A Case of Intrauterine Listeria Infection During Pregnancy: NanoSuit Imaging of Listeria monocytogenes in the Amniotic Membrane
Chihiro Dohshita, Naomi Isomura, Chizuko Yaguchi, Akira Ohishi, Hiroaki Itoh, Tomomi Kotani, Hideya Kawasaki

TL;DR
A pregnant woman with a Listeria infection led to a cesarean section, and the bacteria were found in the amniotic membrane using advanced imaging.
Contribution
NanoSuit imaging was used to visualize Listeria monocytogenes in the amniotic epithelium during an intrauterine infection.
Findings
Listeria monocytogenes was identified in the neonate and amniotic membrane.
Placental pathology suggested transvaginal rather than hematogenous infection.
NanoSuit imaging provided detailed visualization of the bacteria in the amniotic epithelium.
Abstract
Listeriosis during pregnancy is rare but can lead to premature miscarriage and intrauterine fetal death. A 29-year-old pregnant woman at 29 weeks of gestation was transferred to our hospital because of mild fever and abdominal pain. Emergency cesarean section was performed due to non-reassuring fetal status concomitant with suspected intrauterine infection. An unusually bright yellow amniotic fluid was observed. The oropharyngeal cavity of the neonate was occupied by thick, tenacious yellow mucus, making its removal challenging. The neonate was intubated due to poor oxygenation. Neonatal blood cultures revealed Listeria monocytogenes. Gram staining of cerebrospinal fluid was negative. The neonate was treated and discharged on the 65th day after birth. The mother had a fever of 39.4°C on the first day after surgery; however, no other significant incident occurred. She was discharged on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
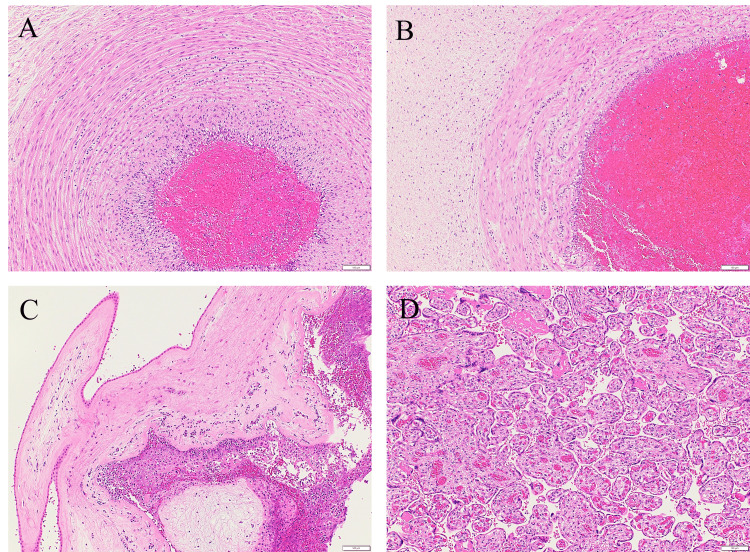 Figure 1
Figure 1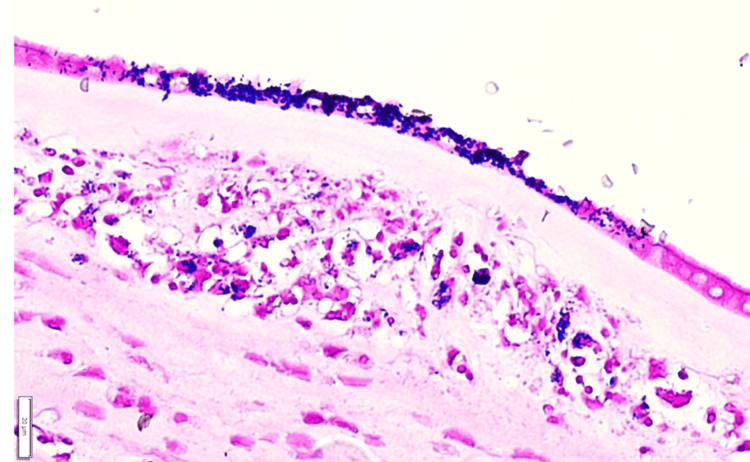 Figure 2
Figure 2 Figure 3
Figure 3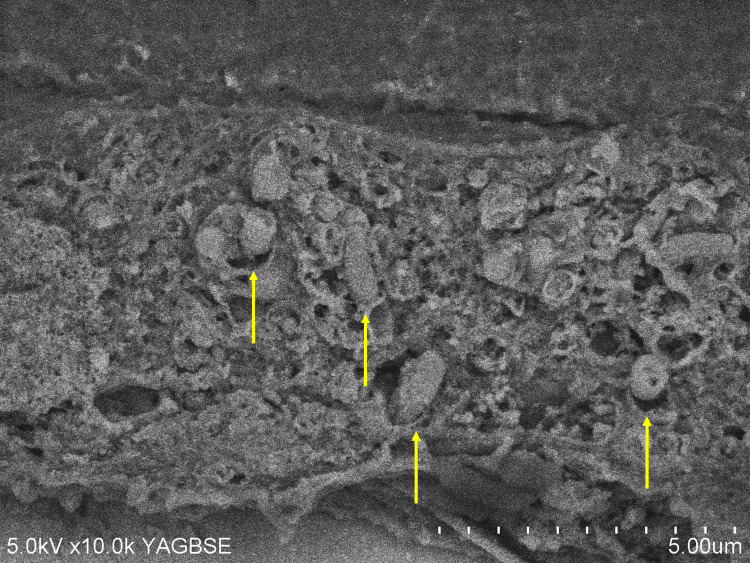 Figure 4
Figure 4| Test parameter | Value | Reference range |
| Hemoglobin | 10.7 | 11.6-14.8g/dL |
| White Blood cells | 19610 | 3300-8600/μL |
| Platelets | 30.2×10⁴ | 15.8-34.8×10⁴/μL |
| C-reactive protein | 9.48 | 0-0.1mg/dL |
| Creatinin | 0.55 | 0.46-0.7mg/dL |
| BUN | 4.7 | 8.0-20.0mg/dL |
| Total bilirubin | 1.23 | 0.4-1.5mg/dL |
| Total protein | 6.2 | 6.6-8.1g/dL |
| Albumin | 3 | 4.1-5.1g/dL |
| A:G retio | 0.94 | 1.32-2.23 |
| LDH | 145 | 124-222U/L |
| ALT | 41 | 7-23U/L |
| AST | 21 | 13-30U/L |
| ALP | 133 | 38-113U/L |
| γ-GTP | 24 | 9-32U/L |
| PT | 13.4 | 10.0-13.0SEC |
| APTT | 35.1 | 24.0-36.0SEC |
| PT-INR | 1.04 | 0.80ー1.20SEC |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsListeria monocytogenes in Food Safety
Introduction
Listeriosis is a zoonosis transmitted by ingestion of foods containing Listeria monocytogenes, a facultative anaerobic Gram-positive rod bacterium. Although listeriosis is rare, its incidence is approximately 13 times higher in pregnant women than in non-pregnant individuals [1]. Iida et al. reported that the number of reported cases of listeriosis has only been about 30 sporadic cases per year in Japan, which has a population of 120 million [2]. Furthermore, Okutani et al. estimated the annual incidence of listeriosis in Japan as 0.65 cases per one million inhabitants [3]. The incubation period can range from a few days to three months, and even mild maternal symptoms may lead to serious outcomes such as fetal growth restriction, fetal dysfunction, or intrauterine fetal death [4]. The present study included NanoSuit-enhanced scanning electron microscopy imaging that identified Listeria monocytogenes in the amniotic membrane epithelium in the case of chorioamnionitis. Herein, we propose a route of transvaginal infection through placental pathology.
Case presentation
A 29-year-old woman, gravida 1 para 0, had a slight fever of 37.7°C and abdominal pain at night at 29 weeks of gestation. She visited her primary care provider the next day. Uterine contractions were observed every two to three minutes, there was bloody vaginal discharge, and the cervical length had shortened to 15 mm. Blood tests revealed inflammatory responses; however, influenza and severe acute respiratory syndrome coronavirus 2 (Sars-CoV-2) antigen tests were negative. She was transported to our hospital. On admission, she was awake and alert, with a body temperature of 37.3°C, pulse rate of 89 beats/min, blood pressure of 124/63 mmHg, respiratory rate of 20 breaths/min, and oxygen saturation of 96% (on room air). She had periodic uterine contractions and lower abdominal pain with a moderate amount of bloody vaginal discharge. Transabdominal ultrasound showed no placental thickening, with the fetus in breech presentation. The estimated fetal weight was -0.4 standard deviations, and the amniotic fluid volume was within the normal range. Blood tests revealed inflammatory responses (Table 1).
In consideration of the maternal signs of infection and indeterminate group B streptococcus status, ampicillin was administered as the initial empirical antibiotic. An emergency cesarean section was performed based on a diagnosis of non-reassuring fetal status from fetal heart rate monitoring, concomitant with a possible intrauterine infection. During the operation, an unusually bright, clear lemon color amniotic fluid was observed. After delivery, oxytocin and methylergometrine were administered for poor uterine contractions. Blood loss was 2,400 g. After surgery, the antibiotic was changed to cefazolin sodium in accordance with the perioperative antibiotic guidelines in the hospital. On the first day after surgery, hemoglobin (Hb) was 7.2 g/dL. We administered ferric carboxymaltose 500 mg. Skin and blood cultures from the neonate, as well as placental scraping cultures, were positive for Listeria monocytogenes. As a result, the antibiotic regimen was switched to sulbactam/ampicillin. The mother had a fever of 39.4°C on the first day after surgery; however, no other significant incident occurred. After changing to oral antibiotics, she was discharged on the 10th day after surgery. Maternal blood, fecal, urine, and vaginal cultures were all negative.
The newborn weighed 1366 g (0.0 standard deviations), had an Apgar score of 1/1 (one minute/five minutes), and an umbilical artery blood pH of 7.331. The oropharyngeal cavity of the neonate was occupied by thick, tenacious yellow mucus, making its removal challenging. Artificial respiration was initiated due to respiratory distress, and intubation was required because of bradycardia. Gradually, the patient’s heart rate increased, and SpO2 reached 100%. Mechanical ventilation with inhaled nitric oxide was started for pulmonary hypertension. Platelet count was 60,000/μl, and blood transfusion was initiated. Polyethylene glycol-treated human immunoglobulin was administered, and empirical antibiotic therapy was initiated with Ampicillin and cefotaxime. On the second day, the newborn was extubated. Blood cultures became negative on the second day after birth. Gram staining of cerebrospinal fluid was negative. The neonate was discharged on the 65th day after birth. Pathological examination by H&E staining showed massive neutrophil infiltration around the umbilical vessels, extending to Wharton’s jelly (Figures 1A, 1B), chorioamnion, and the decidual side of the marginal placental membrane(Figure 1C), but not in the villi (Figure 1D).
Placental pathological findings (H&E staining: scale bar 100μm)A: Umbilical artery - neutrophil infiltration extending into the muscular layer of the vascular wall, B: Umbilical vein - neutrophil infiltration extending to Wharton’s jelly, C: The infiltration of numerous neutrophils is observed on the decidual side of the marginal placental membrane, D: Neutrophil infiltration is not observed in the placental villi.
Gram stain findings were positive in the amniotic epithelium (Figure 2).
Amniotic epithelium was found to be Gram stain positiveGram stain findings (scale bar; 20μm).
Immunohistochemical staining for Listeria monocytogenes showed positive staining in the amniotic epithelium (Figure 3A), but not in the villi (Figure 3B).
Immunohistochemical staining of Listeria monocytogenesAnti-Listeria antibody: abcum:ab35132 (scale bar; 50μm).A: Positive (brown) is observed in the amniotic epithelium, B: Positive staining of Listeria monocytogenes is not observed in the placental villi or intervillous spaces.
Moreover, scanning electron microscopy with NanoSuit, performed according to the methodology of a previous study [5,6], revealed numerous Listeria monocytogenes within the amniotic epithelium (Figure 4).
NanoSuit-assisted scanning electron microscopy reveals Listeria monocytogenes in the amniotic membrane epitheliumNumerous bodies of Listeria monocytogenes (yellow arrows) are observed in the amniotic epithelium.
The NanoSuit method enabled live observation of fly larvae under a high-vacuum scanning electron microscope (SEM). By simply applying the NanoSuit solution, the tissue retains its hydration and original structure, allowing for clear SEM imaging without the need for traditional fixation or dehydration. Performed immunohistochemical staining for Listeria on formalin-fixed, paraffin-embedded sections. Captured images of the 3,3'-diaminobenzidine (DAB)-positive Listeria-stained areas under a light microscope, and marked these areas on both the front and back of the slide using a solvent-resistant pen. By incubating the slide glass, after immunostaining, in a 1% osmium solution for five minutes, the osmium will bind specifically to DAB, enhancing DAB-positive regions for SEM observation. After rinsing with water three times for five minutes each, apply 200 μL of NanoSuit Solution Type II (NanoSuit Co., Japan) onto the slide glass. Then, using a spin coater set at 3000 rpm, thinly spread the NanoSuit solution over the tissue. Field emission scanning electron microscopy (SEM) was performed using a Hitachi S-4800 Field Emission Scanning Electron Microscope instrument (Hitachi High-Technologies Corporation, Japan) operated at an acceleration voltage of 5kV. The backscattered electron (BSE) image was taken using a Yttrium-Aluminium-Garnet (YAG)BSE detector (Hitachi High-Tech Corporation, Tokyo, Japan). The immunohistochemically positive region that had been previously observed was identified on the SEM image.
Discussion
Listeria sp. is widely distributed in the environment, including river water and the intestines of animals. Although it is inactivated by heating, it is capable of proliferating even at temperatures below 4°C and in environments with a concentration of up to 12% sodium chloride. Identified sources of infection include ready-to-eat foods that are typically consumed without prior heat treatment, such as dairy products (including natural cheese), processed meats (such as raw ham), seafood products (such as smoked salmon), and prepared foods (such as deli salads and coleslaw) [7,8]. Therefore, it is advised for pregnant women to wash raw vegetables and fruits, store food in the refrigerator, consume products before the expiration date, and adequately heat food before ingestion [7,8]. In the present case, maternal dietary history and preferences obtained via interview revealed no consumption of unpasteurized dairy products or uncooked processed meats. A causative food item could not be identified. Typical symptoms of maternal listeriosis include influenza-like manifestations, such as chills, fever, and myalgia, with the potential for progression to sepsis, meningitis, or central nervous system symptoms [7]. There are also reports of laboratory findings resembling HELLP syndrome, including fever, hemolysis, elevated liver enzymes, and thrombocytopenia. Therefore, febrile nonspecific symptoms during pregnancy should prompt consideration of infectious etiologies [4].
Although this case initially appeared to be a typical intrauterine infection presenting with preterm labor and fetal compromise, certain unique findings were noted. Specifically, the amniotic fluid had a vivid lemon-yellow coloration, and the neonate exhibited highly viscous sputum in the oral cavity. It was speculated that the fetus led to pneumonia and resulting airway secretions, which were the cause of oral obstruction and yellow amniotic fluid. To the best of our knowledge, this color finding has not been previously reported.* Listeria* infection typically results from ingestion of contaminated food and spreads hematogenously across the placenta from the maternal gastrointestinal tract to the fetus; on the other hand, an alternative ascending route from the vagina, via contaminated feces, has also been reported [7]. In the present case, Listeria monocytogenes was isolated from neonatal blood, stool, pharyngeal, and otorrhea cultures, as well as from swab cultures of the placental surface. However, maternal vaginal discharge and blood cultures were negative. Placental pathology of Listeria infection shows a light yellow microabscess on gross appearance and acute villitis with abscesses on microscopic appearance [9]. This case's histopathological examination of the placenta did not reveal findings typical of transplacental infection, such as intervillositis or villitis (Figures 1D, 3B). Neutrophilic infiltration was predominantly observed in the decidua at the marginal zone of the fetal membrane, near the internal cervical os, which had ruptured during the cesarean section (Figure 1C). Immunohistochemical staining using an anti-Listeria antibody showed positivity only in the amniotic epithelium (Figure 3A). Furthermore, scanning electron microscopy with the NanoSuit method clearly revealed numerous* Listeria monocytogenes* organisms in the amniotic epithelium (Figure 4). No neutrophil infiltration or Listeria immunostaining positivity was observed in the placental villi (Figures 1D, 3B). These findings strongly suggest that the infection was caused by ascending transmission of Listeria monocytogenes from the vagina, following fecal contamination; thus, it is a case of transvaginal infection. However, we have no clear explanation of the negative Listeria monocytogenes findings from the vaginal discharge.
A retrospective study of Listeriosis, which used an electronic and manual retrieval system (2008-2017), reported that 89% of maternal cases involved intrauterine Listeria infection in mainland China. The total of 514 cases that occurred in the perinatal period consisted of 116 pregnant women and 398 neonates. Among pregnant women, 103 patients had intrauterine infections (89%), in all of which only* Listeria* was isolated from the cervical secretions [10]. The most sensitive diagnostic tests for pregnancy-related Listeriosis are placental swab cultures and neonatal gastric aspirate cultures, both of which demonstrate a sensitivity of 78%. In contrast, a previous study reported that maternal blood cultures were positive for* Listeria* monocytogenes in only 33-68% of cases [8]. Severe maternal illness due to Listeria is rare, and most cases resolve without antibiotic treatment. Among neonates with pregnancy-associated listeriosis, 62-72% develop bacteremia, 9-13% develop pneumonia, and 13-19% develop meningitis. The neonatal mortality rate ranges from 9-50%, and up to 13% of surviving infants develop neurological sequelae [11]. Regardless of the manifestation of non-reassuring fetal status, when intrauterine infection is suspected during pregnancy, performing maternal bacterial and/or placental swab cultures may improve the diagnostic yield.
Conclusions
Although it is a rare condition, Listeria monocytogenes infection may result in severe consequences for the fetus during pregnancy. In cases of preterm labor associated with intrauterine infection,* Listeria* should be considered as a possible etiology. Detailed interviews about the maternal environment, preferences, and dietary history, along with proactive bacterial cultures from both the mother and neonate, are recommended. Placental histopathological examination may also provide insights into the route of infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An update review on listeria infection in pregnancy Infect Drug Resist Wang Z Tao X Liu S Zhao Y Yang X 196719781420213407930610.2147/IDR.S 313675 PMC 8165209 · doi ↗ · pubmed ↗
- 2Detection of Listeria monocytogenes in humans, animals and foods J Vet Med Sci Iida T Kanzaki M Nakama A Kokubo Y Maruyama T Kaneuchi C 13411343601998987953610.1292/jvms.60.1341 · doi ↗ · pubmed ↗
- 3Overview of Listeria monocytogenes contamination in Japan Int J Food Microbiol Okutani A Okada Y Yamamoto S Igimi S 1311409320041513595210.1016/j.ijfoodmicro.2003.11.014 · doi ↗ · pubmed ↗
- 4Listeriosis in pregnancy: a rare but high-risk infection Cureus Correia de SáA Casanova D Ferreira AL Fernandes C Cotter J 015202310.7759/cureus.47748 PMC 1067626838021504 · doi ↗ · pubmed ↗
- 5The Nano Suit method: a novel histological approach for examining paraffin sections in a nondestructive manner by correlative light and electron microscopy Lab Invest Kawasaki H Itoh T Takaku Y 16117310020203146742410.1038/s 41374-019-0309-7PMC 6917571 · doi ↗ · pubmed ↗
- 6Identifying active progeny virus particles in formalin-fixed, paraffin-embedded sections using correlative light and scanning electron microscopy Lab Invest Itoh T Yamada S Ohta I 10002010320233674819510.1016/j.labinv.2022.100020 · doi ↗ · pubmed ↗
- 7Human listeriosis Clin Microbiol Rev Koopmans MM Brouwer MC Vázquez-Boland JA van de Beek D 036202310.1128/cmr.00060-19PMC 1003564836475874 · doi ↗ · pubmed ↗
- 8Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study Lancet Infect Dis Charlier C PerrodeauÉ Leclercq A 5105191720172813943210.1016/S 1473-3099(16)30521-7 · doi ↗ · pubmed ↗