Significant Hair Regrowth With 5% Topical Minoxidil in a Child With Marie Unna Hereditary Hypotrichosis Caused by a Recurrent HRURF Variant
Can Cui, Xi Chen, Ying‐Zi Zhang, Jin‐Yuan Ma, Ai‐Hua Wei

Abstract
Click any figure to enlarge with its caption.
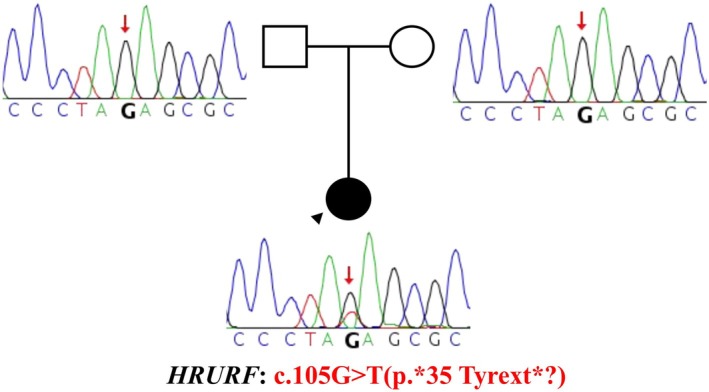 FIGURE 1
FIGURE 1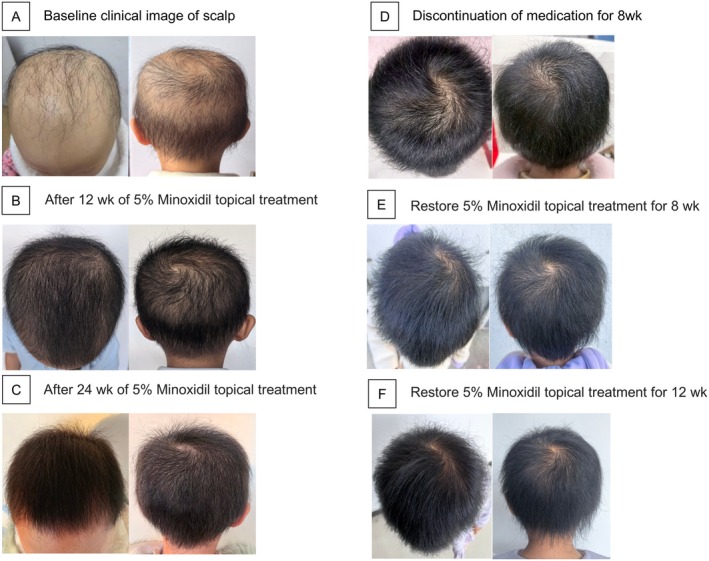 FIGURE 2
FIGURE 2- —National Natural Science Foundation of China10.13039/501100001809
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHair Growth and Disorders · melanin and skin pigmentation · Skin and Cellular Biology Research
To the Editor,
Introduction
1
Marie Unna hereditary hypotrichosis (MUHH) is a rare autosomal dominant disorder first described in 1925 [1]. Affected individuals typically present at birth with sparse or absent scalp hair, eyebrows, eyelashes, and body hair. In 2009, HRURF was identified as the causative gene for MUHH1 [2]. Currently, no targeted therapy is available.
Case Report
2
A 4‐year‐old girl presented with congenital hypotrichosis. At birth, her scalp hair was sparse and shed within the first 3 months. Hair regrowth was minimal, never exceeding 5 cm in length. She was born at term via spontaneous vaginal delivery with normal development. Her father had androgenetic alopecia, and her mother had a normal hair phenotype. There was no consanguinity or family history of similar conditions.
Physical examination revealed diffuse, fine, slightly curled scalp hair with androgenetic distribution. Eyelashes were thin and curled, and eyebrows were nearly absent. A widened midline diastema was noted. No abnormalities were observed in skin, nails, or other systems. After obtaining written informed consent, peripheral blood samples were collected from the patient and both parents. Whole‐exome sequencing identified a de novo stop‐loss variant in HRURF (c.105G > T, p.35Tyrext?), confirmed by Sanger sequencing. Both parents were wild‐type. The patient was diagnosed with MUHH1 (Figure 1).
Genetic analysis of the HRURF variant: Sanger sequencing confirmed a de novo HRURF stop‐loss variant (c.105G > T, p.35 Tyrext?) identified by whole‐exome sequencing.
Given strong parental interest, topical 5% minoxidil was initiated once daily to the scalp (solution for 4 weeks). The parents later switched to the foam formulation without medical instruction, and no adverse effects were reported. After 12 weeks, significant scalp hair regrowth was observed, with improved density and no reported irritation or hypertrichosis. At 6 months, scalp hair density further improved. Treatment was discontinued for 8 weeks, during which minimal hair breakage was noted. Hair length increased slightly, but density plateaued. Upon observing breakage, treatment was resumed. After 8 weeks of re‐initiation, hair density increased, and by 12 weeks, hair length exceeded 10 cm (Figure 2).
Clinical progression of scalp hair growth and response to 5% Minoxidil topical treatment. (A) Baseline clinical image of scalp before treatment. (B) Scalp appearance after 12 weeks of 5% Minoxidil application. (C) Scalp appearance after 24 weeks of 5% Minoxidil application. (D) Scalp appearance following 8 weeks of discontinuation of medication. (E) Scalp recovery after restarting 5% Minoxidil treatment for 8 weeks. (F) Scalp improvement after resuming 5% Minoxidil treatment for 12 weeks.
Discussion
3
Over 25 pathogenic variants in HRURF have been identified in MUHH1 [3]. We identified a recurrent stop‐loss variant in HRURF (c.105G > T, p.35Tyrext?), previously reported in a Danish family, which may convert the normal stop codon into a tyrosine codon, potentially extending the open reading frame and elongating the HRURF protein [3]. In the Danish family, the mother carrying the same variant had sparse, curly, and frizzy hair at birth, but her hair density and appearance normalized in adulthood. However, her two children with the same variant presented with congenital hypotrichosis. In our case, the patient showed significant hair regrowth after topical minoxidil treatment. Whether this improvement will persist or resemble the natural course observed in the Danish mother requires further follow‐up. Nevertheless, the marked short‐term efficacy supports the potential benefit of topical minoxidil in such cases.
Evidence for treating congenital hypotrichosis remains limited. Minoxidil promotes anagen entry and prolongs follicular activity, enhancing hair density and diameter. Topical 5% minoxidil has been used in children as young as 2 years, though hypertrichosis is a known side effect [4]. Case reports have demonstrated its potential to improve hair density in monilethrix patients with KRT86 mutations without notable adverse effects [5]. In a recent case report, an 8‐year‐old boy with CDSN‐related hypotrichosis simplex of the scalp (HSS) received a combination of topical 5% minoxidil and botanical extracts. After 4 months of treatment, marked clinical improvement was observed, with a reported 70% increase in hair density at 6‐month follow‐up [6]. While long‐term safety remains uncertain, minoxidil may serve as a symptomatic option in selected pediatric patients under close supervision.
Conclusion
4
This case demonstrates that 5% topical minoxidil may be effective in improving hair density in patients with MUHH. The clinical response suggests potential benefit even in congenital, genetically driven hair loss. Combined with previous reports on monilethrix and hypotrichosis simplex, our findings support expanding the use of minoxidil in rare hereditary alopecias. Early intervention and individualized treatment approaches may offer improved outcomes for these otherwise treatment‐refractory conditions.
Author Contributions
Ai‐Hua Wei conceived and supervised the study; Jin‐Yuan Ma, Ying‐Zi Zhang, and Can Cui analyzed data; Can Cui wrote the manuscript; Xi Chen made manuscript revisions. All authors reviewed the results and approved the final version of the manuscript.
Consent
Written patient consent for publication was obtained.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. Redler , R. Kruse , S. Eigelshoven , et al., “Marie Unna Hereditary Hypotrichosis: Identification of a U 2HR Mutation in the Family From the Original 1925 Report,” Journal of the American Academy of Dermatology 64, no. 4 (2011): e 45–e 50.20659777 10.1016/j.jaad.2010.06.013 · doi ↗ · pubmed ↗
- 2Y. Wen , Y. Liu , Y. Xu , et al., “Loss‐of‐Function Mutations of an Inhibitory Upstream ORF in the Human Hairless Transcript Cause Marie Unna Hereditary Hypotrichosis,” Nature Genetics 41, no. 2 (2009): 228–233.19122663 10.1038/ng.276 · doi ↗ · pubmed ↗
- 3S. Holm , L. Graversen , A. K. W. Simonsen , J. Blechingberg , L. K. Herlin , and K. Rønholt , “Clinical Presentation of a Family Diagnosed With Marie Unna Hereditary Hypotrichosis 1 Caused by a Novel Variant in HRURF,” Pediatric Dermatology, Ahead of Print, 2025.10.1111/pde.15982 PMC 1264697740433810 · doi ↗ · pubmed ↗
- 4I. Herskovitz , J. Freedman , and A. Tosti , “Minoxidil Induced Hypertrichosis in a 2 Year‐Old Child,” F 1000 Research 2 (2013): 226.24555107 10.12688/f 1000 research.2-226.v 1PMC 3886784 · doi ↗ · pubmed ↗
- 5Q. Shen , Z. Fu , P. Du , and J. Wang , “Gene Detection in a Family With Monilethrix and Treatment With 5% Topical Minoxidil,” Skin Research and Technology: Official Journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI) 29, no. 1 (2023): e 13233.10.1111/srt.13233 PMC 983876336382623 · doi ↗ · pubmed ↗
- 6W. M. Ramadan , A. M. Hassan , E. E. El‐Hawary , and N. S. Gomaa , “Successful Treatment of Hereditary Hypotrichosis Simplex by Platelet Rich Plasma Injection With Topical Minoxidil 2,” Journal of Dermatological Treatment 34, no. 1 (2023): 2169575.36651821 10.1080/09546634.2023.2169575 · doi ↗ · pubmed ↗