethical approval: The health research ethics committee of the University of Maiduguri teaching hospital approved the study.
Results
The results showed that the population of females almost doubled that of males. The mean age of patients was 35.410.2 years and majority of subjects had primary level education (69.1%) and were married (69.4%) Table 1.
There was statistically significant increase in CD4 cell count with the four HAART regimens. The rise was about 82.1% among patients on regimen I, 66.8% regimen II, 70.9% regimen III and 65.6% in patients on regimen IV during the three year study period Table 2.
Among patients who achieved immune recovery at the beginning of the study ≥ 500 cells/ml, there was also a significant increase in CD4 cell count except for patients on regimen IV. The overall increase in this subset was between 22.2 – 34.1% of baseline values. Table 3.
A comparison of CD4 cell count showed significant differences between the four regimens < 0.001. This result showed that in spite of therapy many patients continued to have poor immune recovery irrespective of HAART regimen. Patients with CD4 cell counts of ≤ 200 cells/ml are particularly at a higher risk of opportunistic infections and disease progression Table 4
The results showed a high percentage of patients with incomplete immune recovery <500 cells/ml with the four regimens. The distribution showed that between 65.9 – 77.8% of all patients did not achieve target CD4 cell count during the study period Figure 1.
Distribution of patients with incomplete immune recovery ≤ 500 cells/ml
Discussion
Antiretroviral therapy is known to not only improve CD4 count and immune recovery, it also reduces viral load and improve patient's quality of life. The rise of CD4 T-cell lymphocyte count following initiation of therapy has been used as a clinical marker of immune recovery among patients living with HIV. Majority of subjects in this study were females which was comparable to some previous studies39,40,41, which is reflective of the fact that women in sub Saharan Africa are at higher risk of infection compared to males.
The CD4 cell count significantly fluctuated among patients on the same regimen. Among patient who achieved target CD4 recovery the variation was also significant. While the percentage of patients who failed to achieve complete immune reconstitution was high like in some previous studies42,43,44, the increase in CD4 occurred though at significantly different rates45,46.
The results clearly showed that CD4 recovery was still ongoing, a significant percentage of patients did not achieve targets 47. There is clinical evidence to believe that immune restoration with CD4 cells levels of ≥ 500 cells/mm^3^ is associated with comparable mortality rates with uninfected individuals, so this cutoff value has been widely used to benchmark immune reconstitution in many studies48,49 similar to this study.
The increase of CD4 cell observed across the four regimens was comparable to earlier previous studies50,51. The percentage of patients with incomplete CD4 recovery is considerably higher than 20 – 49.7% reported7,52,53. Patients are expected to achieve and sustain immune recovery early in the course of therapy, studies have established that many patients still fail to achieve normal CD4 cells, though the rate in this study is comparatively higher 9. A number of other studies however reported contrasting levels of immune recovery8,54, which suggests that achieving optimal CD4 recovery is far from being a certain clinical outcome55, 56, 57
The rise in CD4 is known to be nonlinear and unrelated to HAART regimen which indicated no demonstrable superiority exist between regimens55,58. There is some literature evidence that Tenofovir based regimens were better than Zidovudine based regimens59,60, though contrasting conclusions have been reported in one study61.
Similar studies reported no differences in CD4 recovery between Nevirapine and Efavirenz based regimens 21, however other studies appear to contradict this conclusion 36. The highly variable effect of long term HAART on CD4 cell recovery shown by several studies62,63, 64; indicated a number of determining factors some of which include, duration of therapy 13, 28, low CD4 cell at initiation of therapy 24, viral suppression, advancing age, non-adherence, haemoglobin level, adverse drug reactions39,45,46.
The low CD4 recovery may also be associated with poor viral suppression and extensive immunological damage as reported in some studies65. This non-optimization of immune recovery among patients on long term therapy significantly increase the frequency and severity of opportunistic infections66 and ultimately poor clinical outcomes.
Conclusion
This study clearly showed that immune reconstitution continue to occur among patients on all regimens, however a significant percentage of them did not achieve target CD4 cell count. There is need to strengthen routine monitoring as incomplete immune recovery still remain a long term challenge to the achievement of positive clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hogg RS Rates of disease progression by baseline CD 4 cell count and viral load after initiating triple drug therapy Journal of American Medical Association 2001286202568257710.1001/jama.286.20.256811722271 · doi ↗ · pubmed ↗
- 2Grabar S Clinical outcome of patients with HIV infection according to immunologic and viriologic response after 6 months of highly active antiretroviral therapy Annals of Internal Medicine 200013364014101097595710.7326/0003-4819-133-6-200009190-00007 · doi ↗ · pubmed ↗
- 3Corbeau P Reynes J Immune reconstitution under antiretroviral therapy: The new challenge in HIV-1 infection Blood 201111721558255902140312910.1182/blood-2010-12-322453 · doi ↗ · pubmed ↗
- 4Guihot A Immune and viriological benefits of 10 years of permanent viral control with antiretroviral therapy Aquired Immune Dediciency Syndrome 201024461461710.1097/QAD.0b 013e 32833556 f 319952710 · doi ↗ · pubmed ↗
- 5Guihot A Immune reconstitution after a decade of combined antiretroviral therapies for human immunodeficiency virus Trends in Immunology 20113231311372131704010.1016/j.it.2010.12.002 · doi ↗ · pubmed ↗
- 6Lawn SDCD 4 cell count recovery among HIV infected patients with very advanced immunodeficiency commencing antiretroviral treatment in Sub Saharan Africa BMC Infectious Disease 200665910.1186/1471-2334-6-59PMC 143590816551345 · doi ↗ · pubmed ↗
- 7Engsig FN Long term mortality in HIV positive individuals virally suppressed for > 3 years with incomplete CD 4 recovery Clinical Infectious Disease 20145891312132110.1093/cid/ciu 038PMC 627689524457342 · doi ↗ · pubmed ↗
- 8Asfaw ACD 4 cell count recovery trends after commencement of antiretroviral therapy among HIV infected patients in Tigray – Northern Ethiopia: A retrospective cross sectional study Plos One 2015103 e 01225832581622210.1371/journal.pone.0122583 PMC 4376855 · doi ↗ · pubmed ↗