Estimating the under-five malaria risk in Uganda based on the nearest neighbour matched analysis technique
Charles Natuhamya

TL;DR
This study estimates how insecticide-treated nets and indoor spraying affect malaria risk in children under five in Uganda.
Contribution
The novel use of nearest neighbour matched analysis to assess malaria interventions in under-five children in Uganda.
Findings
ITNs/LLINs significantly reduce under-five malaria risk.
IRS also significantly reduces under-five malaria risk.
ITNs/LLINs have a positive effect on IRS effectiveness.
Abstract
Malaria still remains a global burden especially in the under-five despite efforts made towards reducing it. The most recommended vector control methods are; use of insecticide treated nets (ITNs) or long lasting insecticide nets (LLINs) and use of indoor residual spraying (IRS). However, these innovations may not have the same effect on malaria risk in the under-five. This study therefore aimed at assessing; the effect of ITNs/LLINs on malaria risk, the effect of IRS on malaria risk, and the effect of ITNs/LLINs on IRS, using nearest neighbours matched analysis. Nearest neighbour matched analysis was used to match the treated and control units by taking each treated unit and searching for the control unit with the nearest neighbours without replacement. The results revealed a significant and negative effect of ITNs/LLINs and IRS on malaria risk [ATET=-0.05; 95% CI= -0.07 – -0.02] and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
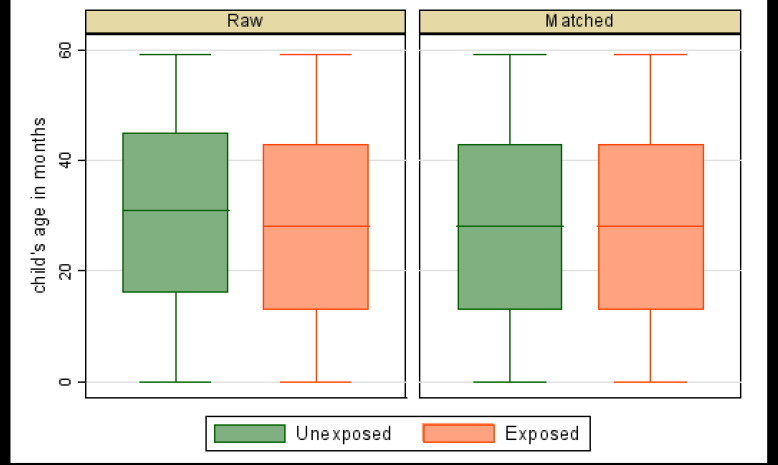 Figure 1
Figure 1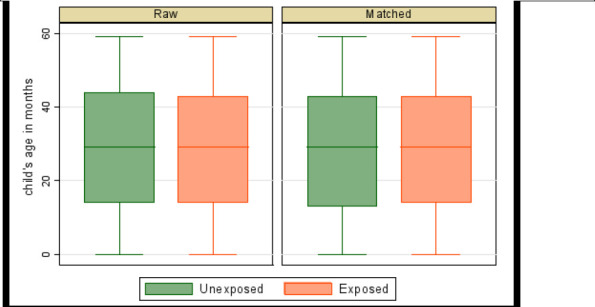 Figure 2
Figure 2 Figure 3
Figure 3| Background Characteristics | Category | Count | Percent |
|---|---|---|---|
| Child's sex (n=7,632) | Male | 3,870 | 50.7 |
| Female | 3,762 | 49.3 | |
| Child's age (n=7,632) | <1 | 1,502 | 19.7 |
| 1 | 1,441 | 18.9 | |
| 2 | 1,502 | 19.7 | |
| 3 | 1,608 | 21.1 | |
| 4 | 1,579 | 20.7 | |
| Anaemia (n=7,632) | Not anaemic | 3,692 | 48.4 |
| Anaemic | 3,940 | 51.6 | |
| Household wealth index (n=7,632) | Low | 4,385 | 57.5 |
| Middle | 1,229 | 16.1 | |
| High | 2,018 | 26.4 | |
| Used IRS (7,592) | No | 6,603 | 87.0 |
| Yes | 989 | 13.0 | |
| Mother's education (n=6,358) | No education | 1,356 | 21.3 |
| Primary | 3,647 | 57.4 | |
| Secondary or | 1,355 | 21.3 | |
| higher | |||
| Used an ITN/LLIN (n=7,632) | No | 964 | 12.6 |
| Yes | 6,668 | 87.4 | |
| Residence (n=6,971) | Rural | 5,518 | 79.2 |
| Urban | 1,453 | 20.8 | |
| Region (n=7,632) | Central | 1,189 | 15.6 |
| East | 1,729 | 22.7 | |
| North | 1,701 | 22.3 | |
| West | 3,013 | 39.5 |
| Estimate | Standard error (SE) | (95% CI) | |
|---|---|---|---|
| Effect of ITN/LLIN and IRS on malaria risk | |||
| Has ITN/LLIN | -0.05 | 0.01 | [-0.07, -0.02] |
| Used IRS | -0.12 | 0.02 | [-0.15, -0.09] |
| Effect of ITN/LLIN on IRS | |||
| Has ITN/LLIN | 0.03 | 0.01 | [0.01, 0.05] |
| Number of observations | Effect of ITN/LLIN on malaria risk | Effect of IRS on malaria risk | Effect of ITN/LLIN on IRS | |||
|---|---|---|---|---|---|---|
|
| ||||||
| Raw | Matched | Raw | Matched | Raw | Matched | |
| Total | 6,931 | 8,406 | 6,931 | 1,974 | 6,931 | 8,406 |
| Treated | 4,203 | 4,203 | 987 | 987 | 4,203 | 4,203 |
| Control | 2,728 | 4,203 | 5,944 | 987 | 2,728 | 4,203 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Statistical Methods and Bayesian Inference · Advanced Causal Inference Techniques
Introduction
Malaria is an infection caused by a parasite of the genus Plasmodium1 that is transmitted by female anopheles mosquitoes2. Despite efforts toward reducing malaria, it remains a global burden 3. In 2018, about 228 million cases of malaria occurred worldwide, of which more than 50% were accounted for by six countries, including Uganda4. Sub-Saharan Africa accounted for the majority (95%) of these cases5. Globally, children aged under five years are the most vulnerable age group affected by malaria. In 2018, they accounted for 67% (272 000) of all malaria deaths worldwide4. In Uganda, approximately 1 in 10 children (9%) aged 0-59 months tested positive for malaria via microscopy in 2018–19 6. The most significant risk factors were considered in this study that is; indoor residual spraying, mosquito bed nets, wealth index, place of residence, and mother's education level, among others7–10. A lot of investment has been made in ITNs, LLINs, and IRS as malaria innovations11. The use of these innovations has been reported to reduce under-five malaria risk12–16. As an example, in 2019, insecticide-treated nets (ITNs/LLINs) protected an estimated 46% of all people at risk of malaria in Africa2. Specifically, in Gulu District of Uganda, IRS effectively reduced the annual prevalence of malaria from 71.5% in 2009 to 29% in 20149. The WHO recommendation of vector control (ITNs/LLINs and IRs) as malaria prevention methods2,17 further informed their choice as treatment groups during analysis in this study. Estimation of average treatment effects is an important goal in evaluation research and programs18. Randomized control trials (RCTs) are viewed as the ideal evaluation technique for estimating treatment effects. Often, however, randomization is not feasible or permissible19. Matching methods can substitute RCTs in observational data20 as they reduce bias in these data21. Nearest neighbour estimators match each treated unit to a fixed number of untreated units with similar values for the pretreatment variables18. In this study, we assessed the effect of ITNs/LLINs on malaria risk, the effect of IRS on malaria risk, and the effect of ITNs/LLINs on IRS, using data drawn from the Uganda Malaria Indicator Survey of 2018-19.
Methods
Data Source and Study Population
This study used secondary data from the most recent Uganda Malaria Indicator Survey (UMIS) of 2018-19. These data were based on a two-stage cluster and stratified sampling technique qualifying them as observational data based on a complex survey design. The first sampling stage involved selecting clusters from sampling frames. Overall, 320 clusters were selected of which 84 were in urban areas and 236 in rural areas. The second sampling stage involved a systematic selection of households and a total sample size of 8,878 households was considered. The study population consists of children less than 5 years of age who were tested for anaemia and malaria infection. Blood samples for biomarker testing were collected by finger-or heel-prick from children aged 0-59 months. Each field team included two health technicians who carried out the anaemia and malaria testing and prepared the blood smears. Three questionnaires were used during the survey (household questionnaire, woman's questionnaire, and biomarker questionnaire). Basic information was collected using the household questionnaire on the characteristics of each person in the household, for example, their age and sex. The data on the age and sex of household members obtained from the household questionnaire were useful in identifying women to be interviewed for under-five children eligible for anaemia and malaria testing. The household questionnaire also captured information on the household's dwelling unit characteristics such as ownership of mosquito nets and indoor residual spraying. The results of the anaemia and malaria testing of under-five children were recorded in the biomarker questionnaire6. Notably, the outcome variable is malaria test result (positive and negative) which signifies malaria risk.
Nearest Neighbour Matching (NNM)
Nearest neighbour and propensity score matching methods are the most commonly used techniques to estimate treatment response using observational data20,22. Despite the popularity of propensity score matching in observational studies, it has a major drawback of pairing individuals of the case and control in the compressed one-dimensional space of propensity scores23 and hence, nearest neighbour matched analysis was used instead, in this study. During analysis, the four steps recommended24 were followed while matching, with the first three representing the design and the fourth the analysis. These are: 1) defining closeness – the distance measure used to determine whether an individual is a good match for another; 2) implementing a matching method, given that measure of closeness; 3) assessing the quality of the resulting matched samples and 4) analysis of the outcome and estimation of the treatment effect, given the matching done in Step (3). The k:1 nearest neighbour matching form was used instead of the 1:1 form, which is the simplest NNM as the latter form can discard a large number of observations and thus would most likely lead to reduced power24. The Mahalanobis distance metric was applied to improve performance while matching. The nearest neighbour matching analysis estimates the average treatment effect (ATE) and average treatment effect on the treated (ATET) from observational data. The average treatment effect on the treated was estimated and used since the study intended to evaluate the treatment effects on children for whom policy or programs are intended for instead of average treatment effects on the whole population, which is useful to evaluate the expected effect on the outcome if children in the population were randomly assigned to treatment. During analysis, children in the treated and control groups were matched by taking each treated child and searching for the control child with the nearest neighbour without replacement. The ATET of interest was then obtained by averaging the difference between the outcome of the treated children and the outcome of the matched control children25–27 using the formula for the nearest neighbour matching estimator below;
Where N^T^ is the number of children in the treated group (those who used ITN/LLIN or whose households used IRS), is the number of children in the control group matched with the treated child i, is equal to if j is a control units of i, and zero otherwise and w_j_ = Σi w_ij_. Box plots of matching over treatment levels were used to check balance of matched data. Matching was considered balanced (of similar distribution) if the matched-sample box plots were the same over the treatment levels.
Results
Characteristics of under-five children
A sample of 7,632 children under the age of 5 years formed the sample of this study. The children were evenly distributed by sex and anaemia status. Most of the children were from households with low wealth index (57.5%), resided in rural areas (79.2%), and were located in the western region (39.5%). The majority of the children had used an ITN or LLIN (87.4%) and resided in households that had not used IRS in the past 12 months of the survey (87.0%). The rest of the results are presented in Table 1.
Effect of ITNs/LLINs and IRS on malaria risk
After nearest neighbour matching, the probability of malaria was 5% [ATET=-0.05; 95% CI= -0.07 – -0.02] lower in children who used ITNs/LLINs compared to the same children who did not. This indicates that sleeping under a mosquito bed net reduces the chances of malaria infection in under-five by 5% compared to not sleeping under the bed nets. The probability of malaria infection among children whose households had sprayed their dwellings in the past 12 months of the survey was 12% [ATET=-0.12; 95% CI= -0.15 – -0.09] lower compared to similar children whose households had not sprayed their dwellings in the same period. Similarly, this implies that use of IRS reduces the chances of malaria infection compared to not using it. It also indicates that IRS has a higher effect compared to use of ITNs/LLINs in reducing the probability of malaria infection in the under-five. The results further revealed that the probability of IRS is 3% [ATET=0.03; 95% CI= 0.01 – 0.05] higher among children who slept under an ITN/LLIN compared to similar children who did not sleep under these bed nets. This indicates that using ITNs/LLINs increases the likelihood of using IRS by 3% compared to not using it as a vector control measure. Results are presented in Table 2.
The box plots (balance plots) for the matched sample are very similar across (Figures 1, 2, 3). The medians, the 25th percentiles, and the 75th percentiles appear to be the same, as well as the tails. Matching appears to have balanced matching variables (child's age in months, child's anaemia status, age of household head, sex of household head, and residence) with the child's age as the bias-adjustment covariate. Mahalanobis distance based on the child's age was used to find matches. The balance of matched data is further indicated in Table 3.
Balance plot of risk of malaria by LLIN/ITN
Balance plot of risk of malaria by IRS
Balance plot of IRS by ITN/LLIN
Discussion
Findings from this study are similar to other studies28–30 as IRS was also associated with a lower risk of malaria. Similarly, ITNs/LLINs (insecticide-treated bed nets) were an important intervention for reducing malaria risk30–33. However, the effect of ITNs/LLINs was lower than that of IRS34. Reasons for this lower effect include; being disliked and hence misused35, there are species-specific differences in biting hours36, there is fear of chemicals, and inherent cultural beliefs37, among others. Results from this study further show that there was an association between ITN/LLIN and IRS; a household where IRS was done in the past 12 months was more likely to sleep under an ITN/LLIN. This is similar to a study38 which showed that a child under five years of age who lived in a house that had been recently sprayed was 3.1 percentage points more likely to sleep under a treated bed net.
One of the limitations of this study was the data collection procedure of one of the vector control methods. Information on whether a household used IRS was obtained by asking a household member whether the household had been sprayed against mosquitoes in the last 12 months. This was subject to recall bias as it is possible that the household member who answered the question did not remember this event or was not present at the time of spraying, which could have resulted in misreporting of IRS.
Conclusions and Recommendations
The findings from this study illustrate a significant and negative relationship between malaria risk and ITN/LLIN use, malaria risk, and IRS during the past 12 months of the survey, but a significant positive relationship between IRS and ITN/LLIN use among the under-five in Uganda. The implementation of policies and programs towards effective use of ITN/LLIN and IRS can reduce the burden of under-five malaria in Uganda. The nearest neighbour matched analysis technique was effective in determining treatment effects. Analysts can use the matching method to determine treatment effects of malaria interventions while dealing with observational malaria data.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sato S Plasmodium—a brief introduction to the parasites causing human malaria and their basic biology J Physiol Anthropol 2021 Jan 740113341368310.1186/s 40101-020-00251-9PMC 7792015 · doi ↗ · pubmed ↗
- 2World Health Organization World malaria report 20212021 Geneva
- 3Dalrymple U Cameron E Arambepola R Battle KE Chestnutt EG Keddie SH The contribution of non-malarial febrile illness co-infections to Plasmodium falciparum case counts in health facilities in sub-Saharan Africa Malar J 2019 Dec 111811953118600410.1186/s 12936-019-2830-y PMC 6560910 · doi ↗ · pubmed ↗
- 4World Health Organization World malaria report 20192017 Geneva
- 5Badmos AO Alaran AJ Adebisi YA Bouaddi O Onibon Z Dada A What sub-Saharan African countries can learn from malaria elimination in China Trop Med Health 2021 Dec 24491863468983910.1186/s 41182-021-00379-z PMC 8542407 · doi ↗ · pubmed ↗
- 6Uganda National Malaria Control Division (NMCD), Uganda Bureau of Statistics (UBOS), ICF Malaria Indicator Survey 2018-192020 Kampala, Uganda
- 7Kamya MR Kakuru A Muhindo M Arinaitwe E Nankabirwa JI Rek J The Impact of Control Interventions on Malaria Burden in Young Children in a Historically High-Transmission District of Uganda: A Pooled Analysis of Cohort Studies from 2007 to 2018 Am J Trop Med Hyg 2020 Aug 510327857923243128010.4269/ajtmh.20-0100 PMC 7410449 · doi ↗ · pubmed ↗
- 8Nambuusi BB Ssempiira J Makumbi FE Kasasa S Vounatsou P The effects and contribution of childhood diseases on the geographical distribution of all-cause under-five mortality in Uganda Parasite Epidemiol Control 2019 May 5e 000893092375310.1016/j.parepi.2019.e 00089 PMC 6424012 · doi ↗ · pubmed ↗